
Abstract
Abstract
Background and Aims:
In the view of small sample sizes of the studies published so far, the value of video capsule endoscopy (VCE) in diagnosing celiac disease (CD) is yet to be determined. The aim of this work was to systemically determine the overall diagnostic characteristics of VCE in diagnosing noncomplicated CD, compared to the gold standard, using meta-analysis.
Patients and Methods:
An extensive literature search was performed looking for prospective, controlled trials, with investigators blinded to results of the pathology of small-bowel biopsies. Two independent authors performed data extraction and assessment of the methodologic quality of each trial. Diagnostic characteristics of each trial were collected, and pooled sensitivity, specificity, likelihood ratios, and diagnostic odds ratios were computed. Description of complications and costs was included, if reported.
Results:
A total of three studies met the inclusion criteria (n = 107; 63 with CD and 44 without). The overall pooled VCE sensitivity was 83% (95% confidence interval [CI] = 71–90%) and specificity was 98% (95% CI = 88–99.6%). No major complications were reported. The costs were mentioned only in one study.
Conclusions:
The overall diagnostic characteristics of VCE, when used to diagnose celiac disease, though good with an experienced eye, could not justify the routine use of VCE as an alternative to the pathology of small-bowel biopsies. More studies are needed with proper cost-benefit analysis.
Introduction
Although serologic markers of the disease have been used with good sensitivity and specificity, the gold standard for the diagnosis of CD remains the typical pathologic findings in small-bowel biopsies obtained through esophagogastroduodenoscopy (EGD) and multiple duodenal biopsies. 3 However, this invasive method of diagnosis may be limited by the patients' aversion to undergo EGD, especially in asymptomatic or mildly asymptomatic patients. Other limitations include the difficulty in obtaining adequate and properly oriented tissue samples, the occurrence of patchy mucosal lesions that can be missed by the biopsies, and in some cases, several mucosal changes occur in the jejunum, which is not accessible to conventional EGD. 1
Video capsule endoscopy (VCE) is one of the most recent inventions that has made an impact in the diagnostic workup of gastrointestinal diseases, mainly small intestinal pathology, the part of the gut that cannot be totally visualized by upper and lower gastrointestinal endoscopy. 4 Since the first report documenting the use of VCE, many adult clinical trials have taken place. In 2001, the Food and Drug Administration (FDA) approved a wireless VCE device (Given Imaging, Yoqneam, Israel) in adult patients, that has since had a significant impact on managing adult patients' small-bowel diseases. 5 It has the ability of eight-fold magnification of the small-bowel mucosa. The main advantages of VCE are that it is noninvasive and that it images the majority of entire small bowel. 4 The aim of this study was to systemically determine the overall diagnostic characteristics of VCE in diagnosing noncomplicated CD, compared to the gold standard, using meta-analysis.
Patients and Methods
Criteria for considering studies for this review
Types of studies
Only prospective studies that looked at diagnostic characteristics of VCE in patients with noncomplicated CD, compared to the gold standard, were included, provided the VCE reader was blinded to the results of duodenal pathology.
Types of participants
In order for studies to be considered for inclusion in this review, the study participants met the following criteria: 1) Participants could be of any age or sex and 2) patients with symptoms suggestive of CD or biopsy-proven celiac disease.
Types of interventions
Studies were considered if participants had EGD with duodenal pathology and VCE.
Types of outcome measures
The primary outcome measure was the successful diagnosis of celiac disease using VCE. Secondary outcome measures were: 1) associated complications using EGD and VCE and 2) costs of each diagnostic tool.
Search strategy for identification of studies
The following sources were searched to identify studies: the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE (from 1999 to March 2008), EMBASE (from 1999 to March 2008), Pubmed (the last 180 days), Web of Science, Scopus, Database of Abstracts of Reviews of Effects (DARE), the Clinical Trials database (ClinicalTrials.gov), and the FDA website. The manufacturer of VCE (Given Diagnostic Imaging System, Yoqneam, Israel) was contacted to see if there were any ongoing trials or unpublished data. The abstracts of Digestive Disease Week (DDW) and the International Conference of Capsule Endoscopy (ICCE) of the last 3 years were looked at.
A search strategy, using both medical subject headings and textwords, was developed in conjunction with a health sciences librarian. No language restrictions were used for the search. The following general search terms were used: “celiac disease” or “coeliac disease” or “gluten-sensitive enteropathy” and “capsule endoscopy” or “gastrointestinal endoscopy” or “VCE.” Additional efforts to identify relevant trials were made through browsing the reference lists of included articles to identify any potentially relevant citations.
