
Abstract
Abstract
Background:
Laparoscopic sleeve gastrectomy has been gaining popularity due to its simplicity and outstanding results. This procedure is no exception to attempts aimed at minimizing abdominal port access. In this article, the senior author (AAS) presents his technique for an entirely transumbilical single-incision approach where no extraumbilical incisions are necessary.
Materials and Methods:
Seven patients underwent laparoscopic sleeve gastrectomies using this single-incision, totally transumbilical technique. The same surgeon (AAS) performed all surgical interventions. The same perioperative protocol and operative techniques were implemented for all the patients.
Results:
A total of 7 single-incision transumbilical laparoscopic sleeve gastrectomies were successfully performed using this technique. Two patients required lysis of adhesions, and 1 patient underwent an umbilical hernia repair during the procedure. Mean operating time was 143 minutes. One of the patients required the insertion of an additional trocar. There were no mortalities or postoperative complications noted during the mean follow-up period of 1.5 months.
Conclusions:
Single-incision laparoscopic sleeve gastrectomy performed entirely through the umbilicus is safe, technically feasible, and reproducible.
Introduction
Materials and Methods
A total of 7 single-incision transumbilical laparoscopic sleeve gastrectomies were performed by the same surgeon (AAS). The patients selected for this approach had preoperative body-mass indices (BMIs) between 35 and 55 kg/m2 with peripheral obesity, as the umbilicus is usually receded further from the gastroesophageal junction beyond the reach of the instruments in patients of higher BMIs and those with central obesity. The patients included 5 females and 2 males, with a mean age of 46.1 years (range, 23–57), a mean preoperative weight of 324.6 lbs (range, 280.2–364.3), and a mean preoperative BMI of 49.3 kg/m2 (range, 43–54.8). The patients' existing comorbidities included diabetes (57.1%), hypertension (42.9%), sleep apnea (71.4%), hyperlipidemia (71.4%), arthritis (85.7%), back pain (71.4%), and gastroesophageal reflux disease (85.7%).
Technical procedure
The patient is placed in the supine position. The surgeon stands on the right side of the patient with the assistant on the left side. A 2.5-cm intraumbilical skin incision is created and is deepened to the linea alba, where a 1-cm fascial incision is made; the peritoneum is incised and the 15-mm blunt trocar is deployed. It should be noted that the fascial incision must be smaller than the blunt trocar size to create an effective seal, preventing gas leakage. Pneumoperitoneum is achieved to a pressure of 15 mm Hg. A 5-mm flexible-tip laparoscope (Olympus, Center Valley, PA) is inserted. Two 5-mm low-profile trocars (Covidien, Norwalk, CT) are inserted. All three trocars (two 5-mm trocars and one 15-mm trocar) are inserted through the same umbilical skin incision but with different fascial incisions at different levels in a triangular fashion (Fig. 1). This minimizes clinching between the trocars, instruments and the scope. It also provides a more spacious range of movement for the single-incision approach.

The intraumbilical transfascial placement of trocars in a triangular fashion.
Using a 5-mm LigaSure (Covidien) and a 5-mm flexible grasper (Covidien), the greater curvature of the stomach is mobilized, starting from a point 6 cm proximal to the pylorus (Fig. 2A), staying close to the wall of the stomach all the way up the greater curvature to the angle of His, dividing both gastrocolic and -splenic ligaments. The mobilized portion of the stomach is used to retract the liver to provide further exposure of the angle of His (Fig. 2B–2D). It is important to identify and mobilize the angle of His with exposure of the left crus of the diaphragm to facilitate the complete resection of the fundus. Retrogastric adhesions are taken down with the LigaSure to allow complete mobilization of the stomach, eliminate any redundant posterior wall of the sleeve, and to exclude the fundus from the gastric sleeve. Once the stomach has been completely mobilized, a 34-Fr orogastric tube is inserted orally into the pylorus and placed against the lesser curvature. This will calibrate the size of the gastric sleeve, prevent constriction at the gastroesophageal junction, and provide a uniform shape to the entire stomach.
