
Abstract
Abstract
Laparoscopy is often carried out with personnel unfamiliar with the equipment and layout, thereby forcing the surgical team to adapt by twisting and stretching awkwardly. This can make laparoscopy more difficult and frustrating for the surgeon, potentially increasing patient risk. We carried out a short survey of laparoscopic procedures to determine when surgeons experience discomfort, and whether or not operative checklists could reduce these.
Materials and Methods:
All patients undergoing laparoscopic operations by one surgeon between November 2006 and May 2007 were studied. Patients and surgeons had various physical measurements recorded, including the placement and orientation of equipment, staff and patients, any problems arising, and the discomfort of the surgical team. Scaled diagrams were drawn, outlining positions and orientation, allowing the measurement of the degree to which the surgeons twisted and stretched. Peroperative surgeon comfort levels were recorded. The ideal table height for surgery was calculated, suggestions to improve the surgeon's comfort were identified, recommendations on theater layout were produced, and sample checklists of common problems with ways of avoiding them were established.
Results:
Of 31 procedures, 10 had full data recorded for analysis. Physically demanding positions were common. There was no correlation between surgeon position and comfort for short operations (<60 minutes). Data for operative time >60 minutes was incomplete, but a definite trend to increasing discomfort with time was evident. In 10 operations, 85 problems occurred, 57 relating to theater layout. A third were avoidable repeat problems.
Conclusions:
Simple measurements of surgeons, patients, and equipment improves staff and equipment positioning. A log of problems and discomforts in the theater ensures that preventable factors are not repeated, reducing the frustrations of laparoscopy. By planning equipment positioning and testing it, a preferred theater set-up layout can be retained for future use. Checklists would help in the smooth execution of a laparoscopic procedure.
Introduction
Materials and Methods
Data were prospectively collected from all the pediatric patients undergoing laparoscopic operations by one surgeon between November 2006 and May 2007. A number of measurements of the patient and surgeon were obtained to calculate the ideal table height for each surgeon.
Patient measurement
The patient's position on the operating table was noted from using scaled diagrams after taking a number of measurements, including the distance from the crown of the head to the top (i.e., anesthetics end) of the table, the distance to the umbilicus from the crown marking the center of the abdomen (commonly, the central port site), the distance from the umbilicus to the xiphisternum superiorly, the pubic bone inferiorly and the edge of the abdomen laterally (measured to the right side of the umbilicus), the distance from the right side of the abdomen to the table edge, and the distance from the umbilicus to the feet, to have the patient's complete height.
Surgeon's position
To record how far up or down the length of the table the operating surgeon (OS) and assisting surgeon (AS) would be standing, the midline relative to the patient's umbilicus was measured and rated as +ve, if they were further up the table toward the head, and −ve, if they were standing toward the feet. Since our surgeons usually stood as close to the table as possible, how far back they were from the table was not recorded. Port-site position was noted at the end of the operation by marking them on a rough abdominal diagram and measuring the distances between each of the ports. We also recorded which surgeon was using which ports and, in the case of the OS, which hand was using which port.
Surgeon's measurement
The total height, elbow height, shoulder height, and eye height was recorded for each surgeon. The elbow-MCP (metacarpophalangeal) joint length was noted, allowing us to draw an arc from the position of the surgeon's elbow, showing their comfortably reach with their elbows by their sides. This was used, along with the value for shoulder width, in producing our scale diagrams. Foot length was also measured.
Surgeon's comfort and predicted discomfort
Surgeon comfort was recorded at 15-minute intervals, using a 10-point visual analog scale. Other factors thought to influence comfort, such as subjective feelings of well-being, alertness, and mood, were noted. Predicted discomfort was estimated from calculating degrees of stretch and rotation during surgery and comparing them to actual measurements/recording of feelings of discomfort during surgery.
Scaled maps of theater and equipment
The theater floor comprised a series of large tiles, which were measured and used as a scaled grid to draw out theater plans (Fig. 1). The scaled maps were used to suggest the modification of future layouts after keeping an operating log of all problems and difficulties encountered.
