
Abstract
Abstract
Introduction:
Laparoscopic nephrectomies (LNs) may be performed in children with benign renal disease by the transperitoneal (TP) or retroperitoneal (RP) approach.
Objectives:
The aim of this study was to present our early results from using both the laparoscopic transperitoneal and retroperitoneal approach, highlighting the change in the approach to a better, simpler procedure performed by experienced surgeons.
Materials and Methods:
Between February 2002 and June 2006, 30 LNs were performed, with the first 10 patients by TP (group 1) and the remaining patients by RP (group 2). Two patients were not included. Demographic data were compared: mean age (88 vs. 66.6 months), gender (30% female vs. 70% male), and laterality (60% left-handed vs. 40% right-handed). Other factors were assessed, as well: Operating time was compared, as was morbidity, analgesics requirement, postoperative hospital stay, and time to resume oral intake.
Results:
LN was performed in 28 of the 30 cases. One case in each group was converted. Both groups were similar regarding operating time (TP: 92.2 minutes vs. RP: 121.1), hospital stay (36.5 hours vs. 28.8), postoperative analgesia (2.1 doses of dipyrone and 1.2 doses of nalbuphine vs. 2.3 and 1.4). RP was associated with significantly faster postoperative analgesia tolerance than that of the TP approach (7.8 hours vs. 14.4; P < 0.05). Two (22.2%) patients in group 1 presented with vomiting, whereas no patients in group 2 had postoperative vomiting (P < 0.05). No further postoperative complications appeared.
Conclusions:
In our hands, both laparoscopic TP and RP approaches are equally safe and effective, but the operating time was slightly shorter (not significant) and postoperative recovery significantly longer for TP. LN may be performed by both approaches, obtaining equal efficacy. TP may be associated with minimal paralytic ileus within the first 12–24 hours, meanwhile RP is related with better surgical skill and postoperative tolerance.
Introduction
Materials and Methods
Between February 2002 and June 2006, 32 LNs were performed. On the beginning of our learning curve, the first 10 patients were treated by using the TB technique (group 1), whereas in the rest (n = 20), we used the RP technique (group 2). Two patients underwent upper pole laparoscopic heminefrectomies, using the RP method, and these results are not included in this report. The indications for both groups were similar (Table 1). All of the kidneys extracted showed less than 10% function on a renal dynamic study.
TP, transperitoneal; RP, retroperitoneal; VUR, vesicoureteral reflux; MCDK, multicystic dysplastic kidney.
n = 30.
Both techniques were performed with three ports; for the TP approach, with the patient in the dorsal decubitus position, three ports were placed: one in the navel (10-mm optic device), with the second and third ports (5-mm working ports) on the half clavicular line below the rib cage and on the same side, 2 cm above the level of the superior iliac spine, respectively (Fig. 1). In the RP approach, with the patient in the lateral decubitus position and the hyperextension of the problem side getting a better active place, on the lower end of the twelfth rib, a 10-mm port was placed for the optic device, and the two working 5-mm ports, one above the of the iliac crest's upper line and the other resting on the external side of the lumbar complex muscle equidistant to the others (Fig. 2). For the material extraction, in all cases, the renal tissue was sufficiently thin enough to allow the extraction through the incision of the initial port (Fig. 3), except in 1 case, where it was necessary to triturate the tissue because of its side. Oral feeding was started between 6 and 12 hours after surgery, and a postoperative analgesic was used (dipyrone with nalbuphine), as required.
