
Abstract
Abstract
Ten-millimeter ports are often used in laparoscopic surgery. Closure of these port sites can be difficult. In this article, we describe two novel methods of closing 10-mm laparoscopic port-site wounds, which are simple, effective, easy, and do not require any special instruments.
Introduction
Novel Method Using the Port Sheath
Once the intra-abdominal part of the laparoscopic procedure is completed, gas is let out. The 10-mm ports are retained and used to elevate the abdominal wall by angling them to 30 degrees. Langenbecks retractors are used to retract the skin around the port to expose the underlying fascia. An appropriate stitch, according to the surgeon's preference, is used to insert a good bite onto the rectus sheath, and the same method is repeated on the other side. In this method, the stitch goes through the peritoneum and both anterior/posterior fascial layers (i.e., full thickness). The surgeon can easily see and feel the full-thickness nature of the stitch. We use a J-needle with 0-PDS (Ethicon, Summersville, NJ) and prefer to take offset stitches at the opposite corners for maximal approximation.
Novel Method Using Two Langenbecks Retractors
If you have removed the port sheath by mistake, you can insert an appropriate-size Langenbeck's retractor into the 10-mm port and lift the port-site wound. Another Langenbeck retractor is used to retract the skin, exposing the fascia. Then, using a J-needle with PDS, you take a stitch from the corner, which is away from the retractor. Then, change the direction of the Langenbeck's retractor and take another bite from the opposite corner. Using this technique, one may avoid struggling to stitch the fascia. It will be very useful in obese patients. Other retractors can be substituted in place of the Langenbeck's.
Discussion
Closing the 10-mm port wounds has been described with using the Endoclose® (Covidien, Norwalk, CT) and Gore suture passer® (W.L. Gore & Associates, Inc., Flagstaff, AZ), a Reverdin needle, or various other suture-passing devices. All instruments are variations on the cobbler's awl, used to feed a stitch across the opposing edges of the fascia, and control is intraperitoneal, requiring prolonged insufflation time. All require specialized equipment. Our methods use instruments available on any standard set, and control is by direct vision with the abdomen dessuflated. The main aim of both of our port closure methods is full thickness approximation of rectus sheath/fascia as illustrated in Fig. 1.
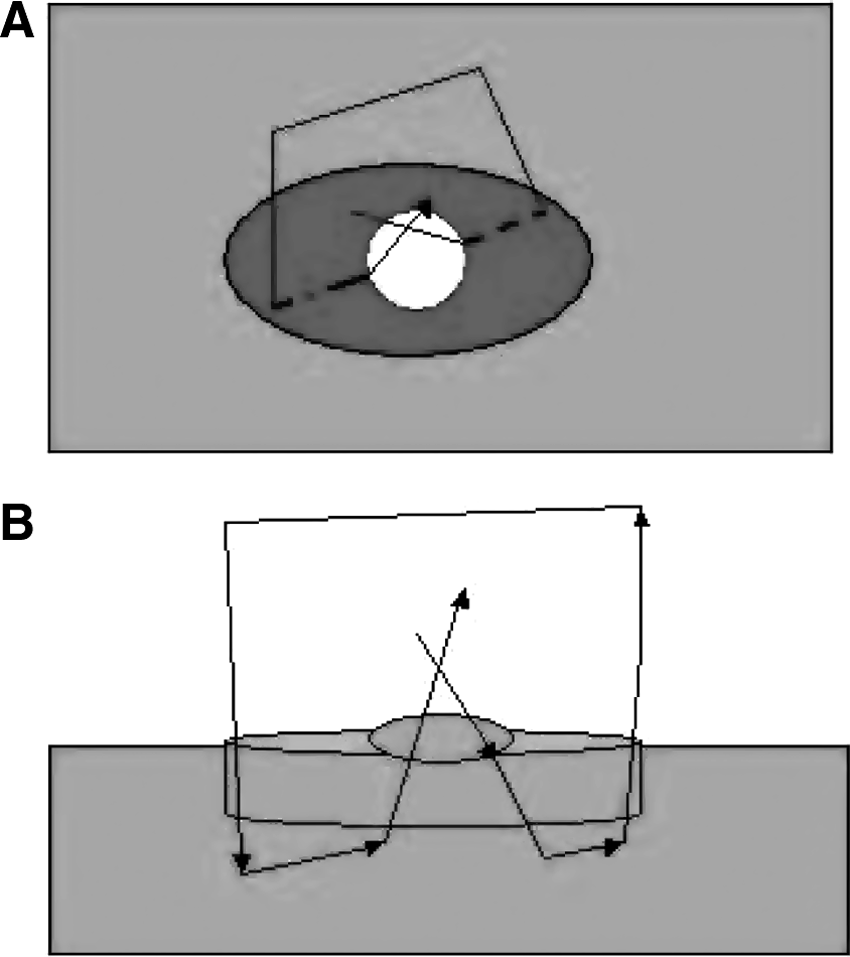
(
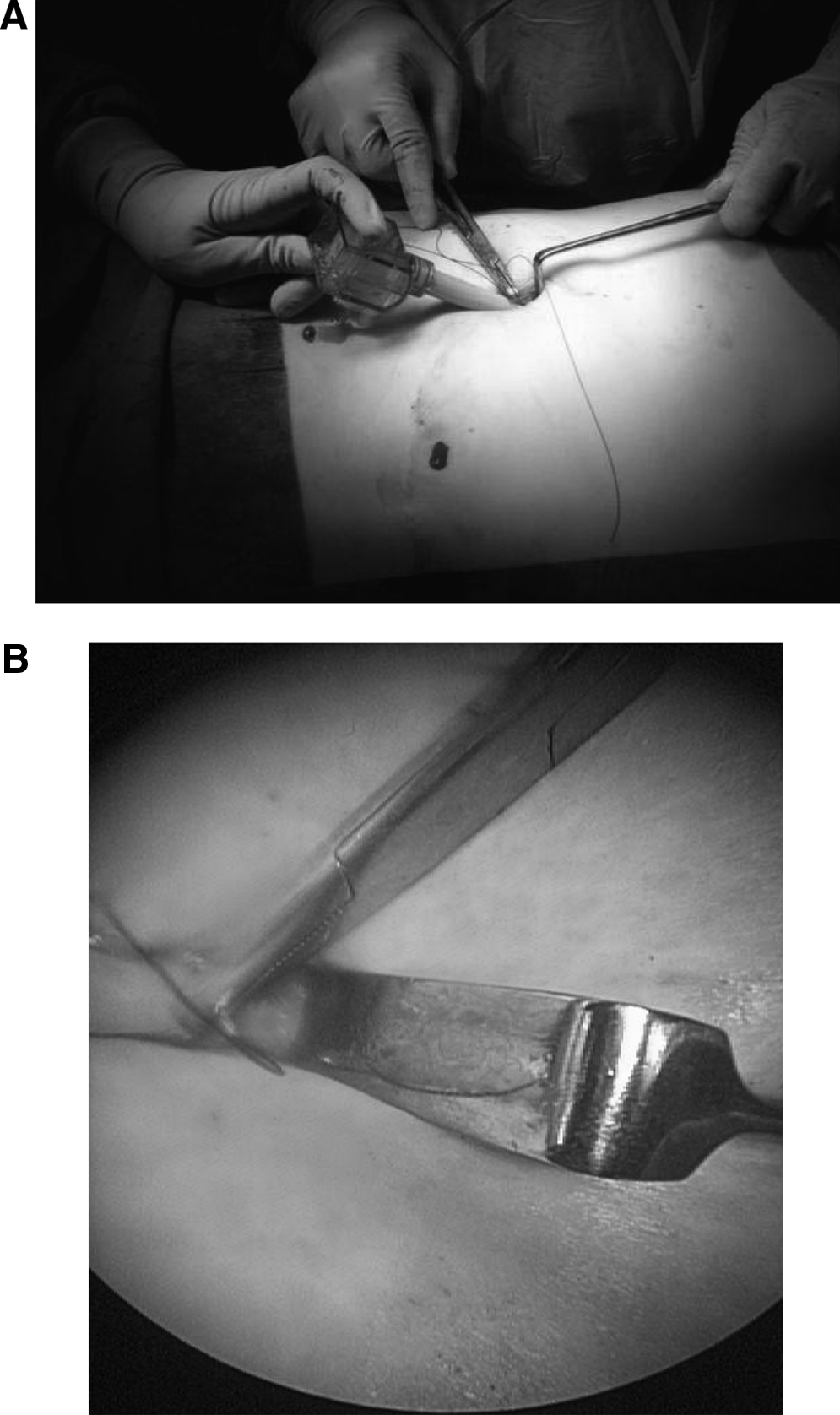
