
Abstract
Abstract
Background:
Primary spontaneous pneumothorax in children is a significant clinical problem. The majority of these patients will require immediate surgical therapy, such as tube thoracostomy.
Patients and Methods:
We conducted a retrospective review of 16 patients with a diagnosis of primary spontaneous pneumothorax over a period of 7 years.
Results:
In the last 7 years, we had 16 patients with spontaneous pneumothorax. Patient age ranged from 11 to 18 years (median, 15.4). We had 12 boys and 4 girls. Pneumothorax occurred on the right side in 9 patients, on the left side in 6 patients, and on both sides in 1 patient. The first choice of treatment was tube thoracostomy. The main symptoms were chest pain, shortness of breath, and cough. In all patients, we made X-ray and computed tomography scan. In 10 children, we detected apical bullas; in 2 patients, we found giant bullas in the lower part of the lung. In 4 patients, we did not find any pathologic signs on the lung. Two patients with spontaneous pneumothorax had tube drainage without recurrence. Eleven patients were operated on with video-assisted thoracoscopic surgery (VATS). Three patients were operated with open thoracotomy. Two of them had giant bullas, and 1 patient had recurrence after VATS. One patient had pneumothorax on both sides of the pleural cavity.
Discussion:
VATS is an effective, safe method for spontaneous pneumothorax in children. In 11 children with pneumothorax, we made a wedge resection of the apical part of the lung with an endostapler device plus mechanical pleurodesis.
Introduction
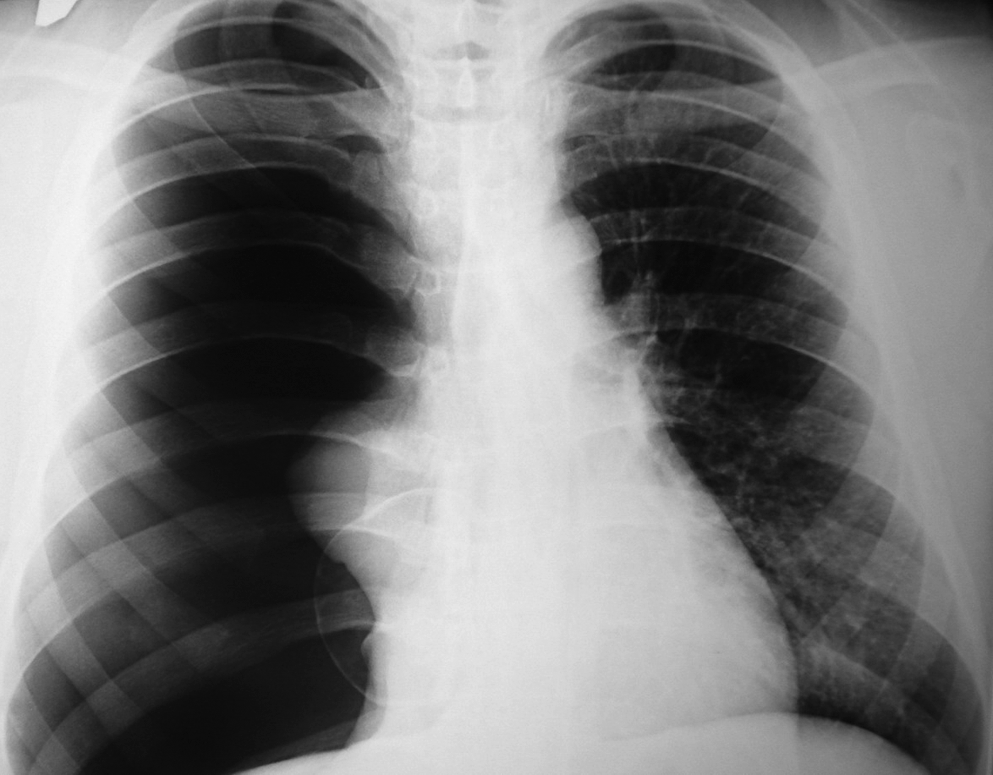
Complete pneumothorax.
Treatment of the spontaneous pneumothorax is greatly varied from observation, tube thoracostomy, video-assisted thoracoscopic surgery (VATS), or thoracotomy. Always, the first line of treatment is tube thoracostomy with observation. If an air leak is persistent, VATS is the method of choice, with a wedge resection of the apical part of the lung with an endostapler device plus mechanical pleurodesis. Before VATS, radiologic investigations [e.g., X-ray and computed tomography (CT) scan] were done. 7 Two patients had giant bulla, and an open thoracotomy was done after tube thoracostomy; 1 patient had a recurrence after VATS, and we decided to perform an open thoracotomy.