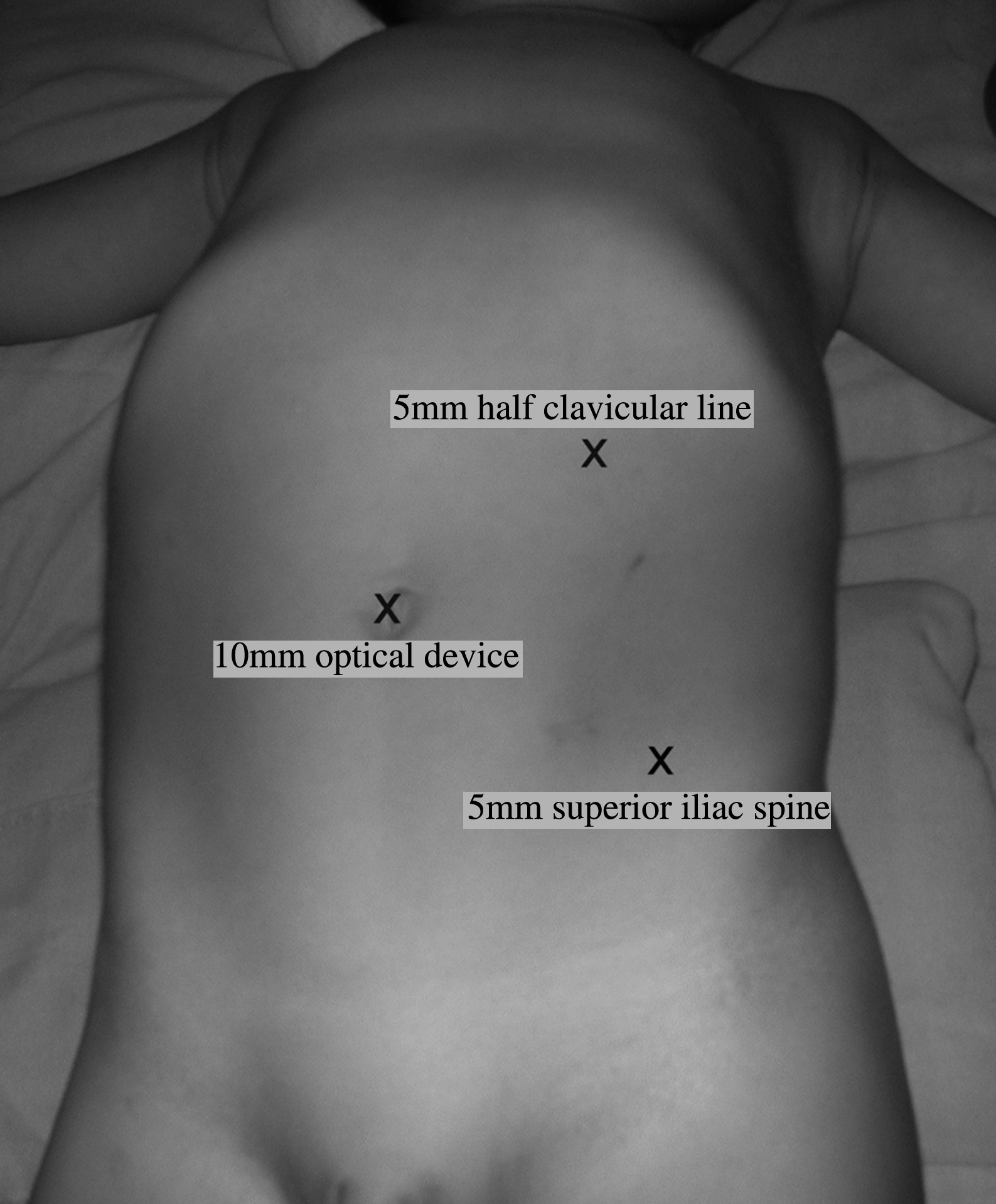
The transperitoneal approach. With patient in the dorsal decubitus position, three ports were placed, one in the navel (10-mm optic device), the second and third ports (5-mm working ports) on the half clavicular line below the rib cage, and on the same side, 2 cm above the level of the superior iliac spine, respectively.
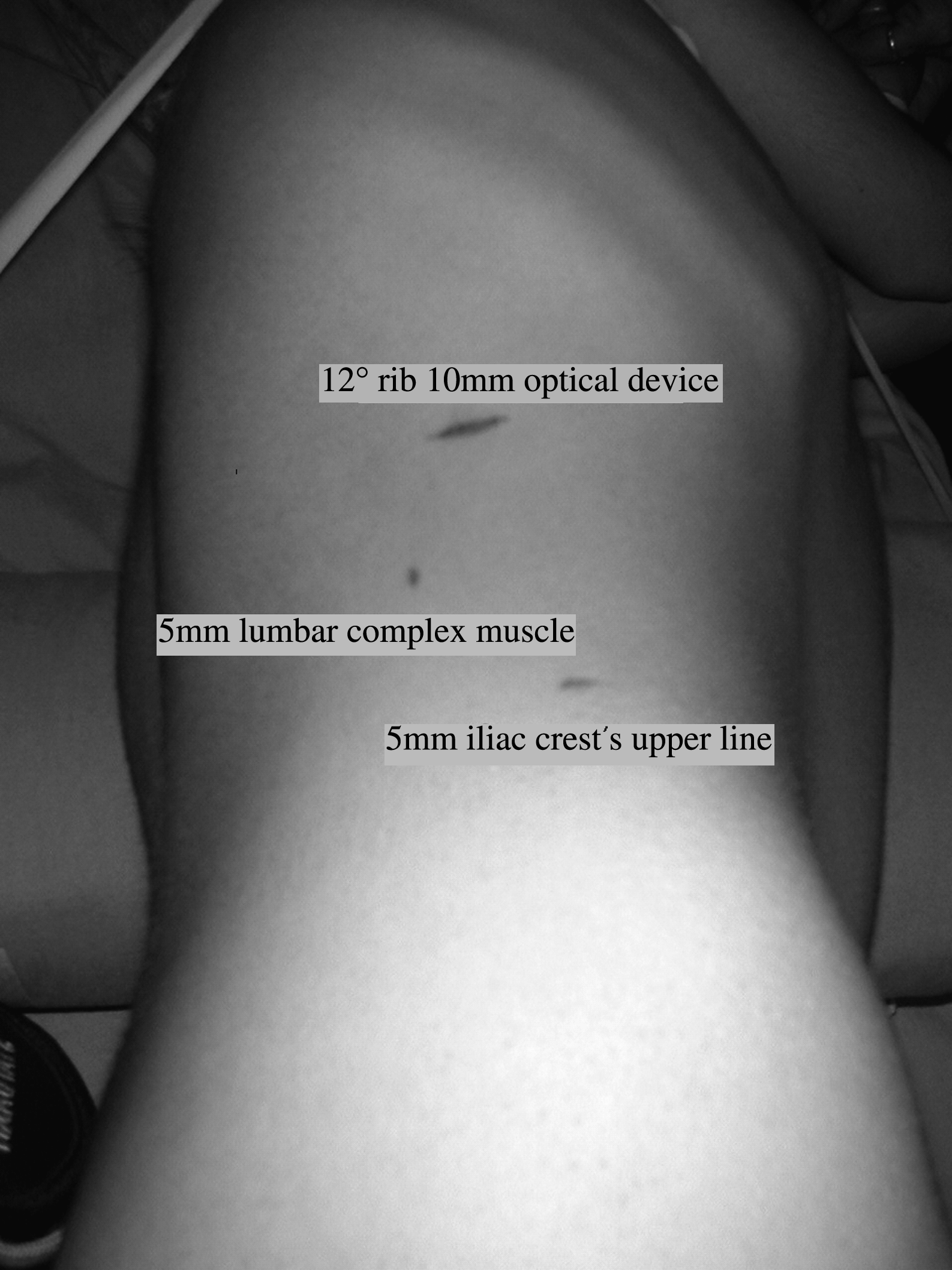
The retroperitoneal approach. With the patient in the lateral decubitus position with hyperextension, on the lower end of the twelfth rib a 10-mm port was placed for the optic device, and the two working 5-mm ports, one above the of the iliac crest's upper line and the other resting on the external side of the lumbar complex muscle equidistant to the others.

The material extraction was sufficiently thin enough to allow the extraction through the incision of the initial port.
Statistical analysis
Statistics were carried out through comparing both groups by means of the Student's t-test, Mann-Whitney, and the Z approximation for a study of proportions. A value of P < 0.05 was considered statistically significant.
Results
LNs were successfully carried out in 28 of the 30 cases. One case of RP nephrectomy had to be converted due to a massive hydronephrosis with perirenal fibrosis. In the other case, a TP nephrectomy changed into an open technique due to a problem with the equipment that occurred during surgery. In the 28 laparoscopic operations performed, there were no complications during surgery. During two retroperitoneal operations, we had peritoneal perforations that did not cause any consequences, such as emphysema or pneumothorax.