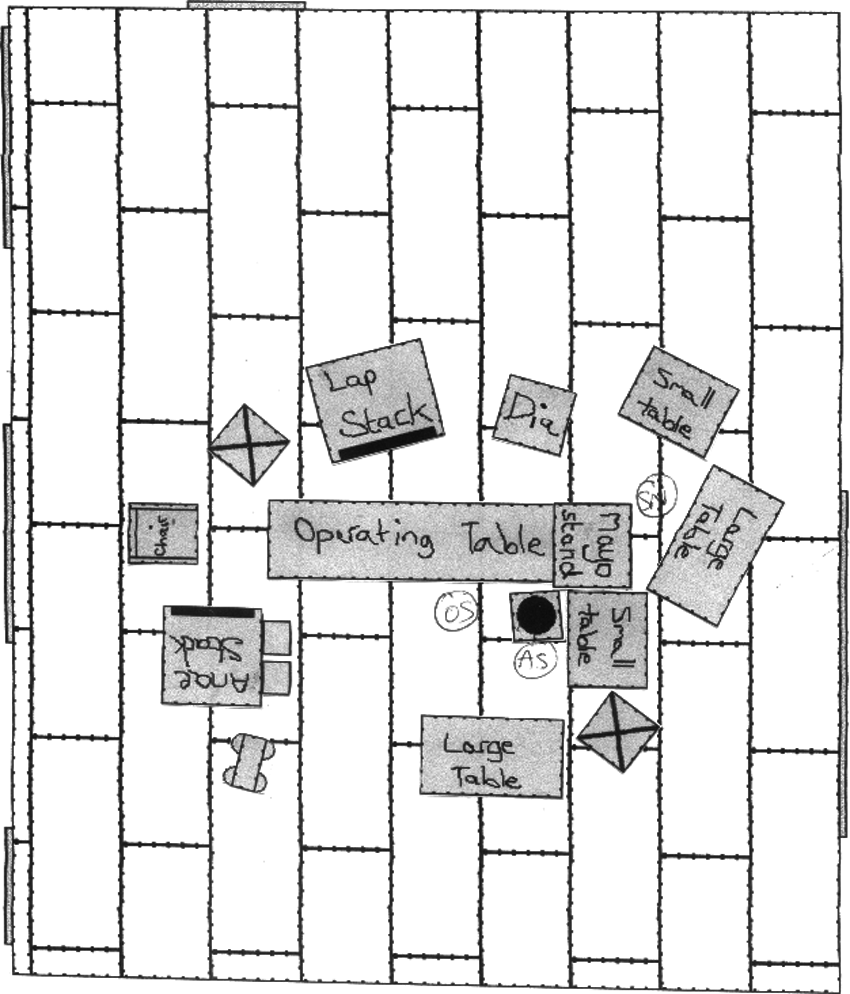
Example of scaled diagram of theater layout.
Results
Of 31 procedures, 10 operations were fully recorded for analysis (Table 1). Children <3 years had similar-sized abdomens (approximately 9 × 17 cm), while in children aged >10 years, these were 17 × 28 cm. One child 136 months in age was shorter and lighter than the other children in the older age group.
UDT, undescended testes.
Calculation of table height for each surgeon
The ideal table height for each surgeon was calculated from using the patient's abdominal depth : width ratio and the average instrument angle within the abdomen. Nine of the 10 children had their abdominal depth : width ratio measured (Table 2). In 1 child, this was not carried out as the operation was performed with the child on its side. This ratio mean was 0.58 (range, 0.53–0.69), despite patients varying between 1 and 15 years of age, and so, the angle of our instruments was assumed to remain the same from one patient to the next. An approximation of the average angle of the operating instruments was calculated by taking a patient of mean abdominal proportions of 12 × 21 cm at the umbilicus and placing port sites halfway between the midline and the edge of the abdomen (Fig. 2).
