
Abstract
Abstract
Introduction:
The aim of this study was to assess retrospectively the results of laparoscopic cholecystectomy (LC) performed in obese patients at our institution with the traditional technique and with the fundus-first (FF) technique.
Patients and Methods:
We performed a retrospective analysis of 194 obese patients that underwent LC between 1994 and December 2007 at our institution. Surgical techniques were compared with respect to operative times, conversion to open cholecystectomy, postoperative complications, mortality, and length of postoperative stay.
Results:
In the reviewed period, LC was performed in 113 (58.2%) patients with obesity type I (OTI), 55 (28.3%) patients with obesity type II (OTII), and 26 (13.5%) patients with obesity type III (OTIII). None of the differences among obese groups treated with the two techniques were statistically significant, with the exception of the lower operative times in the OTIII patients treated with the FFLC. The median operating time in the OTIII group was, respectively, 90 minutes for traditional LC and 65 (range, 45–130) for FFLC (P < 0.05).
Discussion and Conclusions:
This study achieved to conclude that LC in the obese is a safe, feasible, and efficient operation, but remains a demanding procedure even in experienced hands. FFLC can support the traditional LC in the treatment of obese patients, yielding a complication rate comparable with the traditional technique. In our study, it significantly reduced the operative time in OTIII patients, simplifying all the intra-abdominal maneuvers and the gallbladder dissection.
Introduction
Patients and Methods
A computerized database was analyzed retrospectively for 2346 consecutive cases of the LC performed for gallbladder disease in two community hospitals: San Martino Hospital (Oristano, Italy), from January 1994 to December 2001, and Sant'Elena Clinic (Cagliari, Italy), from January 2002 to December 2007. Patients were divided into three main groups: obesity type I patients (OTI) defined as a body mass index (BMI) between 30 and 35 kg/m2; obesity type II patients (OTII) defined as a BMI between 35 and 40 kg/m2; and obesity type III patients (OTIII) defined as a BMI >40 kg/m2. Indications for LC are shown in Table 1. Acute cholecystitis was defined by the presence of fever, right-upper quadrant pain, elevated leukocyte count (i.e., white blood cell >104/mmc), and signs of inflammation on gallbladder ultrasound. Inflammatory status of the gallbladder was classified according to the grading system proposed by Chang. 14 Preoperative magnetic resonance cholangiopancreatography (MRCP) and endoscopic retrograde cholangiopancreatography (ERCP) were performed in selected cases, when clinically indicated. When common bile duct (CBD) stones were discovered, endoscopic sphincterotomy was performed and ductal clearance achieved before surgery. Prophilaxis against deep venous thrombosis was provided in the form of elastic stockings plus a low-molecular weight-heparin (Fluxum®; Alfa Wassermann, Bologna, Italy). One gram of ceftazidime (Spectrum®; Sigmatau, Roma, Italy) intravenously (i.v.) was given at the time of induction of anesthesia or clarythromicin (Klacid®; Abbott, Latina, Italy) 500 mg i.v. if sensitive to penicillin. Type of surgical procedure, conversion to OC, and complications were compiled. Operation time, admission to intensive care unit (ICU), length of hospital stay after operation, and milligrams of analgesics used (Ketorolac, Toradol®; Recordati, Milano, Italy) were recorded. Patients were usually discharged after 48 hours of observation. All patients were seen in the outpatient department at 1 and 6 weeks and, finally, at 12 months. Statistical analysis was performed by using the chi-square test for categoric variables and the Mann-Whitney U test for continuous variables. Probabilities (P-value) less than 0.05 were considered significant.
OTI, obesity type I patients; OTII, obesity type II patients; OTIII, obesity type III patients; ns, not significant.
Technique
LC in both obese groups was performed by using a four-trocar approach,1,2,15 unlike that used in NW patients, in which we routinely performed a three-trocar approach. 16 The pneumoperitoneum was most commonly induced by performing an open supraumbilical incision at a variable distance from the umbilicus, usually comprised between 5 and 10. The pneumoperitoneum was always maintained at an insufflation pressure of ≤14 mm Hg. The primary camera port was usually placed in the supraumbilical port. The patient was then placed in the 30-degree reverse Trendelenburg position and rotated to the left. Under direct vision, a dynamic retraction port was placed in the right subcostal position conventionally used for the Reddick-Olsen technique. 15 The third 10-mm trocar was usually placed midway between the umbilicus and the xyphoid process, 2–3 cm to the left of the midline, and it was used for the passage of the coagulating hook, stapler, scissors, and aspirator. After the inspection of the abdominal cavity and a preliminary exposition of the Calot's triangle, the next step was the insertion of the fourth trocar. It was placed in the epigastric region in cases of enlarged livers or left-lobe hypertrophy. In cases with a large amount of omental fat or prominence of the colon or duodenum, an additional subcostal port was placed laterally to the dynamic retraction port. The rest of the procedure was then carried out with the identification of the cystic duct and the cystic artery at Calot's triangle and their subsequent division between clips. Anterograde dissection of the gallbladder from the liver was accomplished by using a monopolar electrocautery. In the attempt to reduce intraoperative times and to easily perform LC, from January 2006, we routinely adopted in obese patients the FFLC.17–21 Up to then, we had been performing FFLC only in NW patients who otherwise had to be submitted to an open operation because of a very difficult anatomy at the Calot's triangle. 22 We did not use FFLC in obese patients until we had become comfortable with the technique in NW patients.
