
Abstract
Abstract
Introduction:
Outcomes after endoscopic sphincterotomy (ES) and subsequent laparoscopic cholecystectomy (LC) versus laparoscopic bile duct exploration (LBDE) during LC are comparable in fit patients with choledocholithiasis. This randomized, clinical trial aimed to determine the optimum treatment in patients with higher medical risk.
Materials and Methods:
Ninety-one higher risk patients with evidence of bile duct stones were randomized to ES/LC (group A) or LBDE during LC (group B). The primary outcome measure was duct clearance. Secondary outcome measures were complications, number of procedures per patient, conversion, and postoperative hospital stay (POS).
Results:
Forty-seven patients were randomized to ES/LC and 44 to LBDE. The median age was 74.56 years. On an intention-to-treat basis, duct clearance was achieved in 29 of 47 of group A and 44 of 44 of Group B patients (P < 0.001). Clavien Grade II–V complications occurred in 8 of 47 and 8 of 44 patients (P = 0.884), the median number of procedures was 2 (2–3) and 1 (1–1) (P < 0.001), 2 of 47 and 4 of 44 patients required conversion (P = 0.676), and the median POS was 3 (2–7) and 5 (2–7) days (P = 0.825), respectively.
Conclusions:
There was no difference between approaches to duct clearance in terms of postoperative stay, complications, or conversion in higher risk patients, but the laparoscopic approach was more effective and efficient and avoided unnecessary procedures.
Introduction
The question as to whether the gallbladder should be removed after endoscopic sphincterotomy has been answered by, among others, Hammarström et al., 9 who randomised 83 patients to endoscopic sphincterotomy, leaving the gallbladder in situ or open bile duct exploration during cholecystectomy, and followed the patients for at least 5 years. Duct clearance, early complications, and hospital stay were similar in the two groups, but morbidity during follow-up was significantly worse, if the gallbladder was left in situ (28 versus 5%). Eighteen percent required cholecystectomy at a later stage for ongoing or recurrent biliary symptoms and another 15% for other reasons. These results were duplicated by Targarona et al. 10 in a similarly randomized trial of 98 patients. On regression analysis, endoscopic sphincterotomy and leaving the gallbladder in situ was an independent predictor of recurrent biliary symptoms (odds ratio, 6.9; confidence interval, 1.46–32.54). Boerma et al. 11 conducted a randomized, controlled trial of either laparoscopic cholecystectomy or a wait-and-see policy after endoscopic sphincterotomy. Forty-seven percent of the wait-and-see arm had recurrent biliary symptoms, compared with 2% in the cholecystectomy group. Moreover, subsequent conversion and morbidity rates from cholecystectomy were roughly double those in the early cholecystectomy group. Therefore, it is considered best practice to continue with cholecystectomy after endoscopic sphincterotomy in the patient who is fit for general anesthesia.
Laparoscopic bile duct exploration was first employed in the 1990s, but although its use is still not yet widespread, several series of more than 100 patients have now been reported.1,12–34 In these series, the median morbidity is 8%, mortality 1%, with a conversion rate of 4%. Duct clearance rates were greater than 90% in 75% of these series, and there was a retained stone rate of approximately 5%. The reasons for this gradual, rather than revolutionary, uptake in the technique have been the need for surgeons to learn the more advanced skills necessary to explore the bile duct laparoscopically, the initial outlay costs of acquiring the variety of equipment needed to do so, and the more readily available alternative of endoscopic sphincterotomy.
A recent meta-analysis of 591 patients included in five randomized, clinical trials, comparing endoscopic sphincterotomy and laparoscopic cholecystectomy versus bile duct exploration during laparoscopic cholecystectomy, has concluded that the laparoscopic approach seems to be as safe and efficient as endoscopic retrograde cholangiopancreatography and avoids an extra procedure. 35 These trials were performed between 1996 and 2001, were heterogeneous in nature in that two involved preoperative endoscopic sphincterotomy and three postoperative, and they drew upon patients of all ages. In particular, the meta-analysis concluded that duct clearance, as well as morbidity and mortality, rates were similar with a tendency to a shorter hospital stay when laparoscopic bile duct exploration was undertaken, despite the fact that, in some, the experience of the surgeons performing the bile duct exploration was limited and probably not optimal.