Methods of the review
Description of studies
Selection of studies occurred in two phases. Initially, two reviewers (WE and HH) screened all of the articles retrieved through the search of databases, clinical trials, and grey literature described above. All studies were first screened on the basis of title, and then on the basis of abstract. During this screening process, studies were classified into three categories: “exclude” for studies in which it was clear from either the title or abstract that the study did not address the PICO question (P = population, I = intervention, C = control, O = outcome) or was not fulfilling the inclusion criteria, “include” for prospective trials that addressed the research question, and “unsure” for studies in which there was uncertainty. Studies denoted “include” or “unsure” were considered potentially relevant and were further examined in the second phase of the selection process.
In the second phase of study selection, two reviewers (WE and HH) independently assessed the relevance of the potentially relevant studies, based on the criteria for inclusion in the systematic review listed above. The full text of the articles was retrieved in order to decide whether these criteria were met. Disagreement was resolved through discussion and consensus decision. Reviewers were not blinded to the names of authors and institutions, journal of publication, or study results during study selection or at any other stage of the review.
Methodological quality of included studies
Assessment of quality for the studies included in this review was made independently by two reviewers (WE and HH) for fulfillment of the predefined inclusion criteria. The QUADAS tool for quality assessment was used.6,7 Differences in rating were resolved through discussion and mutual consensus.
Data extraction
Data extraction was performed from the original studies to a specific preformatted paper form by the two reviewers. The following data were extracted: study methods (study design, withdrawals/loss to follow-up), study participants (sample size, age, gender, and symptoms), timing of the EGD and VCE, endoscopic and VCE appearance, histologic findings, number of observers, inter- and intraobserver variability (kappa), and outcomes (sensitivity, specificity, PPV, NPV, complications, if any, and costs).
Data analysis and statistics
Since two of the three studies had zero entries in their 2 × 2 diagnostic tables, we chose to estimate and pool data by using exact methods, rather than the more common asymptotic approaches that would have led to inaccuracy in these situations. Sensitivity and specificity data were combined by using simple pooling, with confidence intervals (CIs) computed by using the modified Wald approach. 8 Thus, the estimates for sensitivity, specificity, and their 95% CIs did not arise from meta-analytic techniques. However, in the presence of lack of heterogeneity across the studies, this was not numerically consequential. Likelihood ratios, both positive and negative, were combined by using the exact method for pooling common odds ratios 9 —the ensuing odds ratios were converted to likelihood ratios, using the standard formula. 10 CIs were computed by using the mid-P method. Standard asymptotic methods were used to assess heterogeneity via the I2 statistic. 11 Inter- and intraobserver agreements were documented by the kappa statistic, which measures agreement over and above what would be expected to occur by chance alone. All computations were done by using the Excel 2000 (Microsoft Corporation, Redmond, WA) and Stat-Xact 7.0 (Cytel Software Corporation, Cambridge, MA) software programs. Graphs were produced by using S-Plus 8.0 (TIBCO Software Inc., Palo Alto, CA) software. Positive and negative predictive values were not pooled due to our inability to estimate population prevalence of CD from the given studies.
Results
Two hundred thirteen articles were initially identified by using the above-described search strategy. One hundred ninety one articles were initially excluded on preliminary review of the title and/or abstract, leaving 22 articles for reviewers' evaluation. One study was added after manual search at the articles' bibliographies. Nineteen studies were excluded after a full reading, as they did not fulfill inclusion criteria (Fig. 1). One study was further excluded 12 after contacting the author, as noncomplicated CD patients were already included by another multicenter trial that was included in the presented systemic review.
