
Abstract
Abstract
Trichobezoars from the ingestion of hair typically develop into a large, spherical foreign body within the stomach. Due to the frequently large size, endoscopic removal is usually not feasible beyond diagnosis. Likewise, the size often has forced surgeons to remove these trichobezoars via laparotomy. Laparoscopic removal of gastric trichobezoars has been reported, but the concern with this technique is that the complete removal of the large bezoar without spillage of hairs in the peritoneal cavity may be difficult. As such, most of the reports are laparoscopic assisted, but still utilize an extended incision to facilitate direct removal from the peritoneal cavity. In this case, we describe in this paper the complete laparoscopic removal of a giant trichobezoar in a 10-year-old child without spillage, using piecemeal removal through the umbilical incision without extending the incisions.
Introduction
Case Report
History
A 10-year-old female with known trichotillophagia, attention-deficit hyperactivity disorder, and learning disability presented to her primary care provider with a 10-day history of fevers, emesis, and diarrhea. Her emesis was noted to be associated with oral intake. From a previous visit, there was a 3-kg weight loss documented over the previous 2 months. As part of the evaluation of these symptoms, she underwent an abdominal computed tomography (CT) scan, which demonstrated a gastric bezoar. She was admitted to Children's Mercy Hospital (Kansas City, MO) and underwent an upper endoscopy, which demonstrated a trichobezoar appearing to extend into the pylorus. The bezoar was clearly too large to consider endoscopic removal, and surgical consultation was obtained.
Operation
A 12-mm port was placed in the umbilicus with a direct cutdown through the center of the umbilicus. Then, a 5-mm port was placed in the midepigastrum and a 5-mm stab incision was placed in the left-upper quadrant (Fig. 1A). Two 3-0 silk sutures were placed in the anterior portion of the stomach near the fundus/antral junction and were brought out via the abdominal wall, using the suture-passer device (Endo Close® Trocar Site Closure Device; U.S. Surgical Corp., Norwalk, CT). This maneuver fixed the stomach in three dimensions and triangulated the operative surface by simplifying the gastrotomy and bezoar retrieval. The harmonic shears (Ultracision Harmonic Scalpel®; Ethicon Endo-Surgery, Cincinnati, OH) were used to open the anterior wall of the stomach. Two graspers were used to gently separate the bezoar from the mucosa circumferentially by keeping the jaws closed to avoid separating the hairs from the bezoar (Fig. 2). A standard deployable laparoscopic bag (USSC 10-mm Endo Catch®; U.S. Surgical Corp.) was passed directly into the stomach to capture the bezoar completely from inside the stomach, so there would be no extraluminal handling of an uncontained bezoar. The bezoar effectively filled the bag, with approximately 10–20% of the mass still outside the bag. The umbilical port was then exchanged for a 15-mm port to allow the passage of the splenic laparoscopic bag (USSC 10-mm Endo Catch II®; U.S. Surgical Corp.). The smaller bag was placed into the larger bag, and the open end of the larger bag was brought out through the umbilicus to facilitate the piecemeal removal of the bezoar. The abdomen was reinsufflated and the linear cutting stapler (Endo-GIA Universal XL®; U.S. Surgical Corp.) was used to close the gastrotomy in a longitudinal fashion with three deployments, using the 3.5-/45-mm loads (Fig. 2). The bezoar had a weight of 238 g, measuring 13.0 × 7.5 × 6.5 cm. She was allowed to drink liquids and advance to solid foods on postoperative day 1 and was discharged home on postoperative day 3. She was doing very well at the 1-month follow-up (Fig. 1B).