It is known that complications from laparoscopic bile duct exploration are associated with increasing age and those with higher medical risk, 36 though Paganini et al. 37 found no increase in morbidity or mortality in patients over the age of 70. However, there is still some concern that the longer operating time required for laparoscopic bile duct exploration, compared with cholecystectomy alone, might incur a greater physiologic insult on the higher risk patient, when compared to the two-stage endoscopic approach, and that the latter might be better suited to higher risk patients. There have been no published randomized trials comparing the two approaches specifically in higher risk patients, and this is the reason for our study.
Materials and Methods
Ninety-one higher risk patients with bile duct stones proven on radiographic imaging, or with strong evidence of them, who were fit enough to undergo general anesthesia and cholecystectomy were randomized to receive endoscopic sphincterotomy and subsequent laparoscopic cholecystectomy or laparoscopic bile duct exploration during laparoscopic cholecystectomy between 2000 and 2006. Ethics approval was obtained from the Southmead Research Ethics Committee. Higher risk patients were defined as being over 70 years of age, over 60 with comorbidity, or those over 50 with a body-mass index of greater than 40. Strong evidence of bile duct stones was defined as those with a dilated common bile duct on transabdominal ultrasound (>5 mm up to 50 years, then 5 + 1 mm per decade) and abnormal liver-function tests. In view of the age of this population, and the practice within the unit, in order to exclude occult carcinomas, the majority of patients (76/91) had bile duct stones proven on radiographic imaging prior to randomization. Only 15 patients (6 in group A and 9 in group B) were included on a strong suspicion of having bile duct stones. Patients were excluded from recruitment into the trial if they had undergone previous endoscopic sphincterotomy, required an emergency sphincterotomy for severe cholangitis or pancreatitis, had had a Billroth II gastrectomy, or if they were unfit for general anesthesia and cholecystectomy. An independent computer-generated random number system was used to allocate treatment.
Data were collected prospectively on a standard pro forma. The primary outcome measure was bile duct clearance. Secondary outcome measures were morbidity and mortality, the number of procedures per patient, conversion rate, and postoperative hospital stay. Postoperative complications were defined as those occurring as a result of surgery (i.e., not just within 30 days) to include complications such as missed bile duct stones, which were defined as those presenting within 1 year of surgery. Complications were classified by using the validated classification system developed by Dindo et al. 38 to allow simple comparison between groups. Briefly, this system stratifies complications into five grades, ranging from any deviation from the normal postoperative course (grade I), those requiring certain pharmacologic interventions (grade II), those requiring surgical intervention (grade III), life-threatening complications (grade IV) to death (grade V).
Sample-size calculations were based on a comparison of known lengths of postoperative hospital stay following endoscopic sphincterotomy (1–11 days) and laparoscopic bile duct exploration (1–26 days) from the literature. 39 Medians were used as an estimate of means in the calculation of standard deviations. Sample sizes of 122 (90% power) or 91 patients (80% power) per group were calculated by using nQuery® (Statistical Solutions, Saugus, MA). Analysis of results was based on an intention-to-treat basis, according to randomization and allocation of intervention. Statistical analyses were performed with chi-Square or Mann-Whitney U tests, with significance set at the 5% level, using SPSS® version 11.0 (SPSS, Chicago, IL).
Operative techniques and protocols employed
Standard techniques were used throughout. All procedures were undertaken by one of two experienced biliary surgeons or by experienced trainees under direct consultant supervision at Southmead Hospital (Bristol, UK).
