
Abstract
Abstract
Purpose:
Laparoscopic inversion herniotomy (LIH) is a method of inguinal hernia repair for female patients. In this article, we report our technique and outcomes for this procedure. We propose that LIH is a valid alternative to conventional open herniorraphy.
Methods:
Following institutional review board approval, we reviewed the charts of patients who underwent LIH or open inguinal hernia repair (OIH) from 2004 to 2007. LIH was performed with three instrument sites and no groin incision. The diagnosis, operative time, and complications were reviewed. Follow-up ranged from 5 months to 4 years.
Results:
We performed 79 LIH repairs (15 bilateral, 23 left, and 26 right) in 63 female children. We also performed 76 contemporaneous OIH repairs in girls. The age range was 1 month to 18 years (median, 3.8 years). Operative times for both the unilateral and bilateral LIH repairs were significantly shorter than those for OIH (P = 0.001). There were 2 recurrences after laparoscopic inguinal hernia repair, both within 5 months following repair early in our experience, compared to no hernia recurrences with OIH. The first recurrence was repaired conventionally via an open technique. The second case was repaired laparoscopically.
Conclusions:
LIH is an effective method for the repair of pediatric indirect inguinal hernia in female patients. The procedure allows the evaluation of the asymptomatic contralateral side without the necessity of a second long inguinal incision.
Introduction
The use of minimally invasive surgery (MIS) has increased in the field of pediatric surgery. A number of variations of laparoscopic inguinal hernia (LIH) in the pediatric population have been reported in the literature.2–6 El-Gohary first described the method of laparoscopic inversion herniotomy in 1997, 7 wherein the hernia sac was grasped at its distal end, inverted into the abdominal cavity, ligated, and subsequently resected. The largest published series with this technique included 37 patients. 2 Minimal access was achieved by using only an umbilical trocar, with instruments being inserted through 3-mm stab incisions placed laterally on the abdominal wall without a port. In this article, we report the largest published single-institution experience with this laparoscopic technique of inguinal hernia repair in female patients. We propose that laparoscopic inversion herniotomy is a safe alternative to conventional open herniorraphy.
Methods
Patients
Over a period of nearly 4 years, from January 1, 2004 to November 31, 2007, two attending surgeons at our institution performed the technique of LIH on female patients diagnosed with inguinal hernia. Patients were admitted on the morning of surgery and discharged in the afternoon of the same day. Patients with other significant diagnoses or a postconceptual age of less than 50 weeks were kept in the hospital overnight (or as long as their other conditions required) (n = 2). The follow-up time ranged from 5 months to over 4 years.
Operative technique
The procedures were performed under general anesthesia. The anesthesia team also used caudal blocks, if the parents consented. If no caudal block was placed, patients received an infiltration of local anesthetic at instrument or port sites prior to skin closure. The patients were placed in the supine position on the operating room table, with the abdomen and groin sterilely prepped. We gained access into the abdomen via a 2–3-mm infraumbilical incision; by using a Versess needle, the pneumoperitoneum was established with carbon dioxide (8–10 mm Hg). We used a 3-mm port and a 2.7-mm diameter, 30-degree scope to visualize the abdominal cavity. We always visualized and treated the symptomatic inguinal area first, followed by the contralateral side, as necessary (Fig. 1). Working instruments were introduced through two 1–2-mm lower abdominal stab incisions without the use of ports. A 2.7-mm grasping dissector was passed through the incision ipsilaterally to the side of the inguinal hernia, and a 2.7-mm Endoloop® (Ethicon Inc., Somerville, NJ) was passed through the contralateral incision. The tip of the dissector was then passed through the Endoloop into the canal of Nuck, where the distal hernia sac was grasped and inverted into the abdominal cavity by gentle traction (Fig. 2). High ligation of the hernia sac was completed by cinching down the Endoloop. In our early experience, the ligated hernia sac was left in situ. However, we revised our technique to include sac resection after experiencing 2 hernia recurrences (Fig. 3).