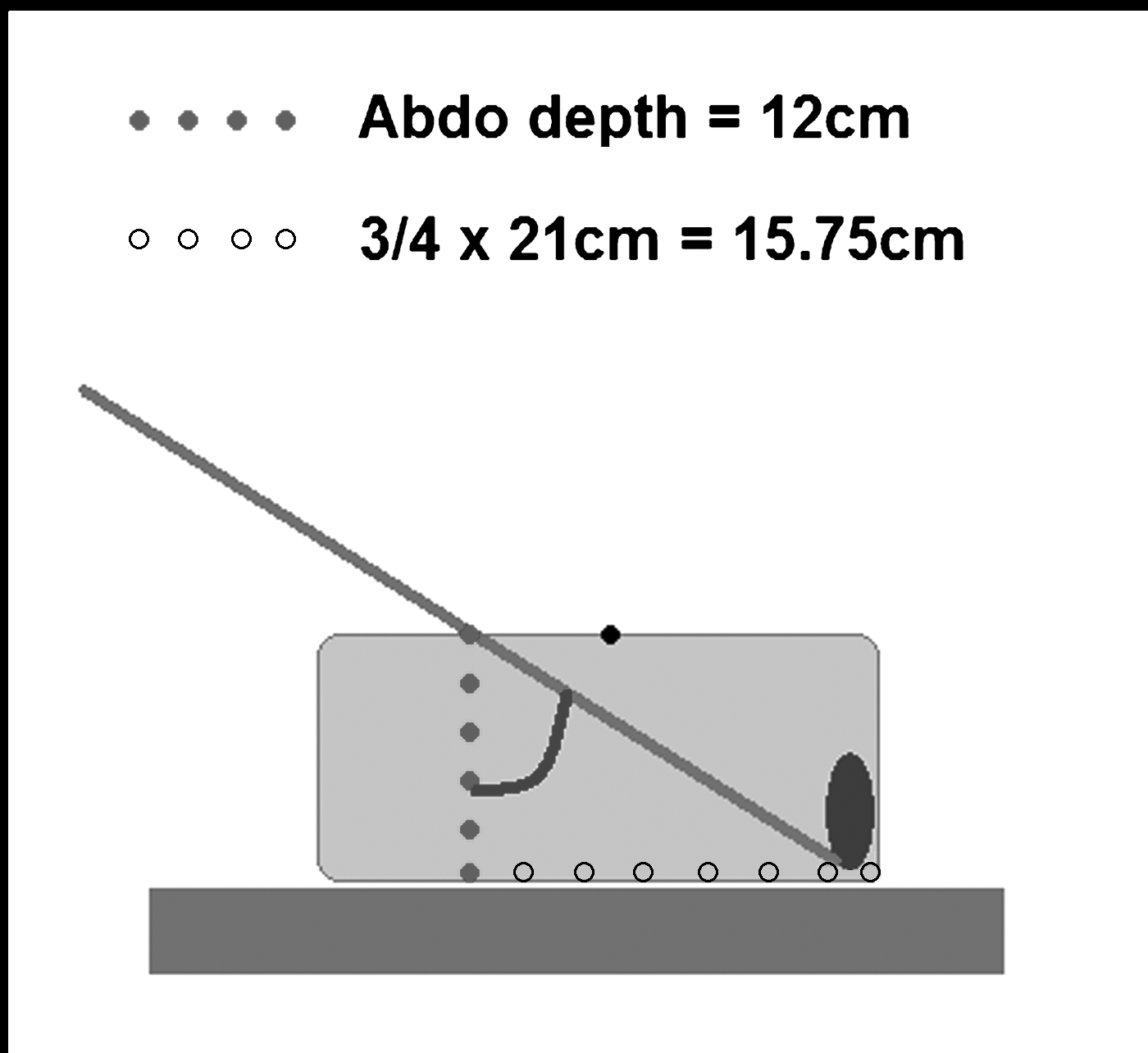
Diagram showing calculation of angle of instruments with the abdominal wall where tan (blue angle) = opposite side/adjacent side = 15.75/12 = 53 degrees to the nearest whole number.
All nonintegers rounded to two significant figures.
Instruments were, therefore, held at 53 degrees from the vertical (37 degrees from the horizontal). Because insufflation increases depth, and the organ is not always as lateral as the abdominal wall, we assumed the real angle was likely to be <53 degrees from the vertical or >37 degrees from the horizontal. Since the operating instruments are 35 cm long, and were likely to be held at around 53 degrees from the vertical, we calculated how much lower the table surface needed to be than the height of the surgeon's hands (Fig. 3). The table height was, therefore, calculated to, ideally, be around 21 cm lower than the elbow height of the operating surgeon.