Intervention A: Endoscopic retrograde cholangiopancreatography and sphincterotomy and subsequent laparoscopic cholecystectomy
After an overnight fast and premedication with 500 mg of ciprofloxacin, the patient was positioned in the prone position receiving supplemental nasal oxygen at 4 L min−1 and monitored with pulse oximetry. Then, 50 mg of pethidine, 20 mg of hyoscine-N-butylbromide, and up to 10 mg of midazolam were administered intravenously (i.v.).
If bile duct stones were confirmed on cholangiography, then sphincterotomy was performed and stones retrieved, using a Fogarty balloon trawl, Dormia basket deployment, and judicious use of mechanical lithotripsy. Duct clearance was confirmed by using balloon-occlusion cholangiography. The techniques of endoscopic electrohydraulic lithotripsy or sphincter balloon dilatation were not employed. If the duct could not be cleared, then an internal biliary stent was placed until subsequent attempts. If no bile duct stones were identified on the initial cholangiogram, a sphincterotomy was not performed. Our extensive audited experience with both procedures before initiating the present study had shown that multiple large stones are more easily treated laparoscopically with reduced potential for complication. We, therefore, deliberately abandoned endoscopic treatment at an earlier stage than in some units where extensive laparoscopic experience is not available.
Laparoscopic cholecystectomy was then carried out on the next available operating list, commonly the following week. Laparoscopic cholecystectomy was performed by using a standard four-port technique. After a wide local dissection of Calot's triangle, the bile duct was imaged with laparoscopic ultrasound (7.5-MHz Aloka linear ultrasound probe; Key Med, Southend, UK) and/or cholangiography to confirm ductal anatomy and ensure that there were no bile duct stones present. 40 If present, the surgeon proceeded to laparoscopic bile duct exploration (see below). Assuming a clear duct, cholecystectomy would then be completed in the usual manner. Gallbladder retrieval bags and subhepatic drains were used selectively. Antibiotic prophylaxis with 750 mg of i.v. cefuroxime was administered only if there was spillage of gallbladder contents during dissection.
Intervention B: Laparoscopic bile duct exploration during laparoscopic cholecystectomy
The gallbladder was approached, as described above. Once ductal stones had been confirmed, the surgeon then decided whether a transcystic or transductal approach was most appropriate. A larger bile duct diameter, larger stones, or multiple stones favored a transductal approach. Choledochoscopy was performed with a three-channel 3- or 5-mm choledochoscope through a transverse incision in the cystic duct or a vertical incision in the common bile duct. Intermittent irrigation with normal saline was used to provide a clear field of view allowing stones to be extracted by using baskets, balloons, and electrohydraulic lithotripsy. Very small stones were flushed transcystically through the sphincter of Oddi under ultrasound visualization with the aid of 20 mg of hyoscine-N-butylbromide given i.v. to relax the sphincter (termed a radiologic exploration). Two passes up and down the duct with the choledochoscope confirmed duct clearance, which was then checked again with laparoscopic ultrasound after clips had been applied to the cystic duct or the choledochotomy had been closed with an absorbable suture. It should be noted that it was often not possible to pass the choledochoscope upward into the common hepatic duct during a transcystic exploration. T-tube drainage of the bile duct was used very selectively in cases where multiple stones or fragments of stones had been removed or when the surgeon was not completely convinced of duct clearance. Biliary stents to protect the choledochotomy were not employed for two reasons. First, there is no scientific evidence to suggest a benefit in their use. 41 Second, instrumentation of the biliary sphincter during laparoscopic exploration of the bile duct appears to be associated with pancreatitis. 42 Cholecystectomy was then completed, and a drain was placed next to any choledochotomy. Antibiotic prophylaxis with 750 mg of i.v. cefuroxime was given if a choledochotomy was made or if there was spillage of gallbladder contents during dissection. Drains were left in place until the first postoperative morning or until bile was no longer present within the drainage bag.
