
Abstract
Abstract
Background:
There have been descriptions of several techniques for congenital inguinal hernia (CIH) repair in the pediatric population by doing high ligation of the sac, without a definitive advantage over the open procedure. High recurrence rates have been reported with using these minimally invasive techniques in which the patent processus vaginalis has been ligated and left in place completely or partially.
Methods:
With approval of the ethics committee, a proper informed consent was obtained. During July 2003 to April 2008, we performed the inguinal hernia repair on 91 patients (76 males and 15 females), using a laparasocopic technique in which we completely resected the patent processus vaginalis and the parietal peritoneum surrounding the internal inguinal ring. This allowed the peritoneal scar tissue to close the area of the ring. Also, this scarring occurs in the extent of the inguinal canal where the dissection took place, therefore causing the same peritoneal scarring and sealing of the inguinal floor. In this series, a purse string was done only in the cases with an internal ring wider than 10 mm.
Results:
There were no conversions. Operative time was in the range of 35–72 minutes (average, 40). Close follow-up in the clinic has been 5 months to 4 years without a single recurrence. In 4 cases, 3 months later, we did a laparoscopic evaluation of the contralateral side due to associated cryptorchidism, in which we were able to confirm a complete closure of the interior inguinal ring. Two small hematomas were followed until they were gone, without further need for intervention.
Discussion:
No recurrences have been observed. We conclude that laparoscopic repair of CIH is feasible using this technique of complete resection of the processus vaginalis and surrounding parietal peritoneum. This series does not conclude on the need for the internal ring to be closed when found to be wider than 10 mm.
Introduction
High recurrence rates of up to 26% have been described in the recent literature with using the Awl technique, or SEAL technique (subcutaneous endoscopically assisted ligation), in which a curved or straight stainless steel needle is introduced percutaneously anterolateral to the internal ring, passing a circumferential ligature, without resection of the processus vaginalis.5,6 Some other series report very low recurrence rates of 0.73%–4.3%.7–9 Laparoscopic inversion ligation has been reported with recurrence rates of 3.8–4.25% 10 and other reviews with 0–5%.11,12 Or, by laparoscopic suturing of the inguinal ring, without any removal of the processus vaginalis, recurrence has been reported at 2–3.7%. 13 From the Universities of Luebeck and Jena, they present their 402 cases. They have a higher recurrence than the open operation, but they do not resect the hernia sac, which is the main theme of our article. 14
Becmeur et al. and Tsai et al. described a technique similar to the one presented in this article, in which they resect the processus vaginalis and then close the inguinal ring, having excellent results with 0%–1.2% recurrence.15,16
We describe a technique based on the theory that congenital inguinal hernia (CIH) is due to a patent processus vaginalis, and therefore, the procedure should be to entirely resect it, with or without closure of the internal ring. This allows the peritoneal scar tissue to close the area of the ring. Also, this scarring occurs in the extent of the inguinal canal where the dissection took place, therefore causing the same peritoneal scarring and sealing of the inguinal floor with complete resolution of the problem.
Materials and Methods
With ethics committee approval, a proper informed consent was obtained. During July 2003 to April 2008, we changed our surgical technique from open to minimally invasive surgery (MIS) for CIH repair. A total of 91 patients have been operated on (76 males, 15 females). Age range was between 2 months to 11 years (mean, 3.5 years). Six cases were incarcerated hernias (6.5%), and 2 of them had the ovary in the sac. None had signs of estrangulation.
The technical details for the procedure are as follows. The patient is placed is in the decubitus position, with the surgeon at the head of the table and the monitor at the feet. The pneumoperitoneum is achieved by using the Veress needle, up to 8–12 mm Hg. Three trocars are used. One (5 mm) is placed as the umbilical port and two (3 or 5 mm) on the flanks. The dissection is started by using a dissector and scissors. The sac is everted and the initial cut is done above the internal inguinal ring in the parietal peritoneum (Figs. 1–3). Then, the dissection is carried out by separating the hernia sac from the vascular structures, and the vas, if male. Great care is taken when the total resection of the processus vaginalis is done by using cautery and scissors.