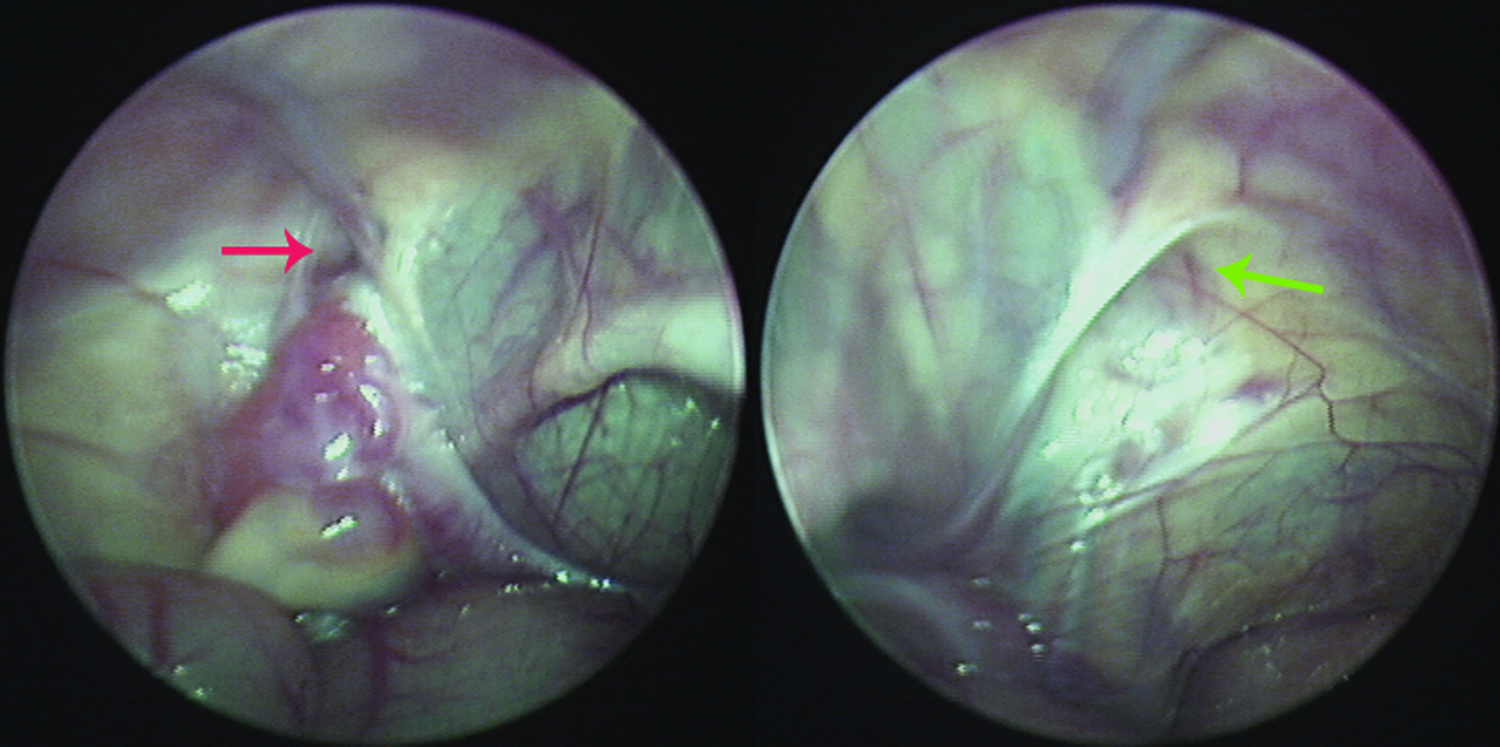
Visualization of inguinal hernia; laparoscopic view. The deep inguinal ring, lateral to the lateral umbilical fold, is seen. The red arrow denotes an inguinal hernia, with adnexal structures entering the canal. The green arrow is placed at the closed deep inguinal ring, on the contralateral side.
