
Abstract
Abstract
Introduction:
A wet colostomy can be done when the simultaneous diversion of fecal and urine streams are necessary. Laparoscopic access is gaining space in urinary diversion procedures. The aim of the present study was to present the technique and results of the first case reported of a video-assisted double-barreled wet colostomy.
Patient and Methods:
In this article, we report a case of a 50-year-old woman with actinic complex urinary and fecal fistula, treated through a retroperitoneoscopic double-barreled wet colostomy. Only the left kidney had function, so she was treated by video endoscopic retroperitoneal dissection of the left ureter, preplanned transverse 5-cm incision for exteriorization of left colon and ureter, extracorporeal section of the left colon with a linear stapler, extracorporeal antireflux ureterocolonic anastomosis, and maturation of the stoma 10 cm proximal to the end of the proximal colonic loop.
Results:
Operative time was 135 minutes. No transfusion was required nor had intraoperative complications occurred. Oral intake was initiated in postoperative day 2, and the patient was discharged postoperative day 6 without complications. Normal activities were recovered after 21 days. In a 3-month follow-up, there were no infectious complications, and good urinary drainage was observed. She was satisfied and adapted to the stoma.
Conclusions:
Video-assisted double-barreled wet colostomy is a feasible procedure. The same goals of the open procedure were achieved, offering the advantages of the laparoscopic approach.
Introduction
In 1989, Carter et al. 7 described the double-barreled wet colostomy, which consisted of a colonic loop diversion, anastomosing the ureters 10 cm distally to the stoma. The rationale was to create a distal reservatory with free urine flow and without feces. It is a simple, safe procedure that keeps urine apart from the fecal stream, reducing the risk of infection. Moreover, colonic segments, different from the small bowel, are, in general, protected from radiation effects. Since Sanchez de Badajos et al. 9 have described an experimental model for performing endoscopic ureteroileostomy with extracorporeal urinary diversion, many researchers have performed laparoscopic and robotic-assisted urinary diversion, whether with intra- or extracorporeal anastomosis.10,11 Although technically challenging, ongoing technical refinements of reconstructive laparoscopy are making these procedures more widely applicable. 12 We treated a patient with a complex urinary and fecal actinic fistula, which needed double diversion. We duplicated Carter's procedure laparoscopically and, in this article, describe our experience with this new minimally invasive option for simultaneous urinary and fecal diversion.
Patient and Methods
A 50-year-old woman had been successfully treated for a stage IIb cervical carcinoma through Wertheim-Meigs surgery associated with adjuvant radiotherapy 8 years previously. Three years after surgery, she developed vesicovaginal fistula and underwent multiple surgical procedures. She had a nonfunctioning right kidney and finally presented with a complex fistula-communicating rectum, vagina, and bladder. After discussing options, she decided to undergo a simultaneous urinary and fecal diversion.
The patient was positioned on the table in the right modified flank-position, allowing maximal retroperitoneal exposition. After an initial 1.5-cm paravertebral incision, the index finger was used to create a retroperitoneal space and place the dilatation balloon. We used a homemade glove-finger balloon, filled with 800 mL of saline. It is important to dissect between the Psoas muscle and the kidney, preserving the peritoneum intact. Two 10-mm paravertebral trocars were placed, one below the 12th rib and the other in Petit's triangle. Another 5-mm trocar was placed anteriorly to achieve a good triangulation (Fig. 1). The left ureter was dissected to the iliac vessels, where it was sectioned, obtaining enough length to perform the colonic anastomosis. The peritoneum was then incised and the descending colon reached at the same level of the ureter. A preplanned 5-cm transverse laparotomy was then performed to achieve exteriorization of the colonic loop and ureter. The left colon was then transected with a linear endoscopic stapler 10 cm bellow the area where the ureter was anastomosed. The double-barreled colostomy was then brought to the skin (Fig. 2A).