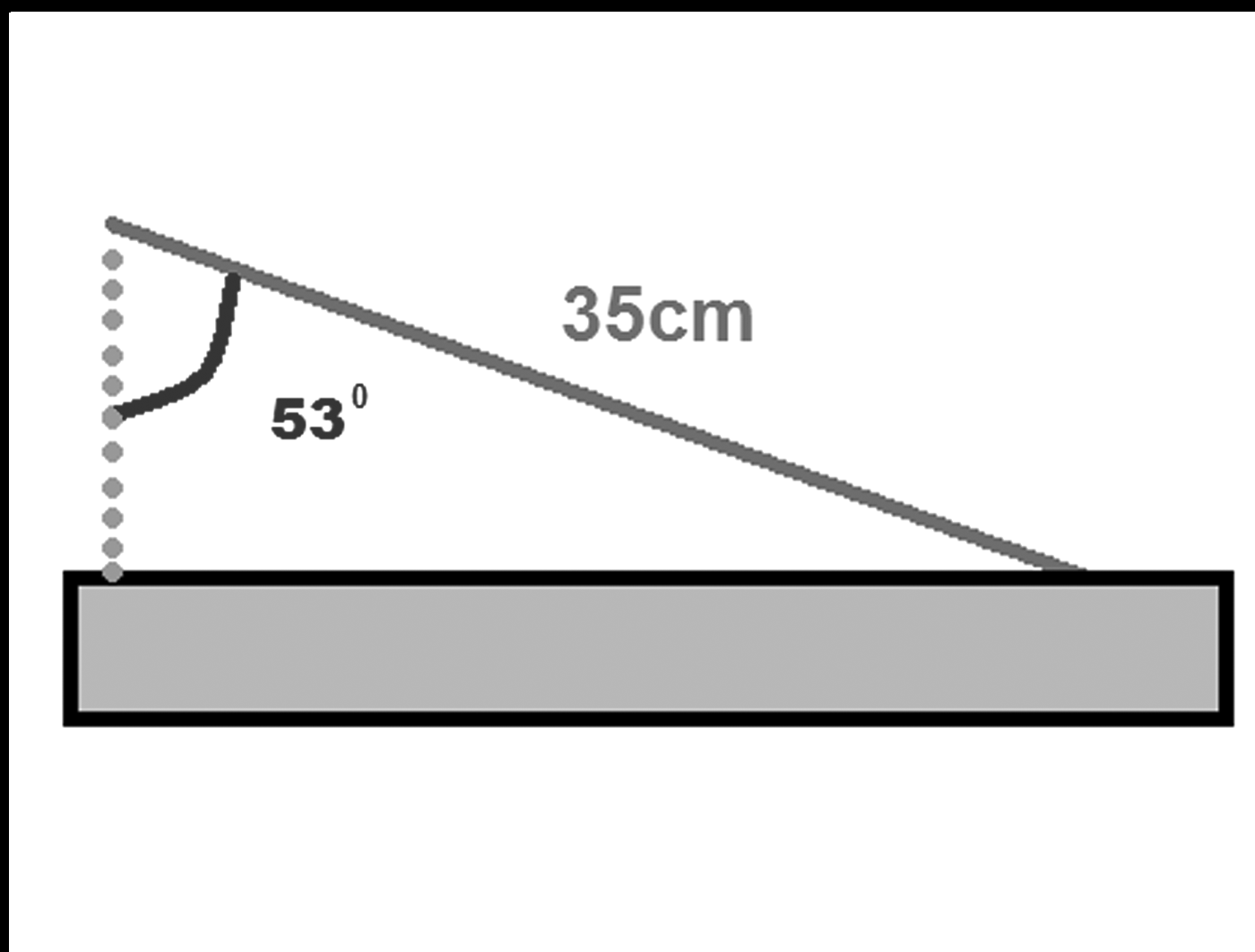
Diagram showing the calculation of table height below the surgeon's elbow where Cos (53) = adjacent side/35 and, therefore, adjacent side = 21 cm to the nearest whole number.
Calculation of surgeon's discomfort
Scale diagrams for each operation (Fig. 4) were produced from estimating surgeon stretch and rotation. The following measurements and circles of set diameters were used for this (Fig. 5):
Circle of diameter = surgeon shoulder width, allowing a line to be drawn from one side to the other, equating to the surgeon's shoulder width, no matter how it is rotated. Circle of radius = surgeon elbow to MCP, representing the range of movement of the surgeon's arm with their elbows by their side. Circle of diameter = 28 cm, representing the horizontal length of a 35-cm instrument held at 53 degrees from vertical. By drawing a line from one side of the circle to the other, we depicted an instrument that was 28 cm, no matter the rotation. Circle of diameter = 83 cm and another of diameter = 38 cm, allowing us to draw lines across them to scale the front end of the laparoscopic stack and its screen, respectively.