Approximately one half of the patients who receive conservative therapy will have a recurrence. 8 We started with tube thoracostomy in all 16 patients. Only 2 patients did not have any surgical procedure, because a significant air leak or recurrences were not noticed after chest-tube suction.
Materials and Methods
In December 2001, the VATS technique was initiated at our hospital. Before that time, we used two methods for spontaneous pneumothorax: conservative treatment with tube thoracostomy and aspiration or open thoracotomy. After December 2001, in all patients with spontaneous pneumothorax, VATS was done. Only in 2 patients with giant bulla did we make an open thoracotomy. In all patients with chest pain or dyspnea who came in our hospital, we made plain chest radiographs. When we found a pneumothorax, we investigated patients for chest trauma, chronic pulmonary diseases, or some other cause of the pneumothorax. In treatment, we always started with intercostal tube catheter drainage, aspiration, and observation. If patients had a continuing significant air leak that did not stop for several days (range, 5–6), VATS was indicated. Today, VATS has a central role in the treatment of spontaneous pneumothorax. 9
In the last 7 years, we had 16 patients with spontaneous pneumothorax. The patients ranged from 11 to 18 years in age (median, 15.4). We had 12 boys and 4 girls. Pneumothorax occurred on the right side in 9 patients, on the left side in 6 patients, and on both sides in 1 patient. The first choice of treatment was tube thoracostomy. The main symptoms were chest pain, shortness of breath, and cough. All patients with pneumothorax had sudden, powerful chest pain, shortness of breath that we noticed in 9 (56%) patients, and cough in 2 (12.5%) patients.
We developed algorithm for the management of spontaneous pneumothorax in children (Fig. 2). When children presented in the hospital with chest pain, shortness of breath, dyspnea, and cough, we made a plain roentgenogram. If we noticed a pneumothorax, we always started with intercostal tube catheter drainage, aspiration, and observation. If there was significant air leak that did not stop for several days (range, 5–6), VATS with mechanical pleurodesis was indicated. Sometimes, conservative treatment was successful, but recurrence was too high. VATS is the method of choice for patients with bullas in CT scan, in patients with recurrence, or in patients with prolonged air leakage at the first episode of a pneumothorax. In patients with giant bullas, we recommended an open thoracotomy. Only 2 patients did not have any surgical procedure, because significant air leak or recurrence was not noticed after intercostal tube catheter drainage and aspiration.