Results
Forty-seven patients were randomized to endoscopic sphincterotomy and subsequent laparoscopic cholecystectomy (group A) and 44 to primary laparoscopic bile duct exploration during cholecystectomy (group B). All patients properly received their intended allocated intervention. During the recruitment period, a further 38 patients were approached for enrollment but declined and chose their method of treatment. The patient characteristics of the two groups are shown in Table 1. There were no significant differences in patient characteristics between groups, except that, proportionally, more patients in group A presented with biliary colic (21/47 versus 10/44 in group B; P = 0.027).
Data is expressed as median (IQR) or n.
The “CONSORT” pathways of patients in groups A and B are shown in Figures 1 and 2, respectively. In group A, bile duct stones were found in 36 of 47 patients at endoscopic retrograde cholangiopancreatography. Further, 26 of 36 patients underwent an apparently successful stone extraction via endoscopic sphincterotomy with the appearance of a clear cholangiogram at the end of the procedure. However, 6 of these patients required bile duct exploration at subsequent laparoscopic cholecystectomy after intraoperative ultrasound revealed stones in the bile duct. The largest bile duct stones retrieved at operation in these patients were 12, 12, 7, 5, 9, and 4 mm at intervals of 242, 18, 14, 10, 4, and 5 days after endoscopic sphincterotomy, respectively. Further, 17 of 26 patients of this group went on to have a laparoscopic cholecystectomy, with no residual duct stones found with intraoperative ultrasound, and 3 chose not to complete treatment and declined cholecystectomy.

Group A “CONSORT” pathway. †One patient in this group presented with a missed bile duct stone 6 months postoperatively and underwent successful endoscopic sphincterotomy and stone extraction. ‡Four of 10 patients had a failed endoscopic extraction, and endoscopic sphincterotomy was abandoned in 6 patients, according to protocol.
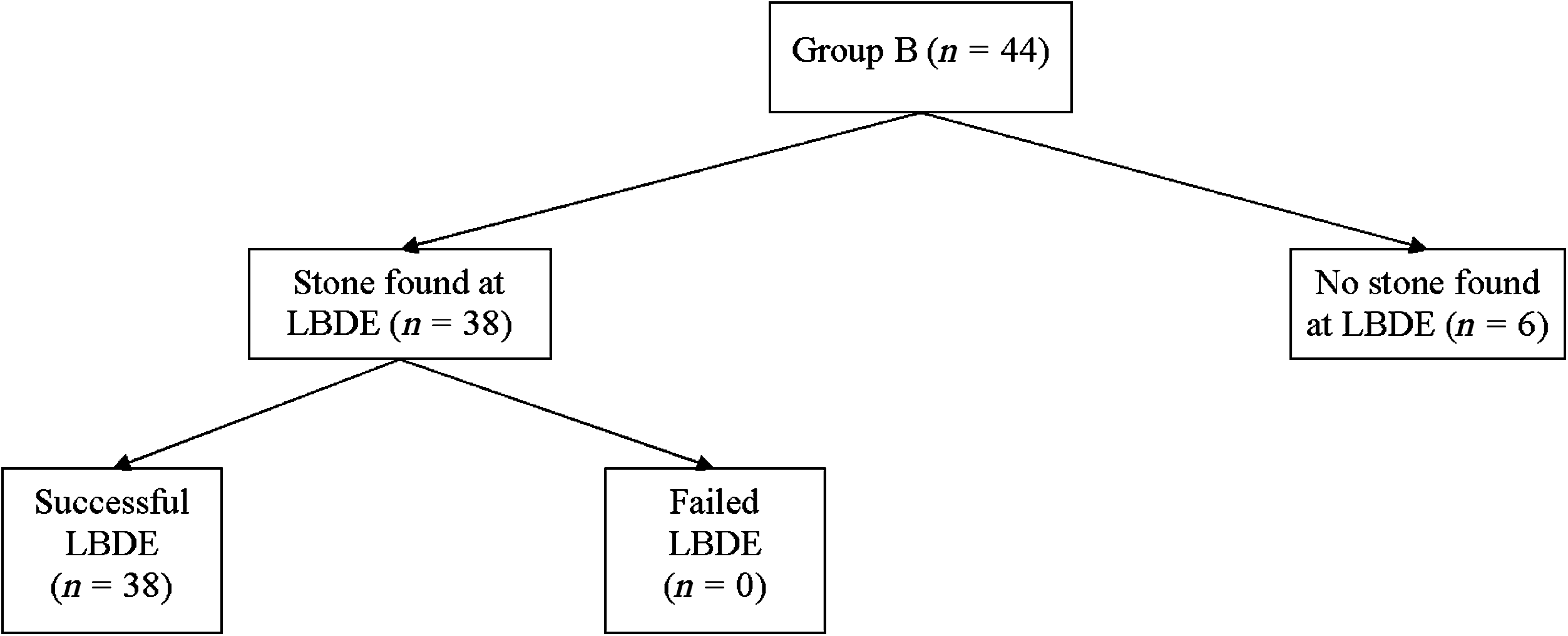
Group B “CONSORT” pathway.