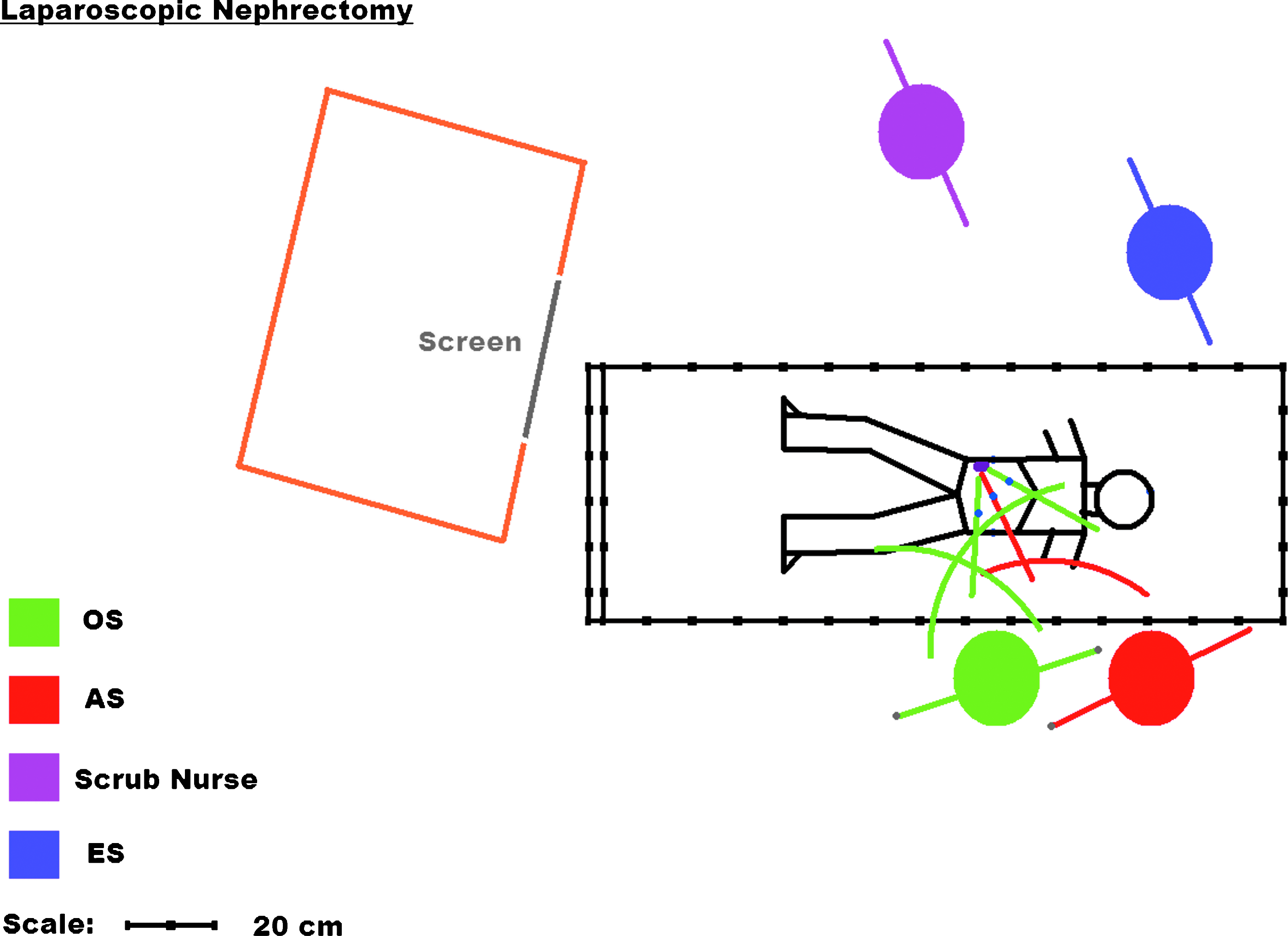
Diagram representing a typical scaled figure of an operation to allow an estimation of surgeon's discomfort. OS, primary surgeon; AS, assistant; ES, second assistant.