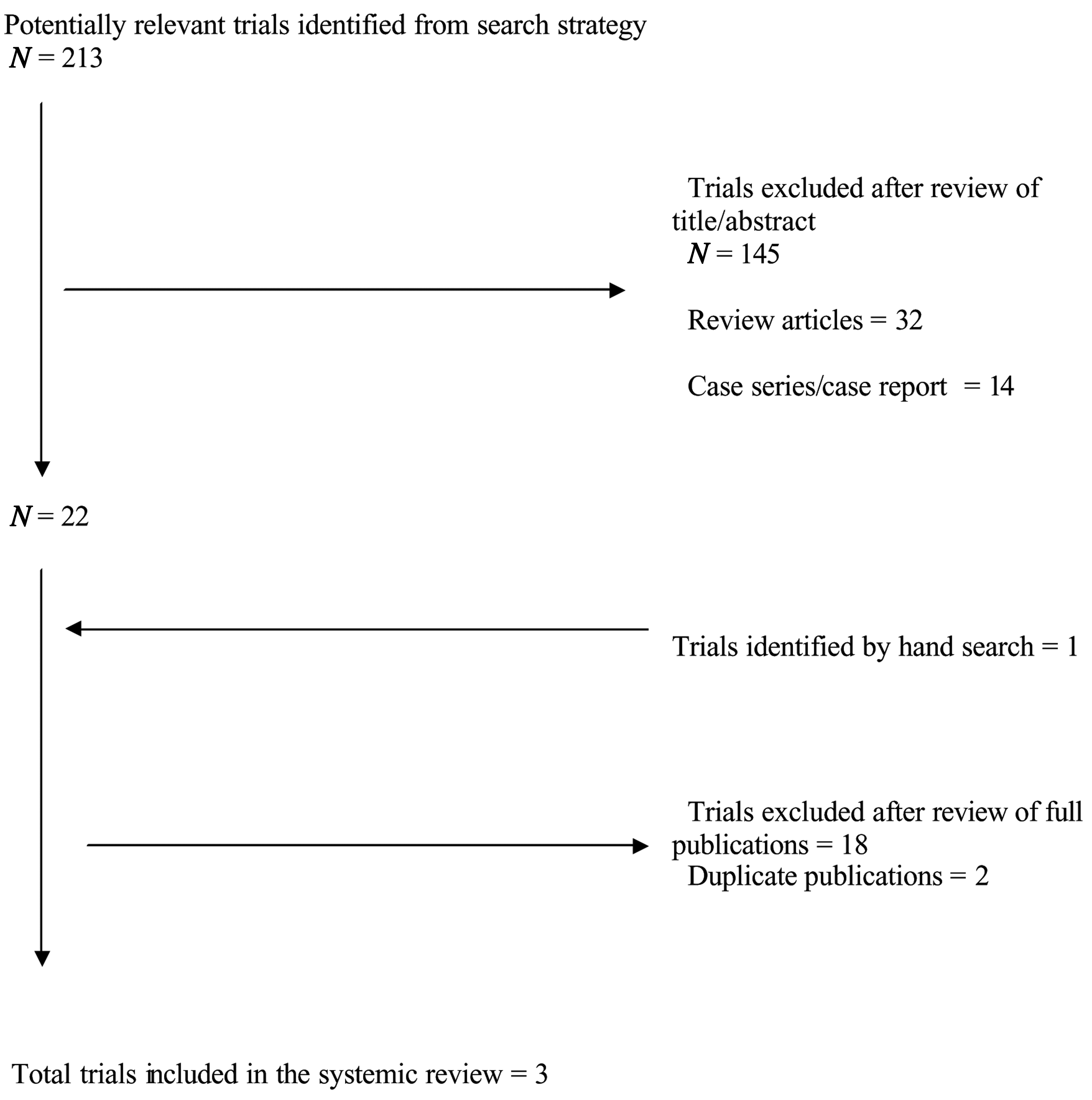
Trial search flow for the systemic review.
A total of three studies were appropriate for the meta-analysis involving a total of 107 adult patients (Table 1).13–15 The three studies were published in the English language, two were single-center (Canada and the UK),13,14 and the third was multicenter (Italy and the United States). 15 The final kappa value between the two reviewers (WE and HH) was equal to 1, indicating complete agreement.
In 2 studies,14,15 the time interval between endoscopy (EGD) and VCE was 1–15 days for the majority of patients. In the study by Hopper et al., the duration between EGD and VCE was not stated. The number of investigators who performed VCE readings was variable among the three studies. While Hopper et al. had one experienced gastroenterologist, 13 the other two studies had four different observers. In the study by Petroniene et al., two gastroenterologists were very experienced and their readings' sensitivity and specificity were at 100%. 14 The other two observers were less experienced and achieved less sensitivity and specificity. The average sensitivity, specificity, PPV, and NPV for this study were 70, 100, 100, and 77%, respectively, with a kappa value of 0.26–1.0. 14
In the study by Rondonotti et al., the investigators' interobserver agreement in the assessment of mucosal lesions was examined, prior to the study, by asking the four investigators to read VCE from 53 patients; 24 of them had CD (different from those recruited into the study). The kappa value ranged between 0.56 and 0.87. The overall sensitivity, specificity, PPV, and NPV of VCE in diagnosing CD from this study were 87.5, 90.9, 96.5, and NPV of 71.4%, respectively. 15
Sensitivity and specificity were simply pooled among the three studies. The combined studies showed a total of 63 diseased patients, of which 52 tested positive with VCE for a sensitivity of 83% (95% CI: 71%, 90%) (Fig. 2). Conversely, of 44 nondiseased patients, 43 tested negative, for an overall specificity of 98% (95% CI: 88%, 99.6%). Both estimates were relatively homogeneous across studies (I2 = 0%) (Fig. 3).