Demographic information was compared in groups 1 and 2 with respect to average age (88 vs. 66.6 months; P > 0.05), sex (50 vs. 70% male; P > 0.05), and operated side (50 vs. 40% right side; P > 0.05). Besides this, we analyzed and compared operating times, mobility, analgesic requirements, hospitalization after surgery, and time to resume feeding. The total operating time, on average, for the TP surgeries was 92.2 minutes (range, 45–160) and 121.1 minutes for the RP (range, 60–200; P > 0.05). Both groups were similar in respect to hospitalization (36.5 hours vs. 28.8, respectively; P > 0.05) and postsurgery analgesic requirements were, on average, 2.1 doses of dipyrone and 1.2 doses of nalbuphine vs. 2.3 and 1.4 respectively (P > 0.05).
The patients operated on when using the RP technique started oral feeding, on average, significantly quicker than those using the TP technique (7.8 hours vs. 14.4; P < 0.05). No patients from group 2 vomited after surgery, whereas 2 of 9 (22.2%) from group 1 had (P < 0.05) delaying oral feeding. No postsurgery complications were noted due to the operating techniques. A 12-years-old girl with vesicoureteral reflux, who underwent a left TP nephrectomy, had to remain hospitalized for 13 days due to having suffered renal hypertension, despite being in good enough condition to leave the hospital after 48 hours, from a surgical point of view. Results and statistics are shown in Table 2.
TP, transperitoneal; RP, retroperitoneal.