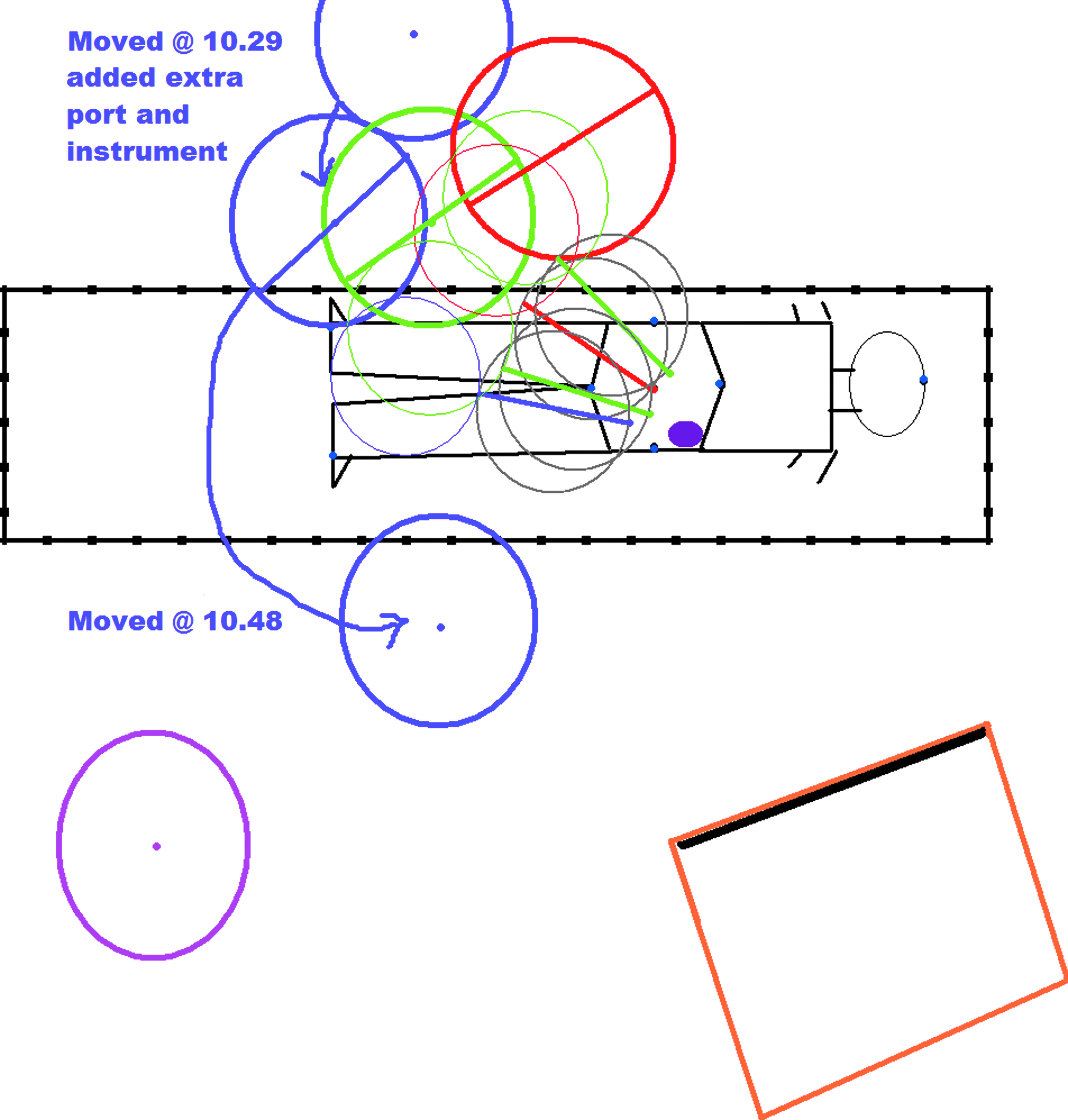
A work-in-progress diagram outlining scaled circles used and changes in position during surgery.
In addition, patient data were used to draw an outline of the patient placed in the exact location on the table. This allowed port sites to be marked on the diagram and the laparoscopic stack's position and rotation relative to the table to be noted. Surgeons' positions up or down the table from the patient's umbilicus was marked, and a line was drawn representing the correct length for their shoulder width, rotated toward the operating ports. Circles were added for heads. The operating instruments were drawn from the target organ through the ports toward the OS and the laparoscope through its port toward the AS. Arcs representing the surgeon's range of forearm movement were marked onto the diagram. These steps, followed for each operation, made it possible to estimate how far the surgeons were having to twist and stretch to reach the operating instruments and look at the screen.
Twisting was calculated by drawing a line from the surgeon to their port site, then drawing another line from the surgeon to the middle of the screen and measuring the angle between the two. Stretching was measured by taking the distance between their comfort arc and the end of the instruments. Stretch and rotation during nine procedures are shown in Table 3. Data for one procedure (nephrectomy) was incomplete and was not included.