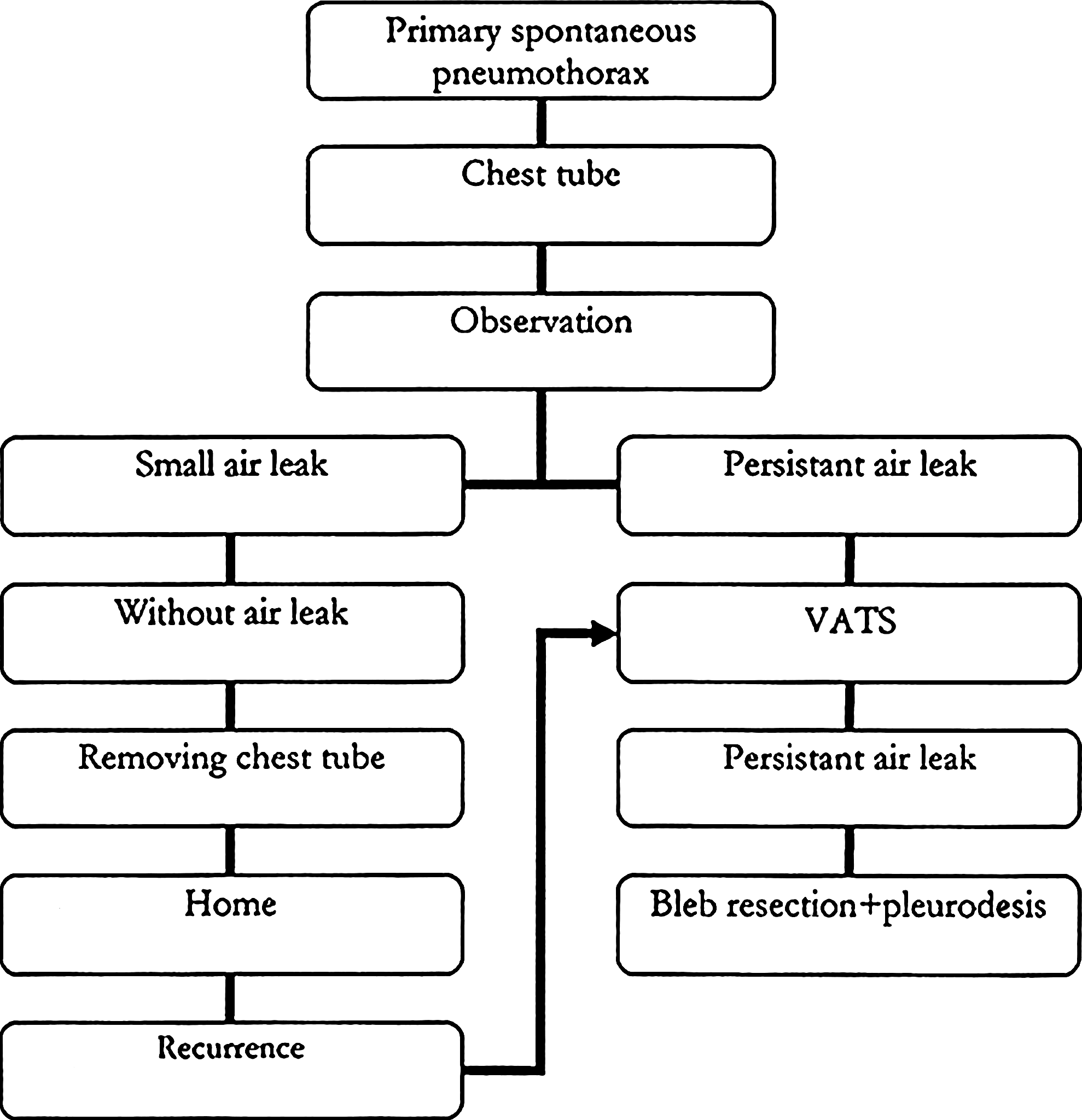
Algorithm for the management of primary spontaneous pneumothorax in children.
Results
In the last 7 years, we had 16 patients with spontaneous pneumothorax. The patients ranged from 11 to 18 years (median, 15.4). We had 12 boys and 4 girls. Pneumothorax occurred on the left side in 9 patients, on the right side in 5 patients, and on both sides in 2 patients. Primary spontaneous pneumothorax is most common in tall, slim, and thin children who have a higher transpulmonary pressure in the apex. 7 All patients with pneumothorax had sudden, powerful chest pain, shortness of breath that we noticed in 9 (56%) patients, and cough in 2 (12.5%) patients. In all patients, we made a plain roentgenogram and, later, a CT scan.10,11 Of the 16 patients, CT scan showed 10 children with apical bullas and blebs, and in 2 patients we found a giant bulla in the lower part of the lung. In 4 patients, we did not find any pathologic signs on the lung. In all patients with apical bullas, VATS was indicated. Also, in patients without pathologic signs on CT scan, but with prolonged air leak, we had done a VATS procedure. In all patients, we indicated intercostal chest-tube catheter drainage, aspiration, and observation. After 5 days, in 2 patients, air leaks disappeared and chest tubes were removed. After removing the chest tube, we did not notice any significant air leak or recurrence. Both children, 5 years later, were without recurrence. In 12 children, we performed a VATS procedure with a stapler wedge resection of the apical part of the lung and mechanical pleurodesis. In 1 patient, we had pneumothorax on both sides, but not at the same time. Those patients had, first, pneumothorax on the one side and, for a couple of months, on the other side.
In summary, we performed 12 VATS procedure in the last 7 years. In 1 patient, there was a bilateral pneumothorax and 2 VATS procedures were done. We had only 1 recurrence after VATS, and open thoracotomy was indicated. We found, on the apical part, small blebs and we did a wedge resection with mechanical pleurodesis.12,13
In children with giants bullas, we indicated open thoracotomy with resection of bullas.