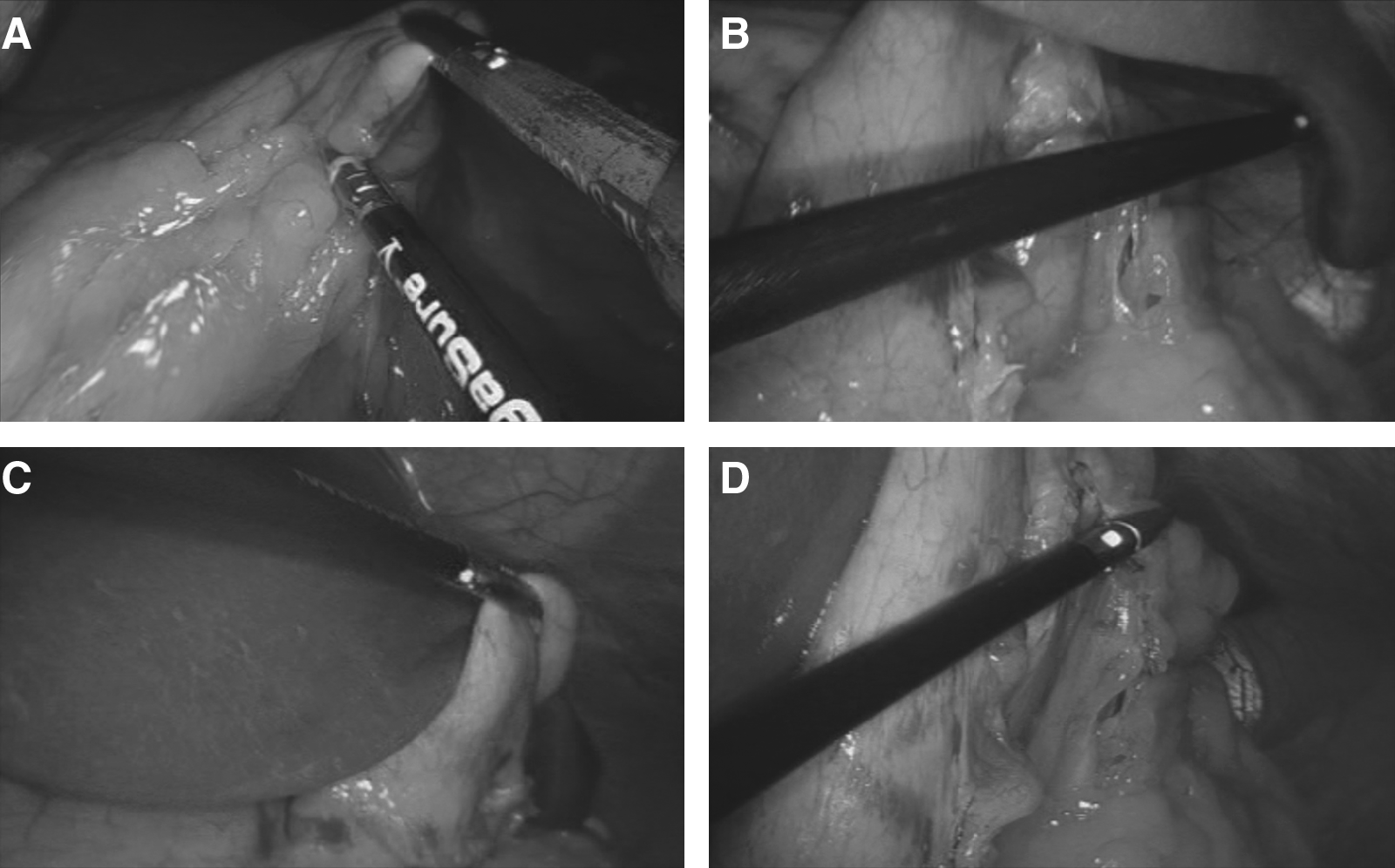
Intraoperative laparoscopic imagery. (
Gastric transection is started at a point 6 cm proximal to the pylorus, leaving the antrum and preserving gastric emptying. A long laparoscopic reticulating 60-mm XL Endo-GIA stapler with a green cartridge 4.8 mm (Covidien) and bioabsorbable glycolide copolymer buttressing material reinforcements (Seamguard; W.L. Gore & Associates, Flagstaff, AZ) is inserted through the 15-mm trocar in a cephalad direction and used for the entire transection. In the last case, we switched to a synthetic absorbable buttressing material (Duet; Covidien). The stapler is fired consecutively along the length of the orogastric tube until the angle of His is reached. Care must be taken not to narrow the stomach at the incisura angularis. It is important to inspect the stomach anteriorly and posteriorly to ensure no redundant posterior stomach. Approximately 80% of the stomach is separated. The entire staple line is inspected for bleeding and tested for leakage. Bleeding may indicate an unstable staple line and necessitates the prompt placement of clips along the line of bleeding. Then, after clamping the distal end of the sleeve, the staple line is submerged under infused saline, and air under pressure is insufflated into the stomach to test for leakage. This is repeated by infusing methylene blue into the sleeve. Air bubbles or bluish discoloration of the infused saline would indicate leakage of an unstable staple line.
The resected stomach is placed in a 15-mm specimen endobag (Covidien) and extracted through the umbilical incision without extension of the umbilical skin incision. The fascial defect of the 15-mm trocar site is closed with a figure of eight 2/0 nonabsorbable suture to prevent port-site hernias. An upper gastrointestinal contrast study is obtained on postoperative day 1 to rule out leaks and obstruction. Once the patient is able to maintain hydration and the pain is managed appropriately with oral analgesics, the patient is discharged.