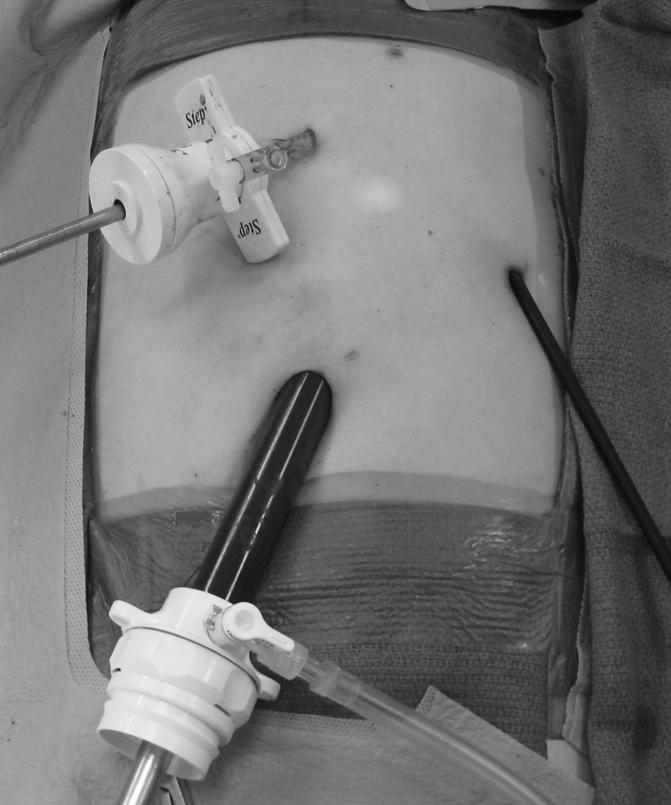
Laparoscopic port placement with postoperative outcome.

Triangulation of the stomach using stay sutures and blunt separation of the trichobezoar from the surrounding stomach.
Discussion
The presence of a gastric trichobezoar has been associated with multiple gastrointestinal complications. Protein-losing enteropathy, gastric polyps, steatorrhea, pancreatitis, intestinal and gastric obstruction, and gastric perforation have been described.2–7 Further, bezoars have been demonstrated to be the cause of 0.8% of small-bowel obstructions treated laparoscopically. 8 Treatment of gastric trichobezoars has been attempted by removal with endoscopy, but usually requires operative intervention, unless they are quite small. 9 Adjunctive measures reported to treat phytobezoars include metoclopramide, papain, cellulase, and carbonated beverages, but these are of little utility with trichobezoar.10–15
The removal of trichobezoars in patients via laparotomy has been well described in multiple reports. The first successful removal was documented in 1896. 1 There are many subsequent reports in the adult and pediatric literature demonstrating the removal of bezoars via laparotomy. The advent of minimally invasive surgical techniques has allowed for a shift toward laparoscopic attempts at removal. Laparoscopic treatment has been shown to be safe and effective for bezoar-induced small-bowel obstruction in adults.16–19 However, small-bowel bezoars are smaller and the bowel can be easily brought out to allow for a clean extraporeal removal without spillage. Laparoscopic removal of gastric trichobezoars has been documented in several cases. A 19-year-old female had a large gastric trichobezoar removed laparoscopically, but its removal from the abdominal cavity required the extension of one of the lower port sites to 4 cm. 20 A 2-cm incision was used in an 18-year-old pregnant woman whose gastric trichobezoar was ultimately removed from the abdomen via moreselization through a laparoscopic approach. 21 This technique was reported as successful in a 62-year-old man; however, in this case, there was no need for extension of the length of the port sites for morselization. 22 The use of laparoscopic removal of gastric bezoars appears to be safe and effective in the adult population.
There is a relative paucity of reported cases of laparoscopic treatment of gastric trichobezoars in the pediatric population. The use of a minilaparotomy of 2 cm in length in an 11-year-old girl has been reported. In this case, a trocar was placed into the stomach after gaining access to the stomach via the minilaparotomy, and a laparoscopic scissors was used to break apart the trichobezoar. 23 There are two other cases of a 7-year-old and a 12-year-old girl who had trichobezoars in the stomach removed via a minilaparotomy, which was assisted via laparoscopy.24,25 In our case, we were able to utilize intragastric maneuvers to control the bezoar from spillage and extract it without a minilaparotomy.
Conclusion
Therefore, we forward this technique as we feel it is a safe, simple operation that most surgeons should be able to replicate to avoid an unnecessary laparotomy for children with this condition.
Footnotes
Disclosure Statement
No competing financial interests exist.