Results
During the review period, 194 consecutive cases of LC were performed in obese patients for gallbladder disease. LC was performed respectively in 113 (58.2%) OTI patients, 55 (28.3%) OTII patients, and in 26 (13.5%) OTIII patients. In this group, 55 (68%) were O patients, and 26 (32%) were MO patients. The male-to-female ratio was 1:3, and the average age was 52 years (range, 38–74). Indications for LC in these series are shown in Table 1. The number of interval cholecystectomies was significant higher in the OTIII, compared to OTI and OTII, groups (P < 0.05). Results of LC are showed in Table 2. Cholecystectomy was succesfully completed laparoscopically in the OTI group in 110 (97%) patients, in the OTII group in 53 (96%) patients, and in the OTIII group in 23 (88.4%) patients. The median operating time for the traditional LC was 55 (range, 36–195) in the OTI group, 70 (range, 40–190) in the OTII group, and 95 minutes (range, 66–240) in the OTIII group. In this last group, the operative time was significantly longer than that in the other two groups (P < 0.05) either in the setting of chronic or acute colecystitis. The median operating time for the FFLC was 62 (range, 45–185) in the OTI group, 55 (range, 40–110) in the OTII group, and 65 minutes (range, 45–130) in the OTIII group. The difference between OTIII groups treated with the traditional LC and with FFLC was significant (P < 0.05) either in the setting of chronic or acute colecystitis.
*P < 0.05; **P < 0.05.
OTI, obesity type I; OTII, obesity type II; OTIII, obesity type III; LC, laparoscopic cholecystectomy; FFLC, fundus-first laporoscopic cholecystectomy; OC, open conversion; CBD, common bile duct; pt, patient(s).
In 8 patients (4%), LC was eventually converted to the open operation (Table 3). In these failed cases, an average of 26 minutes (range, 20–58) of laparoscopic surgery occurred in the OTI group before being converting to OC, while an average of 35 (range, 30–70) and 36 minutes (range, 10–85) occurred, respectively, in the OTII and OTIII groups. The conversion rate was, respectively, 3% (3 patients) for the OTI group, 4% (2 patients) for the OTII group, and 11.6% (3 patients) for the OTIII group. No conversions occurred with the FFLC. Unclear anatomy due to dense adhesions was the cause for conversion in 2 patients in both the OTI and OTII groups and in 1 patient in the OTIII group (Table 3). Inability to safely maintain the pneumoperitoneum due to severe hypercapnia occurred in 1 patient with a BMI of 42. No patient required a conversion due to intraoperative complications. None of the patients were admitted to the ICU after surgery or needed extra postoperative support of mechanical ventilation. Analgesics were not needed after 48 hours.
Interval cholecystectomy.
OTI, obesity type I; OTII, obesity type II; OTIII, obesity type III.
No CBD injuries occurred in this series. Minor complications were represented by 2 (1%) postoperative periumbilical port infections, treated with antibiotic therapy. Six (3%) patients had postoperative periumbilical port hematomas that were promptly drained. Postoperative bile leaks through the subcostal drain were seen in 1 patient in the MO group treated with the traditional technique and persisted for a few days without any clinical manifestations. The leak was managed with i.v. fluids and antibiotics. There was no statistical difference between groups treated with the traditional technique or with the FFLC. The average postoperative hospital stay for both techniques is shown in Table 2. Mortality rate was nil. Follow-up was satisfactory in all cases.
Discussion
Demographic studies show a dramatic increase in the prevalence of obesity in Western countries. 23 Open abdominal surgery in these patients is usually associated with an increased rate of non-procedure-related complications (e.g., pulmonary, cardiovascular, urinary, and wound infections).24–26 The introduction of laparoscopic surgery has undoubtedly led to a drastic reduction of postoperative complications in these patients, supporting LC as the gold standard in the treatment of benign gallbladder diseases.3–10,27–29 Nonetheless, obesity has a not negligible effect on the technical feasibility of the LC. Technically demanding cases are still at high risk for conversion and postoperative complications, thus eliminating the advantages of the laparoscopic procedure. Although steadily increasing in recent years also in our region, obese patients still represent a small portion of our patient population. The aim of this study was to compare LC and FFLC in the treatment of our obese patients in order to evaluate the safety, efficacy, and feasibility of the two different laparoscopic techniques.