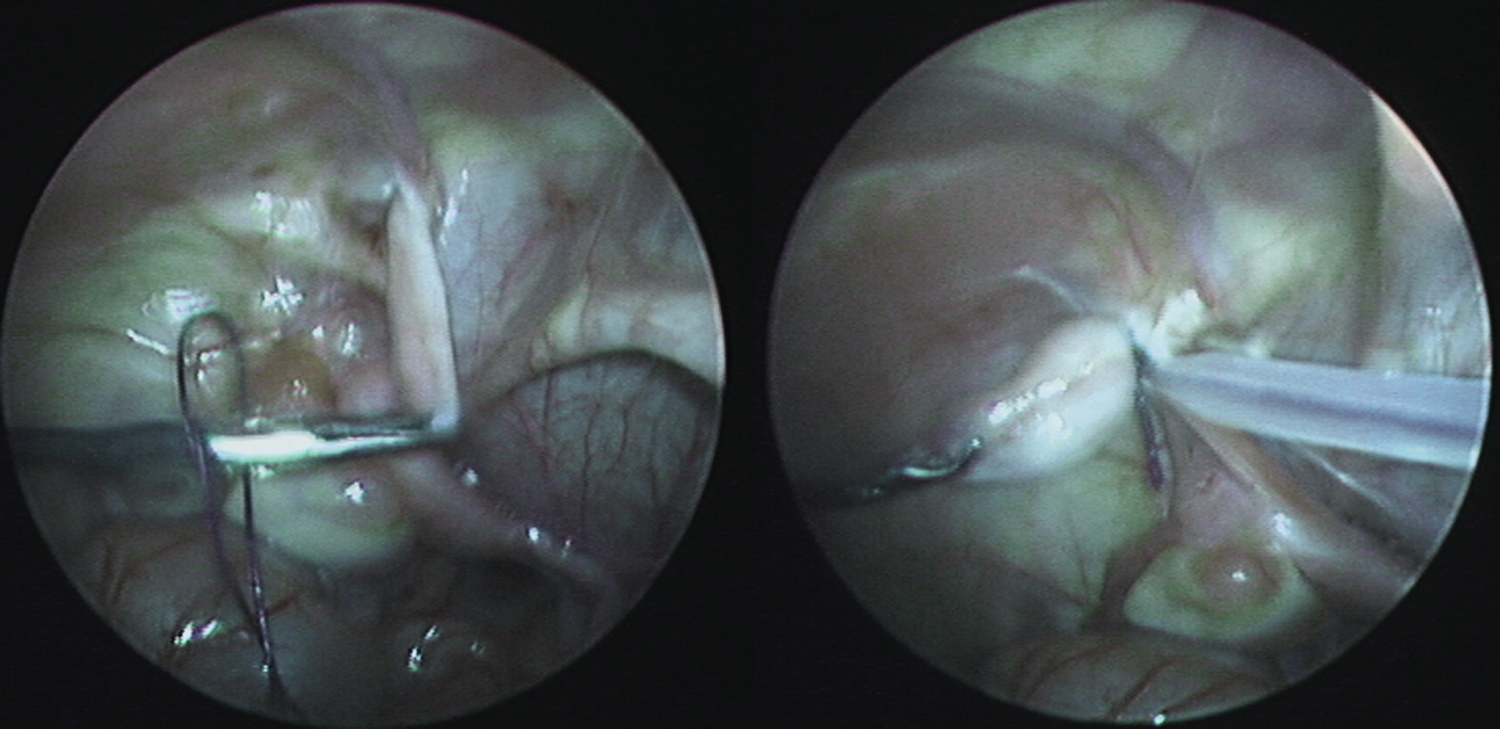
Endoloop placement. The dissector is passed through the endoloop, and the distal aspect of the hernia sac is grasped and brought through the suture. The endoloop is then secured at the base of the inverted hernia sac, effecting high ligation.

Excision of hernia sac. Once the endoloop is in place, the suture is cut. A dissector through the ipsilateral operative site holds the distal aspect of the inverted hernia sac, and the sac is excised.