Results
A total of 7 single-incision transumbilical laparoscopic sleeve gastrectomies were successfully performed with using this technique (Table 1). Two patients required lysis of adhesions procedures, and 1 patient underwent an umbilical hernia repair during the procedure. Mean operative time was 143 minutes (range, 96–176). Mean operative blood loss was 51.3 cm3. Our first patient required the insertion of an additional 5-mm trocar. The mean hospital stay was 2.1 days (range, 2–3). There were no mortalities or immediate postoperative complications. The mean postoperative BMI was 44.6 kg/m2 (range, 39.7–50.9) after a mean follow-up period of 1.5 months (range, 0.5–4) with patients losing a mean of 24.3% excess weight (range, 16.6–35.2) from their initial assessment. The majority of the patients' preoperative comorbidities had improved or resolved; this included 50% of diabetes, 66.7% of hypertension, 60% of sleep apnea, 40% of hyperlipidemia, 33.3% of arthritis, 60% of back pain, and 50% of gastroesophageal reflux comorbidities showing either improvement or complete resolution during their follow-up.
OR, operating room; BMI, body-mass index; LOA, lysis of adhesions; UHR, umbilical hernia repair.
Discussion
Sleeve gastrectomy has gained popularity as the first of a two-stage bariatric procedure and, recently, as a stand-alone procedure.2,3 This can be attributed to the many advantages of sleeve gastrectomy. Unlike a gastric bypass, a sleeve gastrectomy preserves the pyloric function, thus eliminating the risk of dumping. It does not induce malabsorption, making it feasible in patients with inflammatory bowel disease. 4 Unlike the adjustable gastric band, a sleeve gastrectomy does not require any adjustment.
Typically, a laparoscopic sleeve gastrectomy necessitates five to seven small skin incisions for the placement of trocars. 4 Recently, we developed a novel technique for a single-incision laparoscopic sleeve gastrectomy, where the entire procedure is performed through a 2.5-cm umbilical incision, in addition to a 5-mm subxiphoid incision for the placement of a liver retractor. 1 However, we have found that in a select group of obese patients, the procedure can be performed entirely through the umbilicus without the need for any extraumbilical incisions. Originally, sleeve gastrectomies have been recommended for high-risk patients with high BMIs. However, due to the simplicity and effectiveness of the procedure, we and others have expanded its indications to include most morbidly obese patients, including those with lower BMIs. 5 In this group of patients, the procedure can be done entirely transumbilically without the need for any extraumbilical incisions or a liver retractor. This can be attributed to many favorable conditions met in this group of patients. Primarily, the gastroesophageal junction can be easily reached by using transumbilical instruments. Second, the liver is relatively small and can be retracted by using the mobilized stomach. Finally, working from behind, rather than in front of, the stomach achieves excellent exposure during this procedure.
This approach, however, should be tailored according to the patient's body habitus and liver size. In a superobese patient with a low-lying umbilicus, Katkhouda et al. 6 recommend the advancement of trocar placement toward the subxiphoid, as the distance between the subxiphoid process and the umbilicus is likely to be more than 25 cm. The potential advantages of this approach are subsequent to limiting the abdominal incisions to only one site, in addition to the other advantages of MIS. Using the single-access approach, we are able to combine all of the standard laparoscopic entry points into one port of entry (i.e., the umbilicus), thus decreasing the number of incisions required for a laparoscopic sleeve gastrectomy from six to seven incisions to only one virtually invisible intraumbilical incision (Fig. 3). The substantial reduction in abdominal wall trauma could potentially translate into minimal discomfort and less postoperative pain, leading to a faster recovery. Avoiding the lateral placement of ports eliminates the risk of epigastric vessel injury, as well. 7

Postoperative picture of a patient 1 month after a single-incision transumbilical laparoscopic sleeve gastrectomy.
A morbidly obese patient usually has a thick abdominal wall that can limit the maneuverability of the trocars. The “torque effect” on trocars increases with the increasing thickness of the point of abdominal access, counteracting the movement of trocars, and decreasing maneuverability through an extraumbilical incision. Utilizing the thinnest part of abdominal wall (i.e., the umbilicus) could minimize the torque effect on trocars inserted at such close proximity, providing a wider range of motion for the instruments and trocars in different directions. 8 The umbilical incision was ultimately used for the extraction of the gastric specimen. If necessary, the surgeon can add an extraumbilical trocar to handle any intraoperative challenge that may arise.
The applicability of this technique requires confident multiport laparoscopic skills to shorten the learning curve of this approach and overcome the technical challenges associated with navigating instruments within a limited range of motion, handling flexible instruments, and a flexible-tip scope to improve maneuverability.
Coordination between the surgeon and the camera person, as well as switching the 5-mm instrument between the laparoscopic ports are essential to optimize the instruments' range of motion for better ergonomics and to avoid clashing of the instruments and the laparoscope during the procedure. Overall, intra- and postoperative results obtained from using this technique were comparable to previously reported conventional laparoscopic series describing this procedure.9–11
Conclusions
In conclusion, single-incision transumbilical laparoscopic sleeve gastrectomy is safe, technically feasible, and reproducible in a selected group of morbidly obese patients. Prospective, randomized studies, comparing single access versus conventional multiport laparoscopic sleeve gastrectomies in large volumes and a long-term follow-up, are needed to confirm our initial experience.
Footnotes
Disclosure Statement
No competing financial interests exist.