
Abstract
Abstract
The gold standard of treatment in the case of fecal peritonitis in association with traumatic rectal perforation is closure of the perforation in combination with a diverting colostomy. In this paper, we report the successful laparoscopic management of such a trauma without colostomy 24 hours after the incident.
Introduction
Case Report
A 4-year-old girl was transferred from another hospital with a history of impalement of a sharp object about 24 hours earlier. The girl had fever, tachycardia, tachypnea, and obvious signs of peritonitis on the physical examination. The abdominal X-ray performed in the other hospital showed the pneumoperitoneum. After receiving fluid resuscitation, the child went for surgery. During the consent procedure, the parents were informed about the treatment options: laparoscopy, closure of the lesion combined with a diverting colostomy, and the possibility of conversion into a laparotomy. The parents asked the surgeon to try to avoid a colostomy, if feasible. A child abuse procedure was instigated, as usual, by all impalement lesions.
Under general anesthesia, with the patient in the lithotomy position, the anal inspection revealed a fissure at 12 o'clock, and by the digital examination, the lesion could be felt at the rectal anterior wall about 4 cm above the dentate line. The preoperatively performed cystoscopy and vaginoscopy to exclude associated lesions were normal. For the laparoscopic procedure, four 5-mm ports were placed: one infraumbilical for the optic and, after creating a pneumoperitoneum of 10 mm Hg, two other ports were placed at the right hypochondrium and one at the left hypochondrium. At laparoscopy, a large transverse rectal lesion was seen at the level of the peritoneal reflection (Fig. 1), and there was fecal contamination of the peritoneal cavity with signs of peritonitis. After cleaning of the fecal material from the peritoneal cavity with isotonic saline solution, the rectal lesion was closed with running sutures of Vicryl 4/0 (Fig. 2). A transanastomotic 24 CH rectal tube was placed under laparoscopic control. After flushing the peritoneal cavity again with isotonic saline solution, the ports were removed without leaving drains.
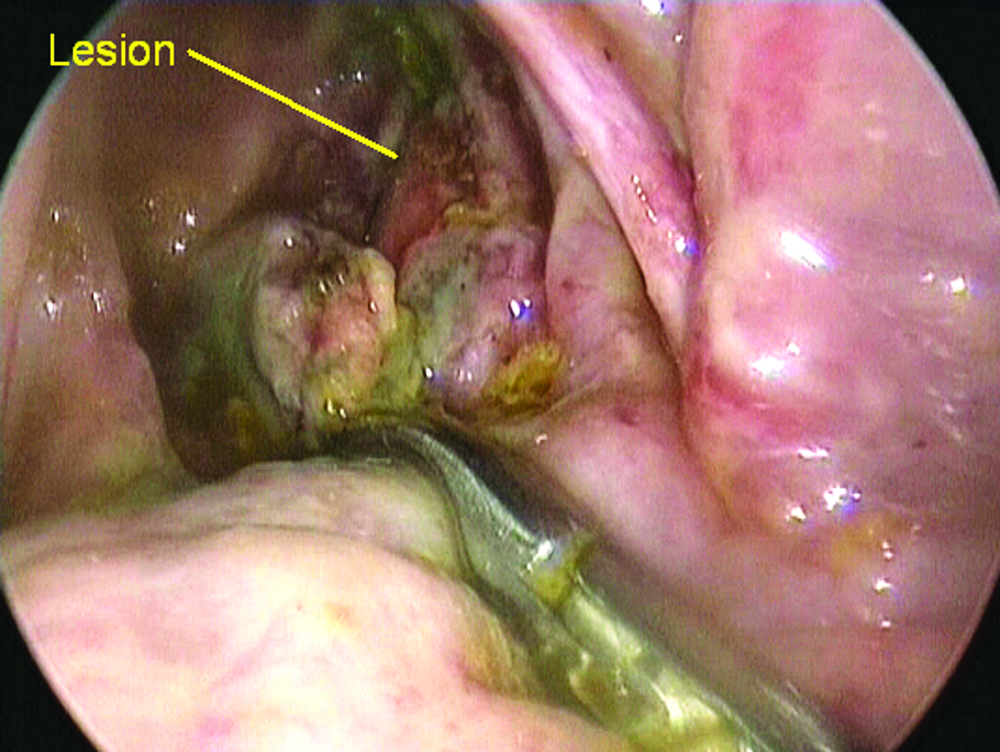
Rectal perforation.