In 10 of 36 patients, stone extraction was not completed at endoscopic sphincterotomy for a number of reasons, and a bile duct exploration was undertaken at laparoscopic cholecystectomy. Endoscopic sphincterotomy failed to clear the bile duct in 4 of 10 patients in whom bile duct stones were found; 2 were intolerant of the procedure, 1 opted for surgery after two endoscopic sphincterotomies, and 1 had a benign distal stricture, not diagnosed on preoperative imaging, below a large stone making endoscopic retrieval impossible. The other 6 patients had multiple large stones, commonly greater than 15 mm in diameter, and stone removal was abandoned according to protocol.
Nine patients in group A had negative endoscopic retrograde cholangiopancreatograms, but 2 of these patients (both of whom had bile duct stones confirmed radiologically prior to randomization) were still found to have duct stones at laparoscopic cholecystectomy and required bile duct exploration. One patient had a 6-mm stone at an interval of 204 days after endoscopic retrograde cholangiopancreatography. This long interval was due to a myocardial infarction after endoscopy. The other patient had a 5-mm stone 5 days after a negative endoscopic retrograde cholangiopancreatogram.
It was not possible to cannulate the bile duct in 2 patients. The procedure was abandoned in 1 patient, after their oxygen saturation deteriorated, and the other had a large complex paraesophageal hiatus hernia, which prevented passage of the endoscope. Of these patients, 1 completed treatment and underwent laparoscopic cholecystectomy with no stone found in the bile duct and the other elected to have no further treatment; a subsequent magnetic resonance cholangiopancreatogram revealed that their ductal stone had passed spontaneously. The median interval from completion of endoscopic treatment to laparoscopic cholecystectomy was 13 days (interquartile range; IQR, 5–29).
Thus, 18 of 47 patients in group A required bile duct exploration (15 transductal, 2 transcystic, and 1 radiologic) at laparoscopic cholecystectomy for reasons mentioned above. In 8 of these instances, this followed an apparently clear endoscopic cholangiogram, after stone extraction in 6 and without stone extraction in 2 patients. The interval to laparoscopic cholecystectomy was within 18 days in 6 of 8 of these patients.
In group B, 38 of 44 patients were found to have stones at laparoscopic cholecystectomy, all of which were extracted laparoscopically (30 transductal, 5 transcystic, and 3 radiologic). Two of the 6 patients who were found not to have bile duct stones at operation were entered into the trial “on a strong suspicion” of bile duct stones only. T-tube drainage was used without incident in 4 patients in group B. On an intention-to-treat basis, the allocated intervention achieved duct clearance in 29 of 47 patients of the endoscopic sphincterotomy group (group A) and 44 of 44 of the laparoscopic bile duct exploration group (P < 0.001).