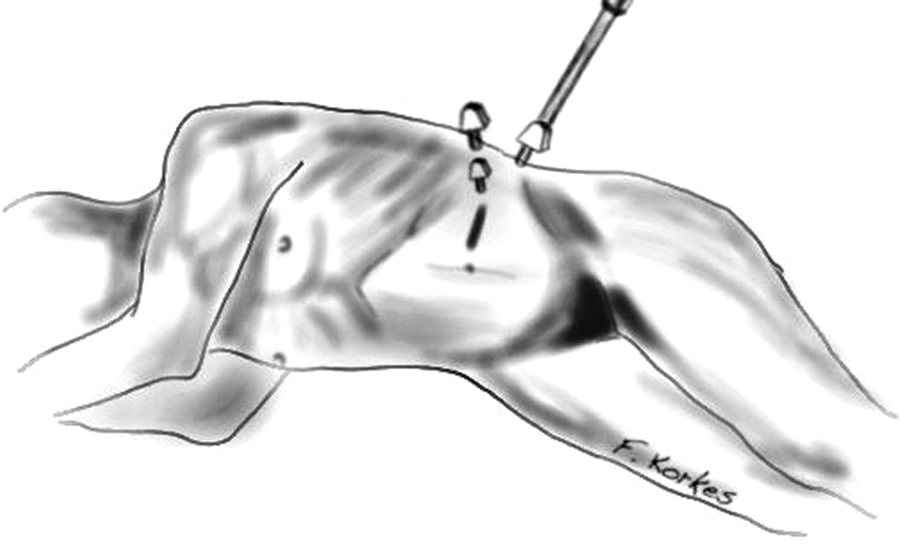
Patient and trocars position.
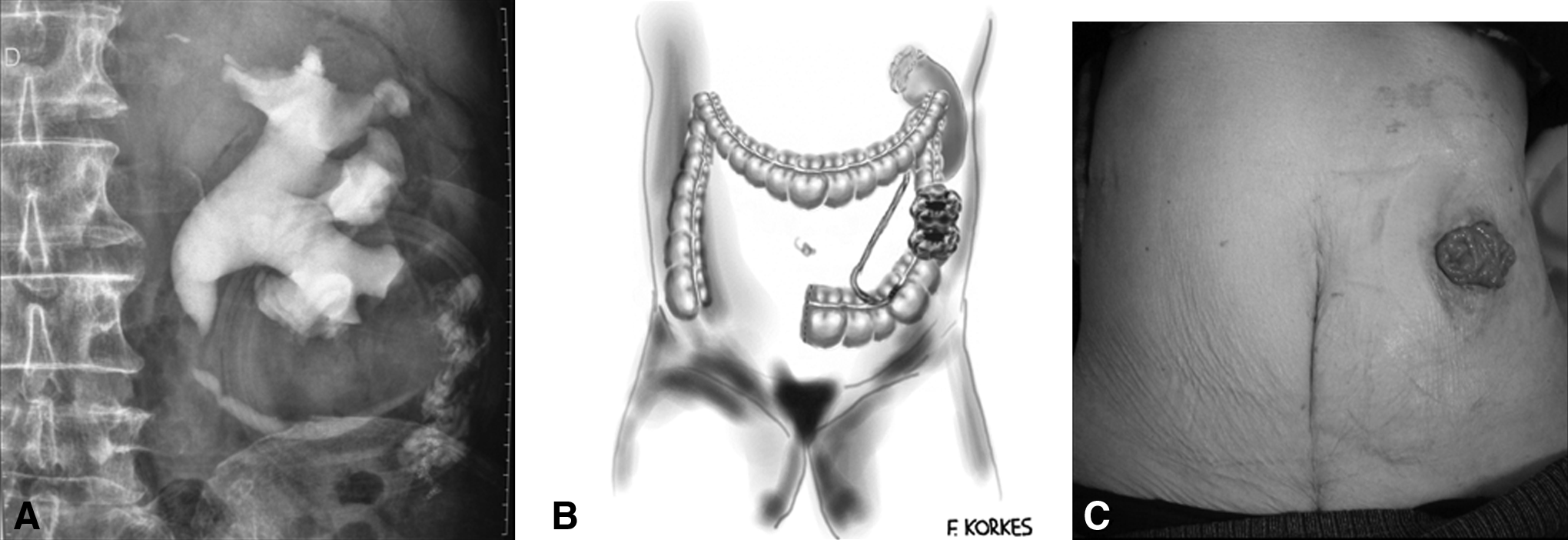
Postoperative aspect of laparoscopic double-barreled wet colostomy. (
Results
No blood transfusion was required, and operative time was 135 minutes. Oral intake was initiated in postoperative day 2, and patient was discharged after removing the ureteral stent and drain postoperative day 6. No complications were observed. Recovery to normal activities occurred after a 21-day period. After a 3-month follow-up she was satisfied, adapted to the stoma, and had no infectious complications. The intravenous urogram demonstrated good urinary drainage and renal function (Fig. 2B). Stomal and skin aspects were unremarkable (Fig. 2C).