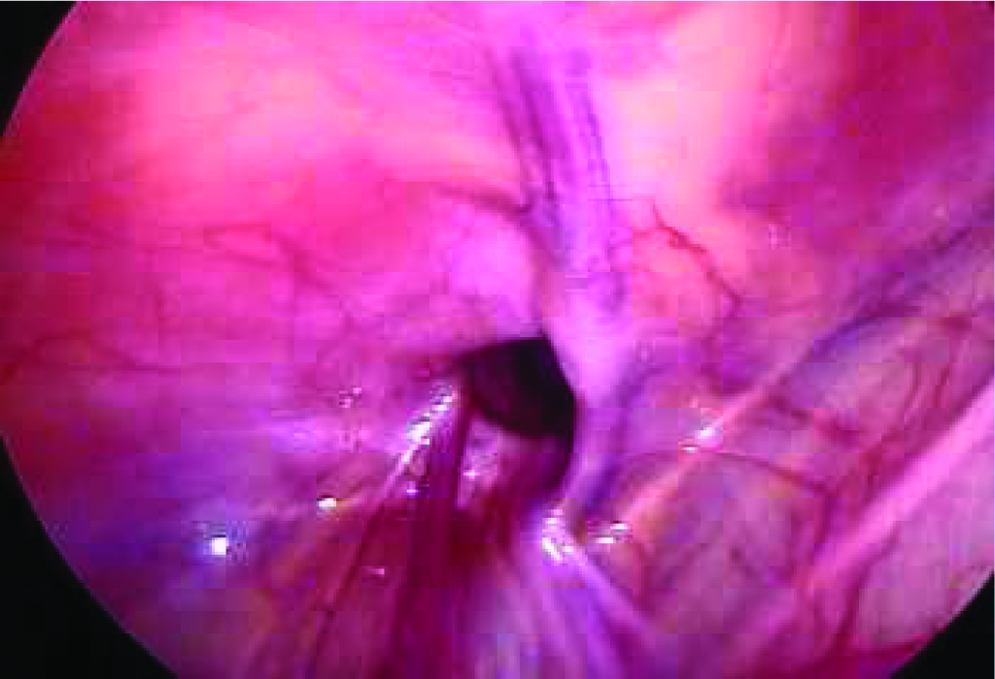
Laparoscopic view of inguinal hernia.

The sac is everted and the initial cut is done above the internal inguinal ring in the parietal peritoneum.

Hernia sac separated from the vascular structures, and the vas, if male.
Some of the parietal peritoneum is taken during the resection and a small circular area of deperitonealized surface around the internal ring is left. The processus vaginalis is completely resected (Fig. 4). This allows the peritoneal scar tissue to close the area of the ring. Also, this scarring occurs in the extent of the inguinal canal where the dissection took place.

The sac is completely removed with a circular area of parietal peritoneum.
In the male patients (Figs. 5 and 6), we use a 3-mm Maryland dissector to measure the ring, and with the grasps open gives a 10-mm size. The hernia sac is completely removed together with some of the parietal peritoneum. Then, if the ring is wider than 10 mm, we do a purse-string stitch around the deperitonealized inner ring. Great care is taken not to strangulate the vas and to keep the vessels uninjured. 17 We use a polyester suture (2-0 RB1) for this stitch. Then, the vas is checked so that there is enough room for its entrance to the inner inguinal ring.