Complications occurred in 14 of 47 and 19 of 44 patients in groups A and B, respectively, and are listed in Tables 2 and 3. A controlled bile leak was defined as bile within the drainage bag the following day without systemic upset. There was no significant difference (P = 0.884) in the occurrence of relatively severe Clavien grade II–V complications between groups (8/47 and 8/44, respectively).
LBDE, laparoscopic bile duct exploration; ERCP, endoscopic retrograde cholangiography; LC, laparoscopic cholecystectomy; ES, endoscopic sphincterotomy.
Sixty-five endoscopic retrograde cholangiopancreatograms were performed on the 47 patients in group A (range, 1–3). Consequently, more procedures in total were performed in group A than B (median of 2 (IQR 2–3) versus 1 (IQR 1–1); P < 0.001). Conversion to an open procedure was necessary in 2 of 47 patients in group A and 4 of 44 in group B (P = 0.676). In all cases, conversion was due to dense gallbladder adhesions and fibrosis, rather than any difficulty with the bile duct. Two of these patients had successfully undergone bile duct exploration laparoscopically prior to the need to convert to an open operation. The median total postoperative stay after all procedures was 3 (IQR, 2–7) days in group A and 5 (IQR, 2–7) days in group B (P = 0.825).
All living patients have been followed up for at least 1 year. The median length of follow-up is 1.88 (IQR, 1.38–3.15) years. There have been 6 deaths due to unrelated disease during this time, 2 in group A and 4 in group B. One further death occurred in group B due to carcinoma of the pancreas in a patient who was diagnosed after investigation of persistent jaundice following bile duct exploration and stone removal where preoperative magnetic resonance cholangiopancreatography had not identified a tumor. The latest follow-up information was obtained by direct contact with the patient in 76 of 84 of living patients and via the patients' general practitioner in the remaining 8. Two patients have presented with choledocholithiasis during follow-up so far. In group A, 1 patient presented with a missed bile duct stone 6 months postoperatively, and in group B, 1 patient presented after 2.3 years with a recurrent stone; both patients have been successfully treated endoscopically (in our experience, we feel that it is reasonable to assume that a stone presenting within a year was one that was missed at surgery). No clinically apparent biliary strictures have been detected during follow-up.
Discussion
The laparoscopic removal of bile duct stones in all comers offers advantages over the endoscopic approach: equivalent removal of duct stones with fewer procedures, reduced cost, and preservation of the biliary sphincter. When laparoscopic bile duct exploration is employed, the operation is longer. Consequently, in elderly patients and those with significant comorbidity who may not tolerate longer procedures, the advantage may be lost. This study was performed to see if this was the case or whether any advantage remained. The results show a continuing advantage for the laparoscopic approach. There was better clearance of the bile duct (100% in the laparoscopic group) with fewer procedures per patient. This was achieved without any increase in the rate of complications or in the length of stay, when compared to endoscopic sphincterotomy and cholecystectomy in the same patients.
These patients underwent extensive diagnostic tests, largely to exclude malignancy. Despite this, 14% of patients in the bile duct exploration group had no stones found at operation, this being established by laparoscopic ultrasound, a technique with better sensitivity and specificity than intraoperative cholangiography. 43 In the endoscopic sphincterotomy group, 23% of patients had no duct stones at the initial procedure. Thus, about one fifth of patients apparently presenting with bile duct stones would undergo unnecessary endoscopic retrograde cholangiopancreatography, if this approach was the chosen one.