On the one hand, this study clearly shows the feasibility, efficacy, and safety of the LC in obese patients. It can be performed routinely in the obese population for the treatment of acute and chronic gallbladder disease with, overall, low conversion rates (4.6% in this series), low complication rates (0% of major complications), and a shorter hospital stay. On the other hand, our experience also confirms that reasonable concerns expressed by some surgeons over the potential difficulties during LC in obese patients are still justified.27,28 The large size of these patients compels the surgeon to constantly adapt the laparoscopic technique in order to perform a safe operation and avoid conversion to OC. 5 Surgical technique must be tailored on every specific case and must rely upon precise technical details and standardization of the procedures to maintain high safety standards.
The exposure of the structures at the Calot's triangle in obese patients can be, in fact, very difficult also in patients with a local normal anatomy for several reasons. The working space in these patients can be drastically reduced by the presence of an abundant abdominal wall or a large amount of intra-abdominal fat. The surgeon may be compelled to use higher levels of intra-abdominal pressures (>14 mm Hg) in order to hold up the thick abdominal wall and thus maintain an adequate working space. This strategy is not without risk in consideration of the hemodynamic modifications due to pneumoperitoneum induction and to the limited cardiopulmonary reserves in most of the morbid obese patient 26 and should be used only in cases of proven necessity. The inability to safely maintain an adequate pneumoperitoneum was the reason for conversion to OC in 1 OTIII patient of this series. In fact, if the pneumoperitoneum cannot be safely, efficiently maintained because of an ongoing risk of a cardiopulmonary failure, a prompt conversion to OC is warranted.
In obese patients, the depth of the subcutaneous fat may determine an excessive distance between the laparoscopic instruments and the surgical field, and a reduced mobility of instruments themselves in the dissection maneuvers.3,5,9,27,30 A prominent costal arch can often eliminate the advantage of a more cephalad location of all those ports useful for the upward traction of the gallbladder. In fact, due to the presence of a rigid rib cage, the pneumoperitoneum can determine a modification of the superior abdominal compartment, transforming it from an oval-shaped cavity (Fig. 1) to an hourglass-shaped one (Fig. 2). This anatomic condition determines a further reduction of the working space and may worsen the mobility of surgical instruments. Nonetheless, the operative field being localized at this hypothetic bottleneck, it is not infrequent for an instrument to be “crowding” with resulting clumsy, unsafe manipulations of the anatomic structures. These anatomic containments, together with the possibility of modified anatomic findings at Calot's triangle, can make LC a technically demanding, time-consuming procedure in obese patients, even in experienced hands. Prolonged operative times, especially in OTIII patients, usually reflects the encountered technical difficulties in the induction of pneumoperitoneum and in the dissection of the relevant structures at the Calot's triangle.

Shape of the superior abdominal compartment after the induction of the pneumoperitoneum in a patient with BMI <29.
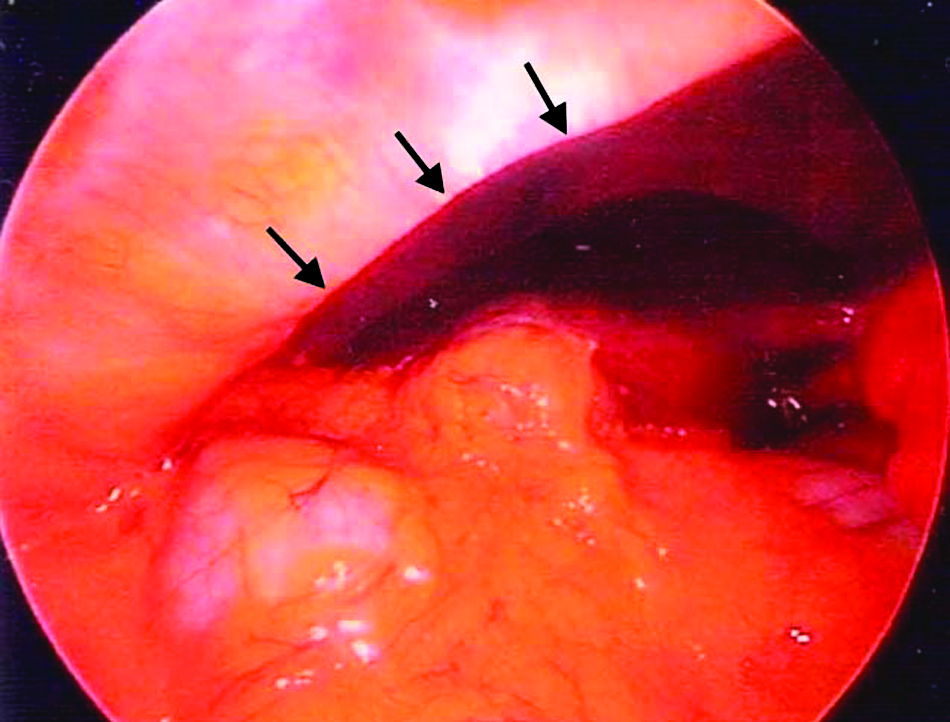
Shape of the superior abdominal compartment after the induction of the pneumoperitoneum in a patient with BMI >35. Due to the presence of a rigid rib cage, the pneumoperitoneum can determine a modification of the superior abdominal compartment, transforming it from an oval-shaped cavity to a hourglass-shaped one. The resulting prominent costal arch (arrows) may limit the upward traction of the liver and gallbladder.