If bilateral hernias were present, the contralateral hernia was also repaired by using the same ports. Upon completion of the operation, all instruments were removed under direct vision. The umbilical port was removed, and the fascia and skin were closed with single Vicryl stitches. Stab incisions were closed and dressed with Steristrips™ (3M; St. Paul, MN).
Results
A total of 79 LIH repairs were performed in 63 patients. Ages ranged from 1 month to 18 years (median, 3.8). The same two attending surgeons individually performed all the procedures, with assistance from a pediatric surgery fellow or resident. None of the cases were complicated by an incarceration or bowel obstruction. Unilateral hernia repair was performed in 48 patients, and bilateral hernia repair was performed in 15 patients. Of the unilateral repairs, 26 were on the right side, 22 on the left. Of the bilateral hernia repairs, 6 had bilateral hernias diagnosed preoperatively. The other 9 patients had contralateral hernias diagnosed intraoperatively. Of these, 5 patients had a preoperative diagnosis of a left-sided hernia, and the other 4 had right-sided hernias.
Mean operative time was 17.3 ± 6.1 minutes for unilateral repair and 25.7 ± 12.8 for bilateral repair when using the laparoscopic inversion herniotomy technique. We compared these times to the open repairs performed on female children by the same two pediatric surgeons. The mean operative times of 25.4 ± 9.1 minutes for unilateral (n = 193) and 37.1 ± 12.4 for bilateral (n = 76) for these open cases. Statistical analysis, using a Student's t-test, showed a significant difference between laparoscopic and open repairs (P = 0.001 for unilateral, P = 0.032 for bilateral).
In the early period of this study, there were 2 recurrences. Both of these occurred in patients who did not have the hernia sac resected. The first patient was diagnosed with recurrence 3 months following the initial procedure, and the second patient's recurrence was noted 5 months following the procedure. The first was repaired through an open approach, and the second was repaired with repeat laparoscopic inversion herniotomy, with resection of the hernia sac. Following the second recurrence, all hernia sacs were resected.
In 2 patients, sliding hernias, in which the ovary and fallopian tube comprised portions of the hernia sac, were noted. In the first patient, attempts were made to establish a sac that could be ligated, but this was felt not to be a satisfactory repair. Laparoscopic inversion herniotomy was aborted, and open hernia repair was performed by high ligation and closure of the internal ring. In the second patient, in which a sliding hernia was noted, no effort was made to repair the hernia laparoscopically, and an open repair was performed. There were no postoperative wound infections or delay in tolerance of oral feedings. Patients did not have a significant amount of postoperative pain or discomfort requiring medication or hospitalization. The cosmetic appearance of the wounds was excellent, with most being nearly unidentifiable.
Discussion
The role of laparoscopy in pediatric inguinal hernia repair is evolving and increasing in frequency. 8 There has been much discussion among pediatric surgeons regarding the utility of the laparoscopic repair of inguinal hernias. The open technique remains the standard of care, and some have argued that the added risks associated with a violated peritoneal cavity from laparoscopic intra-abdominal repair are unjustified. Further, there is debate as to whether the laparoscopic technique is an appropriate anatomic repair.
In open repair, high ligation and resection of the hernia sac is the standard. One laparoscopic technique of inguinal hernia repair in boys, recently described by Chan and Tam, involves the laparascopically assisted purse-string closure of the internal ring, excluding the spermatic cord structures, is performed with the hernia sac left intact. 3 Their method involves the extraperitoneal injection of saline to lift the peritoneum off the underlying vas deferens and testicular vessels. A purse-string suture is then placed circumferentially at the internal inguinal ring to close the defect. While this is not the high ligation that is performed in an open technique, it is similar, in that the internal inguinal ring is closed, which would preclude the viscera from herniating into the intact sac. The vas and vessels are protected, in that they are not manipulated or dissected free from the sac, which is left in situ.