The stones, in some of these patients, were large and numerous, probably a feature of the age of the population. (The rate of transductal exploration in group B of 79% is very high and associated with larger stones than seen in younger patients.) Our previous, substantial, and audited, experience 12 had shown us that duct clearance of multiple large stones could usually be achieved relatively easily laparoscopically but is more difficult with greater potential for complication endoscopically. We, therefore, abandoned the endoscopic route earlier, in 6 patients, than some would have done. Institutions with particular expertise in endoscopic sphincterotomy and the management of “difficult” choledocholithiasis publish impressive duct clearance rates. Mechanical lithotripsy has been shown to be successful in 80–90% of those with stones greater than 15 mm in diameter, but complication rates rise with increased instrumentation of the duct.44,45 The largest series, to date, of electrohydraulic lithotripsy reports a duct clearance rate of 96% in difficult stones, but greater than 10% of cases were subsequently complicated by biliary obstruction. 46
In this study, where the endoscopic route was used as the sole intended means of clearing the duct, the perceived success rate at the end of endoscopic therapy was 85% (35/41; 4 failed extractions and 2 failed cannulations). These results in the endoscopic arm of the trial might be interpreted as suboptimal by some, but they are consistent with results from others worldwide 8 and better than the average of those presented in a recent survey of endoscopic retrograde cholangiopancreatography practice within the UK. 47 An alternate approach to study design would have been to have had independent endoscopists who may have strived for higher duct clearance rates by means of more aggressive endoscopic intervention rates. However, the same difficulty would have arisen in determining a suitable end-point for attempted endoscopic removal of stones, as an alternative satisfactory surgical treatment was available. The result is a trial of relatively conservative endoscopic sphincterotomy against laparoscopic duct exploration and would, therefore, favor endoscopic sphincterotomy in terms of complications and, perhaps, length of stay. Indeed, only two relatively minor complications related to sphincterotomies were encountered in the 65 endoscopic procedures undertaken, fewer than expected from other studies.48,49
There were 6 patients who had a negative occlusion cholangiogram after endoscopic duct clearance but still had stones at operation. This phenomenon has been described previously,50,51 but measurement of it demands an extremely early reassessment by an alternative approach. We have established the inferiority of operative cholangiography, compared to laparoscopic ultrasound, 43 so it is likely that occlusion cholangiography missed stones. Practical difficulties in the scheduling of patients for a laparoscopic cholecystectomy, limited by the health care system, probably resulted in some stones entering the bile duct in the interim. Thus, an assessment of the bile duct at the time of laparoscopic cholecystectomy is clearly worthwhile even after apparent clearing of the ducts endoscopically.
It was postulated that there might be more morbidity in this group of higher risk patients manifest as an increased rate of complications and of length of stay. This has proved partly to be the case. Morbidity from our previous experience of all-comers undergoing laparoscopic bile duct exploration 12 was 19%, compared to 43% in this study. This may be a result of age, comorbidity, and a higher rate of transductal exploration in the current group. Nevertheless, the endoscopic group fared no better. There were very few Clavien II–V complications in either group, which may explain why the increase in complications was not mirrored by an increased length of stay. The higher rate of transductal exploration in group B was associated with a postoperative stay of 5 days, similar to the 4.8 days following transductal exploration for all-comers previously described. The relatively short-term follow-up in this study has found a missed stone in the endoscopic group and a recurrent stone in the laparoscopic group. Previous studies would suggest a recurrence rate of 1% per annum after sphincterotomy.52,53 Preserving the sphincter by using a laparoscopic approach, which may lead to a reduction in recurrent stone formation, when compared to endoscopic sphincterotomy, 54 may be less valuable in the elderly, as decreasing sphincter tone with age might allow duodenobiliary reflux and the formation of primary bile duct stones.
Conclusions
With the proviso that this study was performed within a unit known to have extensive experience of laparoscopic bile duct exploration and, perhaps, a relatively conservative approach to endoscopic therapy, we would conclude: In elderly or higher-risk patients who are fit for surgery, a laparoscopic cholecystectomy and bile duct exploration can achieve better duct clearance with fewer procedures than endoscopic sphincterotomy and subsequent laparoscopic cholecystectomy, with no increase in complications or hospital stay.
Footnotes
Disclosure Statement
No competing financial interests exist.
This work was presented in abstract form at the Annual Meeting of the Association of Surgeons of Great Britain and Ireland in Manchester, UK, April 18–20, 2007.