We had 2 children with pneumothorax with a strong air leak. After a CT scan investigation, we found a lung bulla in both patients. One 17-year-old boy had a bulla of 9 cm diameter (Figs. 3 and 4) and a 12-year-old girl had a bulla of 5 cm diameter (Fig. 5). In these children, we did not perform VATS because we thought that bullas were too large for endostapler wedge resection and positions were not on the apical part of the lung (Table 1). 14
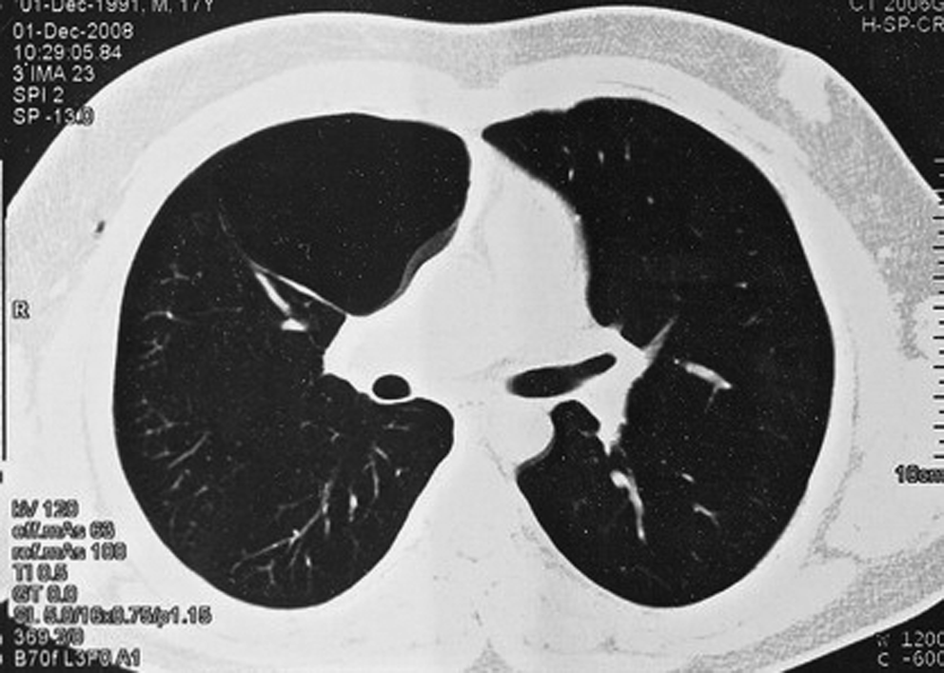
Giant bulla: computed tomography scan.

Giant bulla.

Bulla on the left side: computed tomography.
PSP, primary spontaneous pneumothorax; CT, computed tomography; VATS, video-assisted thoracoscopic surgery.
The duration of the VATS procedure was from 65 to 105 minutes (median, 85). The mean duration of the chest drainage was 5 days. Length of hospital stays was 6 days (range 5–8). All our patients received antimicrobial chemoprophylaxis with a single dose of ceftriaxone. In all patients, we prescribed postoperative patient-controlled analgesia. The duration of the open thoracotomy was 118 minutes (range, 93–138). The pain in patients with VATS was 2 days and in patients with open thoracotomy pain was 5 days. In all patients, we prefer apical bullectomy with linear stapler and mechanical pleurodesis because these operations were safer, simple, and fast. Cosmetics benefits of VATS procedures were also very important because wounds healed with minimal scars. Scars after open thoracotomy were long and ugly. The follow-up period was from 4 months to 5 years (mean, 3.4 years).
Discussion
Spontaneous peumothorax is a disease defined as the accumulation of air in the pleural space. Spontaneous pneumothorax occurs as a disruption of visceral pleura, with an escape of air into the pleural space with secondary lung collapse.15–17
Pneumothorax is divided into “small,” “moderate,” or “complete,” depending on the presence of a visible rim between the lung and chest wall. In the guidance for treatment of spontaneous pneumothorax, spontaneous pneumotho-racies were classified into three groups (18):
“Small”—small rim of the air around the lung <2 cm, chest tube not necessary “Moderate”—lung collapsed halfway toward the heart border “Complete”—airless lung, separate from the diaphragm
Children with small pneumothorax and without clinical signs, such as breathlessness, require only an observation without a chest tube or any other kind of treatment. Moderate, complete spontaneous pneumothorax always requires chest-tube drainage with suction and observation. 19 The size of the chest tube depends on patient age. We had 3 patients less than 14 years, and we inserted a small chest drain (No. 14). In patients 14 years and older, chest tubes were larger (No. 20). In all patients, low-pressure suction was done and pressures were between −10 and −20 cm H2O. Spontaneous pneumothorax is a very serious disease, and hospitalization is recommended in all cases.
In 1990, the first VATS procedure was reported by Levi et al. 20 Since then, this technique has spread rapidly around the world and has taken over the role of open thoracotomy. Our treatment algorithm is as follows: conservative treatment, such as chest tube suction, for at least 5 days. At the first episode in patients with bullas in CT scan, VATS was recommended, and also in patients with recurrence or with prolonged air leakage. In patients with giant bulla, open thoracotomy was recommended.
In our hospital, we did not have any patients with small peumothorax, and in all patients, chest-tube drainage was necessary. Chest-tube suction was recommended in our hospital for at least 5 days. After 5 days, in 2 patients, air leaks disappeared and chest tubes were removed. When an air leak was persistent, VATS procedure with mechanical pleurodesis was indicated. We had only 1 recurrence after a VATS procedure. VATS is a procedure with many more advantages than open thoracotomy. The pain in patients with VATS was less expressive than in patients with open thoracotomy. In addition, in patients with VATS, wounds healed with minimal scars.
Conclusions
VATS is a method with low morbidity, low invasiveness and cosmetic issues, and good results. VATS allows an effective, safe performance of standard surgical procedures, avoiding thoracotomy incision.
Footnotes
Disclosure Statement
No competing financial interests exist.