In our first method (Figs. 2 and 3), retaining the port and using it to elevate the sheath not only exposes it, but also moves any underlying structures away. In the second technique (Figs. 4 and 5), lifting the abdominal wall with the first Langenbeck retractor allows the bowel underneath to drop away. Using the second retractor to expose the sheath allows precise insertion of the J-needle at opposing corners. Usually, only one stitch is required. As far as we know, our methods have not been described before. We have used this technique on >2000 patients over a period of 18 years. Our patients undergoing laparoscopies usually have at least one 10-mm port, and in cholecystectomies and selected cases of difficult appendicetomies, one more 10-mm port was used. All patient received a follow-up appointment at 6 weeks and, if required, again in 3 months. The port sites were specially clinically assessed for any hernias. None of our patients developed a port-site hernia. This was specifically because of the full-thickness nature of the stitch, which goes through both fascial layers as well as the peritoneum. They are low in cost, reliable, efficient, fast, safe, and simple.
(

(
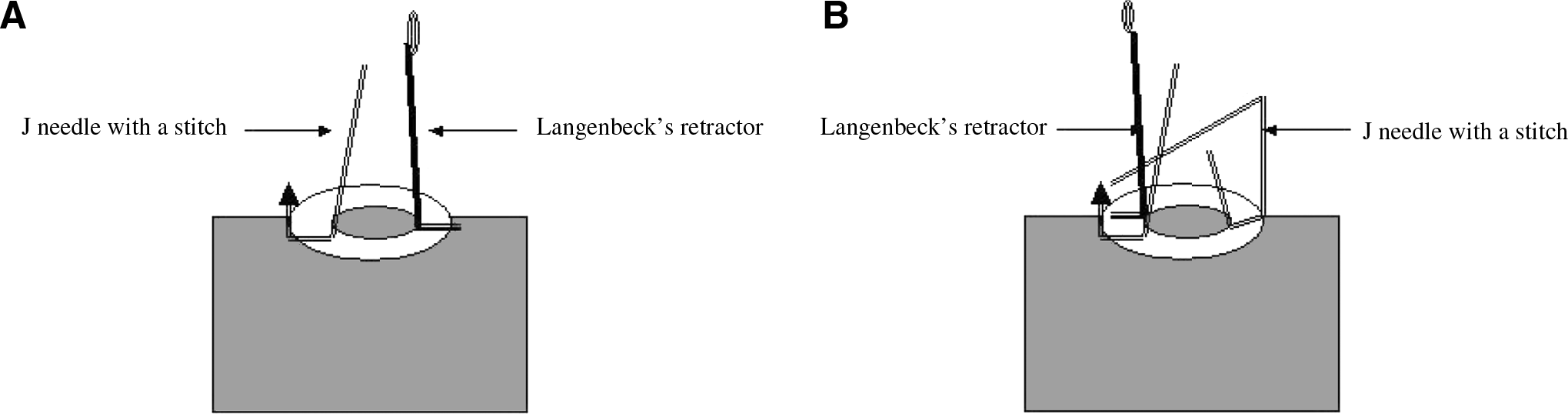

Figure showing the lift technique in practice, using two Langenbeck's retractors.
Conclusions
The methods are easy to learn and reproduce. The only limitation is that the wound has to be large enough to accommodate the chosen retractor and needle. We did not encounter any complication because of our technique.
Footnotes
Disclosure Statement
No competing financial interests exist.