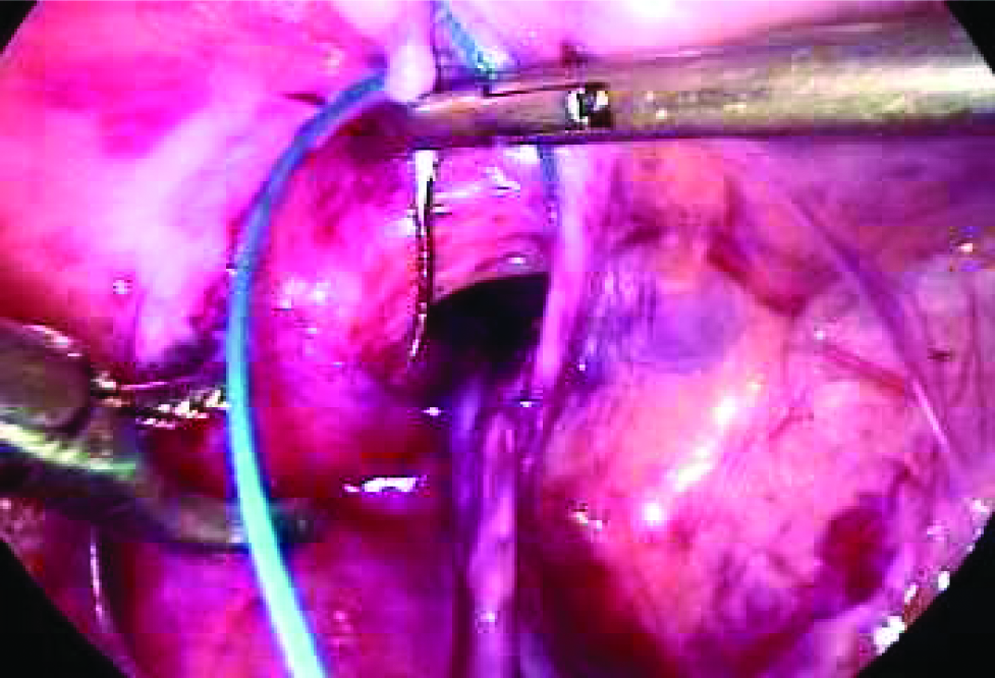
Closure of the ring.

Final results of closure.
In the 15 females, there was no need to perform a closure stitch in the inner inguinal ring, because all the rings were less than 10 mm.
Results
All operations were successfully performed laparoscopically. There were no immediate surgical complications. The operative time was in the range of 35–72 minutes (average, 40), being longer in the initial cases and shortening as experience was obtained. Two hematomas were followed until gone, without further need for intervention. These were the only complications (2.2%).
Close follow-up in the clinic has been 5 months to 4 years without a single recurrence. In 4 cases, 3 months after the operation, we did a laparoscopic evaluation of the contralateral side due to associated cryptorchidism, in which we were able to confirm a complete closure of the interior inguinal ring. All other bilateral cases were done in a single operation.
Discussion
Multiple techniques have been described to repair CIH by MIS. They all involve the high ligation of the sac with incomplete resection of the processus vaginalis and never leaving the area deperitonealized. Using the technique described in this series of 91 patients, no recurrences have been observed. We conclude that the most important factor to avoid recurrence in a CIH is to completely resect the processus vaginalis/hernia sac and surrounding parietal peritoneum, causing scarring and reperitonization of the inguinal canal, inguinal ring, and adjacent area. Therefore, laparoscopic repair of CIH by a complete resection of the hernia sac and the parietal peritoneum surrounding the ring has a better overall outcome than other MIS options already published, where some leave the processus vaginalis incompletely resected. And, unless the inguinal ring is wider than 10 mm, we do not close it in this series.
Conclusion
This article is not conclusive in the matter of closing or not closing the inguinal ring. Considering the orchidopexy results of associated inguinal hernias, we think that even in rings that are wider than 10 mm, it is not necessary to close them after the resection of the sac and surrounding peritoneum. Further experience is required. The continuation of this series will be presented at IPEG 2009, in which we have been leaving all the rings without purse string. This excludes prematures and newborns that have wide rings, in which case, we will close.
Footnotes
Disclosure Statement
No completing financial interests exist.