Discussion
The first LN was performed by Clayman et al. in 1991, who used the TP technique on an 85-year-old female patient. 6 The first to perform a an RP laparoscopy with insuflation were Roberts 7 in 1978 and Wickham and Miller 8 in 1979. Gaur et al. and Kerbl et al., in 1992, published the first cases of RP laparoscopic nephrectomies in adults,9,10 whereas Chandhoke et al. and Rassweiler et al. did the same with children in 1993 and 1994, respectively.11,12 Since then, a large amount of results have been published on using both LN techniques. The TP approach has shown the advantage of working in a wide space and with easier identifiable anatomic repairs. Nevertheless, the access to the renal hiliar region requires a considerable mobilization and retraction of the bowel; on the other hand, the RP technique has the disadvantage of a smaller active space with an absence of intra-abdominal anatomic structures that are easy to recognize, such as the liver or spleen. At the same time, it provides a direct, faster access to the renal hilius, thereby avoiding bowel manipulation that could produce ileus and delay the recovery of the patient. Renal benign disorder continues to be the main indication in children, although recently, cases of extractions of kidney tumors have been published on using both techniques.13,14 In spite of this, we did not included in our study oncologist indications, and in not one of the extracted materials were malignant signs of tumors found.
Like other adult and pediatric surgeons 15 who are used to performing the initial laparoscopies via the abdominal cavity, we opted for the TP approach to start out the experience, which could affect the final results because these were the first patients in our learning curve. Guilloneau et al. demonstrated a lesser average operating time in performing lumboscopic nephrectomy, and comparing them with the laparoscopic approach 16 ; this probably due to a direct entry via the RP approach in the renal cell without the necessity of abdominal dissection. Lorenzo Gomez and Gonzalez carried out an investigation comparing more than 330 procedures performed by using both methods, where the operating time for the RP approach was also less. 15 On the other hand, the average operating time for our first 10 cases was less than those operated on by the RP approach (92.2 minutes vs. 121.1), but we were not able to show, statistically, this difference (P >0.05), so it is difficult for us to conclude that the TP approach has resulted in our experience as technically more accessible.
Both groups showed the need to convert 1 case. Nevertheless, in group 2, the reason was a technical problem with the equipment during surgery. However, excluding this case, comparing the conversion percentage, the difference was statistically not significant. In group 1, it was decided to convert in an open way on a 7-year-old patient due the massive hydronephrosis and perirenal fibrosis. Rassweiler et al. report an operating time longer in similar cases with a high probability of conversion for severe adhesions and fibrosis. 17 Hemal et al. demonstrated that it is feasible to perform RP nephrectomies with massive hydronephrosis (more than 1000 mL of liquid in the system), 18 but nevertheless, like Valla et al., 19 we do not recommend the initial RP practice on these types of patients. In this study, both approaches were statistically similar with respect to complications during and after surgery, hospitalization, and analgesic requirements.
All the patients could eat again within the first 24 hours. However, those operated on using the RP method were able to eat earlier than those operated on the transabdominal way. It is important to clarify that in the first cases for all laparoscopic surgeries with the TP technique, the postsurgery tolerance in these patients could have been delayed because of a more conservative approach. Nevertheless, 2 patients in group 1 vomited at 10 and 12 hours after surgery, delaying the return to oral feeding. It is interesting to note that in many publications20,21 of nephrectomies performed by the TP approach, there are no details of events, such as nausea or vomiting, early on after surgery, despite the fact that all achieve tolerance within the first 12–24 hours. A prospective, comparative study by Desai et al., 22 using both techniques in 5 of 50 patients, resulted in ileus that lasted longer than 48 hours in transabdominal nephrectomies. However, they could not associate this approach with a large incidence of ileus.
It is for this reason that, today in our institution, the laparoscopic RP approach is the preferred method for the staff and residents to perform nephrectomies. Despite this preference, we have achieved our learning curve with the TP approach, and now, we are quite willing to recommend it to those starting urologic laparoscopy. This study shows that there is comparable security and efficacy in both approaches, but probably, there exist specific situations in which a particular method is more suitable. We believe that it could be beneficial for the patient as well as for the surgeon if the latter can perform both approaches with equal ease, depending on each clinical situation. Finally, the option of the laparoscopic approach for the nephrectomy must depend on the preference and individual training of each surgeon.
Conclusions
LNs can be performed in children with equal efficacy and safely via the transabdominal or RP approach. Both approaches were statistically similar with respect to operating times, complications during and after surgery, hospitalization, and analgesic requirements. Patients operated on by the RP approach had a significantly earlier oral tolerance after surgery. The TP approach can be associated with a minimum ileus within the first 12–24 hours after surgery, delaying slightly the return to oral feeding. We finally believe that the choice of the approach must be in accord with each clinical situation, as well as the preference and training of each individual surgeon, emphasizing and recommending RP procedures, depending on the skills of the surgeon.
Footnotes
Acknowledgments
The authors would like to thank Professor Doctor Azad Najmaldin, MS, FRCS, for the comments and advice made during our research work.
Disclosure Statement
No competing financial interests exist.