Discussion
Urinary tract reconstruction is a key to exenterative surgery, as it contributes to a significant increase in morbidity and mortality. Severe complications after consecutive procedures may lead to complex fistulae, involving the rectum, bladder, and vagina. Advances in surgical techniques and peroperative care have also required simultaneous advances in reconstructive surgery. Traditionally, two stomas are required with an ileal conduit: a urostomy in the right quadrant and a terminal colostomy in the left quadrant.13–15 In this setting, intestinal diversion generally brings additional problems to daily care. The confection of two stomas is also associated with longer surgery and more complications, mainly in patients with prior radiotherapy or previous abdominal surgeries. It is associated with more cumbersome daily care and thus reduces patient acceptance.16–18
Double-barreled wet colostomy is a good alternative for patients who need concomitant urinary and fecal diversion. After conventional wet colostomy, acquosal diarrhea occurs. Double-barreled wet colostomy is performed, leaving the distal 10–15-cm colonic segment to ureteral anastomosis and performing a loop colostomy proximally. After this procedure, a continuous urine flow occurs apart from a semisolid fecal output, contributing to a better quality of life. Separate exoneration of urine and fecal content is obtained through only one stoma. In this manner, if the patient removes fecal content after evacuation, there are few problems concerning weight inside the bag. Peristomal skin must be perfectly protected, leaving the bag tight to the colonic stoma in order to prevent the contact of urine with the skin. Complications of this procedure are minimal, but pyelonephritis, metabolic disturbs, hydronephrosis, fistulae, dehiscence, and stenosis have been reported.7,16,17,19,20
If an oversized reservatory is built, stasis occurs and leads to high urine absorption and hypercloremic-hypokalemic acidosis. It can be avoided by building a short distal reservoir, thus reducing residual volume and stasis. Some researchers have advocated that reservoirs with 10–25 mL capacity allow good urinary flow, effective contraction, and prevent from urinary tract infections.16,17 Carter's procedure has been performed by several researchers without further complications, but is mostly performed right after pelvic exenterative surgery, implicating longer operative time, length of stay, and increased morbidity. Median operative time, in recent series, is 235 minutes, with an average hospital stay of 15 days, 33–43% morbidity, and 3.3% mortality rates.19,21,22 Table 1 demonstrates current experience with such procedures.
The laparoscopic route has brought the advantages of minimally invasive procedures to urinary diversion either with intra- or extracorporeal anastomosis, especially after radical cystectomy and exenterative pelvic surgery. The present report aims to demonstrate that these benefits can also be obtained when performing a simultaneous urinary and fecal diversion. It has been previously suggested that laparoscopic cystectomy with an ileal conduit is associated with lower blood loss, postoperative analgesic requirements, shorter length of hospital stay, and earlier return of bowel function than open cystectomy. 23 The use of a titanium linear stapler to urinary reconstruction aims to further reduce operative time. Preliminary reports evaluating the feasibility and safety of the titanium stapler for the intestinal neobladder have demonstrated that urinary stones occur in about 5% of cases, similar to neobladders built with nonabsorbable sutures.24,25 Additionally, laparoscopic-assisted creation of stomas seems to result in faster recovery with similar operative time and improvement in cosmetic appearance. 24 Robotic surgery might also shorten the learning curve, as described for other procedures.26,27 Table 2 demonstrates other researchers' experience with laparoscopic and robotic-assisted urinary diversion procedures.
Radical cystectomy + extracorporeal diversion (diversion mean time, 75 minutes). ICRA, intracorporeal robot-assisted anastomosis; ECLA, extracorporeal laparoscopic-assisted anastomosis.
Video-assisted double-barreled wet colostomy, as described by Carter et al., is a safe, efficient alternative for patients that need simultaneous urinary and fecal diversion. By maintaining an intermittent fecal and continuous urine flow, 21 it provides a better quality of life. Additionally, the laparoscopic approach brings the advantages of minimally invasive procedures. Peroperative and functional outcomes seems to be better than after open surgery,28,29 even though larger studies might bring additional information. Extracorporeal anastomosis, as currently performed, has the advantage of being faster, but also allowing a safe anastomosis. To the best of our knowledge, this is the first report of a minimally invasive simultaneous urinary and fecal diversion, and some important technical aspects might be reinforced. The transperitoneal approach seems to be better when both ureters are to be reimplanted; when the right ureter is too short to be brought through the colostomy incision, a small median incision might help ureterocolonic anastomosis. Even though the present case was performed extraperitoneally, our preliminary results are encouraging, when compared to conventional open surgery.
Conclusions
In conclusion, video-assisted double-barreled wet colostomy is feasible, guarding the advantages of a laparoscopic approach. Extracorporeal anastomosis is more advantageous, in our opinion, and satisfactory cosmesis is also guaranteed. Reproducibility by other surgeons and larger series are required to further evaluate safety, morbidity, and mortality rates of this new approach.
Footnotes
Disclosure Statement
No competing financial interests exist.