Pooled sensitivity of video capsule endoscopy in diagnosis of celiac disease.

Pooled specificity of video capsule endoscopy in diagnosis of celiac disease.
These high sensitivities and specificities led to very favorable likelihood ratios for VCE. A patient's odds of having the disease were nearly 35 times higher after testing positive with VCE (LR+ve: 34.5; 95% CI: 16.7, 43.5), while patients' odds of disease were nearly five times smaller after a negative test result (LR-ve: 0.22; 95% CI: 0.01, 0.64). Again, these results were generally homogeneous across the studies (I2 = 0%).
There were no major complications reported. Petroniene et al. reported minor discomfort in 1 patient due to WCE and 8 patients with minor discomfort due to EGD. Another patient had severe discomfort with EGD. None of the patients needed surgical intervention. 14 Although the Hopper et al. study was not designed to assess the cost benefit, they reported the hospital costs to be 693 sterling pounds per patient for VCE, compared to 410 for EGD. 13
Discussion
CD is the most common case of enteropathy in the West. 2 Although serologic tests, mainly antitissue transglutaminase and antiendomyseal IgA antibodies, could help in making the diagnosis, the gold standard for diagnosis is the typical pathologic findings of small-bowel biopsies. 3 Occasionally, the patient may decline EGD or EGD may be contraindicated. This may lead to some difficulties in making the diagnosis, especially if the patient is IgA deficient, in which case the VCE could be very helpful. Since the introduction of VCE in 2000, more indications are immerging, one of which is the diagnosis of CD. Typically, VCE is used to visualize the small bowel, especially in cases of obscured gastrointestinal bleeding.4,16
CD could be patchy or affecting the distal small bowel, in which case small-bowel biopsies could be negative. 17 VCE may be of a value in the diagnosis of complications of CD.18,19 In the view of the few publications investigating the value of VCE in the diagnosis of noncomplicated CD with small sample sizes, we performed a systemic review to explore the diagnostic test characteristics of VCE in the diagnosis of noncomplicated CD. The three studies included in the systemic review have minimal heterogeneity among them. A sensitivity analysis exploring any major differences in the random versus fixed-model effect showed no difference!
No subgroup analysis was needed, as the studies were similar in patient population and outcome. A few studies were excluded, despite addressing the same topic, as they looked at the diagnostic value of VCE in the diagnosis of complications related to CE (e.g., small-bowel lymphoma). 18 Other studies examined the role of VCE in refractory CD or when initial EGD and biopsies are negative; however, the gold standard in these studies was vaguely defined. 19
The overall pooled diagnostic test characteristics in our systemic review were acceptable, especially when it came to specificity (i.e., when VCE is negative for celiac disease); it is unlikely that the patient has CD. Nevertheless, 20% of patients may have CD and being missed when using VCE. Interestingly, the specific pathological diagnostic criteria (Marsh criteria) thought pathognomonic, are not 100% specific to celiac disease. 3
Endoscopic findings of CD have been disappointing in making the diagnosis, 20 but one could argue that VCE is better, as it gives eight times magnification, compared to normal endoscopy, and also, it examines the entire small bowel. The latter point is important, taking into consideration that CD could be patchy.4,16 Overall, although using VCE as a routine diagnostic tool for the diagnosis of CD might be too optimistic, there may be some scenarios where VCE use by an experienced eye could be helpful, so evaluation of this diagnostic tool in the diagnosis of CD is warranted.
Conclusions
VCE offers an alternative way of diagnosis of CD with acceptable diagnostic test characteristics, especially if used by an experienced gastroenterologist. It is helpful in situations when EGD and duodenal biopsies cannot be done. More studies are needed to explore the value of VCE in diagnosing CD in situations where CD is very likely and duodenal biopsies are negative and suggesting that small-bowel changes might be, although unlikely, more distal. Cost analysis of VCE, compared to EGD, needs to be thoroughly examined.
Footnotes
Acknowledgments
The authors are grateful to Liz Dennett for searching and library support, Brian H. Rowe, MD, MSc, CCFP (EM), FCCP, Terry P. Klassen, MD, MSc, FRCPC, and Donna Dryden, PhD, for their valuable guidance, and to F. Biagi, MD, for his prompt response to the authors' queries.
Disclosure Statement
No competing financial interests exist.