In the attempt to overcome these technical problems and reduce operative times and conversion rates, always maintaining high safety standards, from 2006, after a 10-year judicious use in difficult cholecystectomies in NW patients, we decided to introduce FFLC in patients with BMI >30. The FF technique, starting the dissection from the gallbladder fundus,17–22 and keeping it close to the gallbladder wall until the Calot's structures are clearly identified and sectioned, offers the advantage of providing an adequate exposure of the ductal system at the Calot's triangle, exerting progressive tractions on the biliary structures. In our experience, FFLC resulted in being extremely useful in OTIII patients to overcome the limitations imposed by the depth of the abdominal wall and by a pronent costal arch, because it allowed the exposition of the operative field by exerting only a mild upward traction on the liver and gallbladder. In obese patients, especially those with severely inflamed gallbladders, and/or with an enlarged liver, 22 the upward traction of the gallbladder-liver complex may be, in fact, an important limiting factor when the traditional laparoscopic technique is used. In these cases, the FF technique was effective in achieving a right-upward traction of the liver and the manipulation of the hepatic undersurface in a reduced working space. Moreover, avoiding heavy tractions and manipulations of the hepatic undersurface in patients with a steatosic liver reduced the possibility of hepatic trauma with the resulting tedious bleeding. In our experience, the FFLC made easier the manipulations of all the structures involved in the dissection, reducing significantly the operative times in OTIII patients, when compared to the traditional technique. We did not find any significant difference of operative times in OTI and OTII patients treated with the two techniques, with the exception of a subgroup of patients who underwent an interval cholecystectomy.
The high number of interval cholecystectomies in obese patients, especially those with OTIII, reflects the tendency of some surgeons to indefinitely postpone surgery in the erroneous belief that a delayed LC in a less inflammatory environment may reduce the conversion rate to OC. But, the conditions of the gallbladder, after one or more previous episodes of acute cholecystitis, may be more important than the acute inflammatory environment in determining a conversion to OC. 31 Patients with a prolonged interval from onset of symptoms to diagnosis are at higher risk for conversion to OC than patients who undergo early surgery. In this series, in most of these patients with acute cholecystitis, an early operation allowed the identification of the relevant structures at the Calot's triangle and their safe management. On the contrary, in a delayed approach, the presence of a thickened gallbladder, with dense adhesions associated with abundant steatonecrosis, typical of these patients, makes the dissection of Calot's structures unsafe. In these conditions, dissection of the Calot's triangle may result in being very difficult and time consuming, especially when the traditional laparoscopic technique is used.32–34 With this technique, the difficulty to achieve a sufficient exposition of relevant structures in a reduced space, and the dissection in a scarred cystic pedicle, may determine prolonged operative times with high conversion rates of the LC to OC. FFLC resulted as useful also in these cases, allowing a progressive and good exposition of the operative field, thus facilitating the dissection manuvers and reducing operative times.
Conclusions
This study, although with all the inherent limitations that apply to the nature of a retrospective design (e.g., lack of control of variables that could have had an impact on patient and physician outcomes), achieved to conclude that LC in the obese is a safe, feasible, and efficient operation, but remains a demanding procedure even in experienced hands. FFLC can safely support the traditional LC in the treatment of obese patients, yielding a complication rate comparable with the traditional technique. In our study, it significantly reduced the operative times in OTIII patients, simplifying all the intra-abdominal maneuvers and the gallbladder dissection.
Footnotes
Acknowledgment
Supported by: Clinica Sant'Elena, Quartu Sant'Elena, Cagliari, Italia.
Disclosure Statement
No competing financial interests exist.