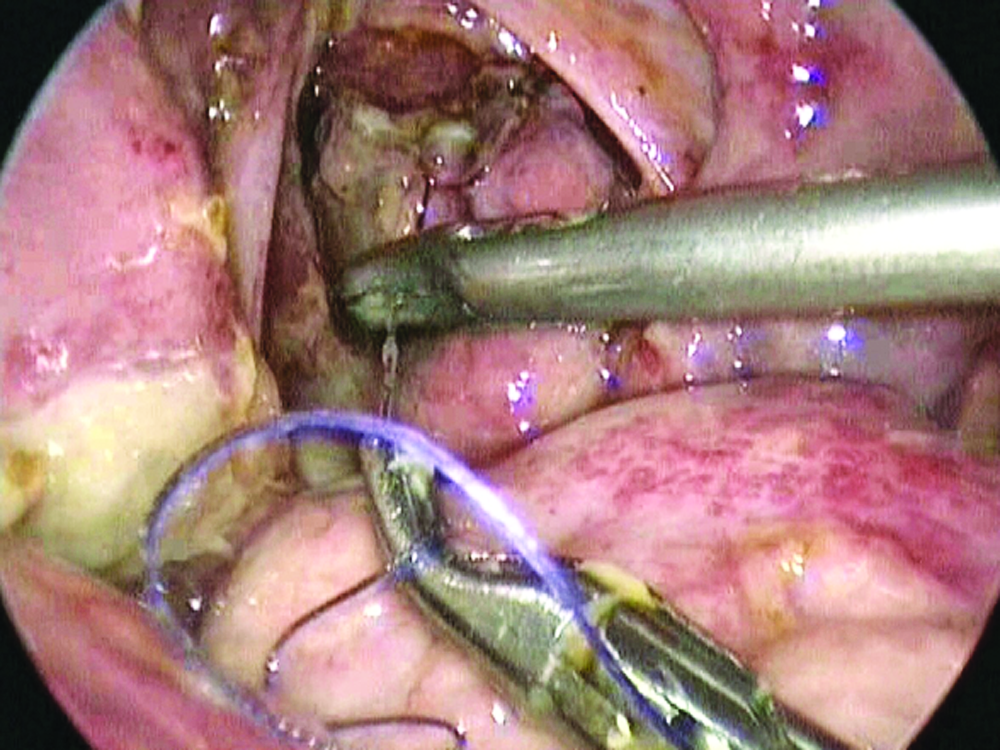
Closure of the rectal perforation.
The patient received intravenous antibiotics (amoxicillin/clavulanate combined with gentamicine) for 1 week. The rectal tube was left for 5 days. The oral feedings could be started at postoperative day 2. The patient made an uneventful postoperative recovery and was discharged on postoperative day 10 because the investigation for child abuse was not completed.
Discussion
This is probably the first report in the literature of this kind of management in the pediatric population. There is a report in the literature of using laparoscopy to define the intraperitoneal extension of injuries and guide the colostomy placement. 1 In the adult literature, there are some reports of laparoscopic closure of rectal perforation without protective colostomy in the case of incidental injury of the rectum during the prostatectomy 2 or radical cystectomy, 3 although this is not really comparable to the traumatic perforation of the rectum as in our patient. Because the traumatic rectal injuries in children are rare, it is difficult to get enough experience with the management adopting new techniques. Undoubtedly, for the children presenting with this kind of injury, tread by the laparoscopic approach without a diverting colostomy has a major advantage. A colostomy has a big impact on the psychosocial life. Further, the cosmesis is also important.
Conclusion
This case demonstrates the feasibility of laparoscopic closure of a rectum perforation without a colostomy. It may be that the dogmatic approach of a proximal diverting colostomy in the case of fecal peritonitis associated with traumatic rectal perforation should be reevaluated.
Footnotes
Disclosure Statement
No competing financial interests exist.