Yip et al. recently described their method for laparoscopic inguinal hernia (LIH) repair, called the flip-flap hernioplasty. 4 In this method, the hernia is identified, and an incision on the peritoneum is made, anterolaterally to the defect. A peritoneal flap large enough to cover the defect is then lifted, and the anterolateral half of the sac is dissected free of underlying tissue. This causes the sac to collapse, and also keeps the spermatic vessels and vas deferens safe, as they are at the medial aspect of the sac. The flap is then flipped medially (over the now collapsed defect) and anchored with a stitch. The theoretic benefit of this closure is that increased intra-abdominal pressure will actually act to decompress the hernia sac. Although the benefits of laparoscopy in the treatment of inguinal hernia are marginal, the laparoscopic approach has an obvious advantage: the ability to visualize the hernia clearly. In addition, the use of laparoscopy allows one to examine the contralateral side with similar ease, as commonly done by placing a laparoscope during open repair through the hernia sac. The theoretic advantage of an umbilical laparoscope placement would be the ability to visualize the opposite side in the presence of a thin sac, where during open repair one risk causing a tear in the sac.
The method of inversion herniotomy, as used in this series, also allows safe dissection of adherent viscera. Using the endoloop as a leash on the sac, an adherent round ligament or ovary can be dissected off without excessive manipulation with a dissector. 2 One must, however, be prepared to convert to open repair if the viscera cannot be safely dissected. Further, laparoscopic inversion herniotomy is feasible only in female patients, because it does not allow for protection of the vas deferens or testicular vessels. In regards to the benefits of sac resection, it is possible that a hernia sac left in situ may reherniate through the inguinal canal, if the ligating suture becomes loosened. Thus, we postulate that resection of the sac may eliminate this possibility. Evidence suggests that transection of the sac without ligation is an efficacious treatment for inguinal hernia, as it is not associated with increased incidence of recurrence or other complications. 5
In our series, the cases involving large hernias with a higher risk of ovary or other organ involvement were converted to open. We did not believe that these cases could be safely treated laparoscopically. While the visceral portion of the sliding hernia could be reduced laparoscopically, closure of the internal ring would require intracorporeal suturing. These steps may be more complicated and may add to the overall operative time. Subsequently, instrument changes, with the possibility of additional ports, would be required; so, we believe that conversion to an open inguinal technique would be the better approach. Any patient who was preoperatively diagnosed with a large inguinal hernia had an open repair. All emergent cases were performed with the open technique, as well.
In this nonrandomized series, the primary outcome measure was hernia recurrence. As we have had 2 recurrences with LIH, compared to none with the open approach, most surgeons may disregard the utility of the laparoscopic method. Nevertheless, with increasing experience in the use of LIH, we are not experiencing additional recurrences. To further demonstrate feasibility, an additional outcome we studied was procedural times, where we observed a statistically significant decrease in operative times for both the unilateral and bilateral LIH repairs, when compared to open procedures performed during the same period. We would like to note that the operations are extremely homogenous, with a narrow standard deviation in operating room times, making the differences observed reproducible and with small P-values. Although it is arguable whether an 8-minute difference is of questionable clinical relevance, shorter operating room times could theoretically equate to an increase in the number of cases performed per day. The ability to perform additional cases could then offset any increased costs of laparoscopy, such as the initial investment in the equipment, as well as its maintenance. 9 On the other hand, the changes in operative times may be surgeon dependent and might not alter costs or the number of cases performed. It is also possible that the observed differences in operating times may be secondary to the same surgeons repairing larger hernias with the open method.
Conclusions
Laparoscopic inversion herniotomy is a safe, feasible technique for repair of indirect inguinal hernia in female children. The procedure is easily learned and allows for the complete evaluation of the contralateral side. The incisions are small, and the findings can be easily documented with pictures. We have found that using an endoloop suture as a method of high ligation of the sac is very effective. Early experience of this procedure is very promising and should be validated in a larger, prospective, randomized trial.
Footnotes
Disclosure Statement
No competing financial interests exist.