Cases marked (a) and (b) were ones in which the position of the patient was changed during surgery.
FS, Fowler-Stephens; Lap UDT, laparoscopy for undescended testes.
Negative values occur where the ends of the instruments are within the arc of the surgeon's arms. Since the surgeon can easily step back to correct this, the negative values were scored as 0 cm. The OS for each operation was given two values: one for each hand. These were added together, as two outstretched arms are heavier than one.
Stretch
We defined a 0–9-cm stretch as small, a 10–19-cm stretch as medium, and a 20–30-cm stretch as large (30 cm being full-arm extension).
Rotation
We similarly defined rotation as small for a 0–29-degree twist, 30–59 degrees being medium and 60–90 degrees being large. There was a wide variety in positions adopted by the team (Table 3). Nine of the 24 positions had a surgeon stretching at least 12 cm to hold their instrument (15 cm being 50% of full-arm extension), and 8 of 24 recorded starting positions had a surgeon twisting more than 45 degrees from their midline
Comfort: Combined stretch and rotation
By assigning stretch and rotation values of 0 for small, 1 for medium, and 2 for large, we rated how uncomfortable we thought the surgeon would have been accounting for both factors. We assumed that stretch and rotation were summative (a reasonable assumption) and equal (which we could not prove, but it is likely they would have a similar impact). For each operation, the change in each surgeon's comfort was recorded every 15 minutes, given that there would be a certain value of comfort to account for how they were feeling at the start of a procedure. We recorded the change in comfort over the first 30 minutes for all our operations, and after 30 minutes, we included only those that lasted more than an hour. Table 4 shows our predicted values of comfort, where 0 is theoretically comfortable, 1 denotes slight discomfort, 2 and 3 describe being quite uncomfortable, and 4 suggests that the surgeon is at near full stretch and very twisted away from the midline. Tables 5 and 6 compare this to the actual comfort values recorded for each operation. There was no correlation between length of surgery and change in comfort up to 60 minutes in our small series. Data for longer operations were incomplete and could, unfortunately, not be analyzed fully, although there was certainly a trend to increasing discomfort with time in operations in using our measurements.
Where 0 = comfortable, 4 = maximum discomfort predicted.
Bil FS, biliary Fowler-Stephens; Lap UDT, laparoscopy for undescended testes.
Where 0 is comfortable and 4 is very uncomfortable.
Bil FS, biliary Fowler-Stephens; Lap UDT, laparoscopy for undescended testes.
Log of encountered problems
We found 85 recorded problems, 57 of which occurred relating to the equipment and layout of the theater (Table 7). Other problems related to preparation of the surgeon and assistant, preparation of the patient, and preparation of the trays and equipment. Of the 57 related to positioning of equipment, 9 appeared more than once. Six occurred twice and 3 occurred 3 times (i.e., 21 were repeats). Over a third of the problems could have been avoided by simply noting them down the first time they appeared and checking them off as addressed the next time. For the rest, we were able to find simple solutions to, or ways to minimize, their occurrence. These were things such as ensuring spare disposable scissors were available in case the set scissors were blunt or checking that the laparoscopic stack was near enough to the surgeons for the fiber-optic light lead to reach the telescope. We subsequently grouped these into tips for the scrub nurse (Table 8), surgeons (Table 9), and circulating theater staff (Table 10).
(r) denotes problems repeated.
Discussion
In adults, “discomfort in the shoulders, back, and neck is an established complaint among laparoscopic surgeons and is related to the unnatural postures adopted during laparoscopic interventions.” 2 These researchers showed that, on simulators, having armrests improved both the comfort of surgeons and the number of operative errors. Such items are not readily available for actual use in operating theaters, but it shows the potential benefits of good surgeon positioning on both comfort and technique. Stone and McCloy highlight the lack of rigorous ergonomic application in the medical community, especially in the design and testing of equipment. 3
Our study has shown that it is possible to calculate and set up the table height for standard pediatric laparoscopic surgery for each surgeon. Ideally, the surgeon's elbows should be resting at their sides, having the forearms horizontal when in the neutral (i.e., middle of the range of movement) position to make long operations more comfortable and to give a greater range of movement vertically, allowing the instrument to be comfortably moved up and down equally (Fig. 6). The ideal table height was calculated to be around 21 cm lower than the elbow height of the operating surgeon.
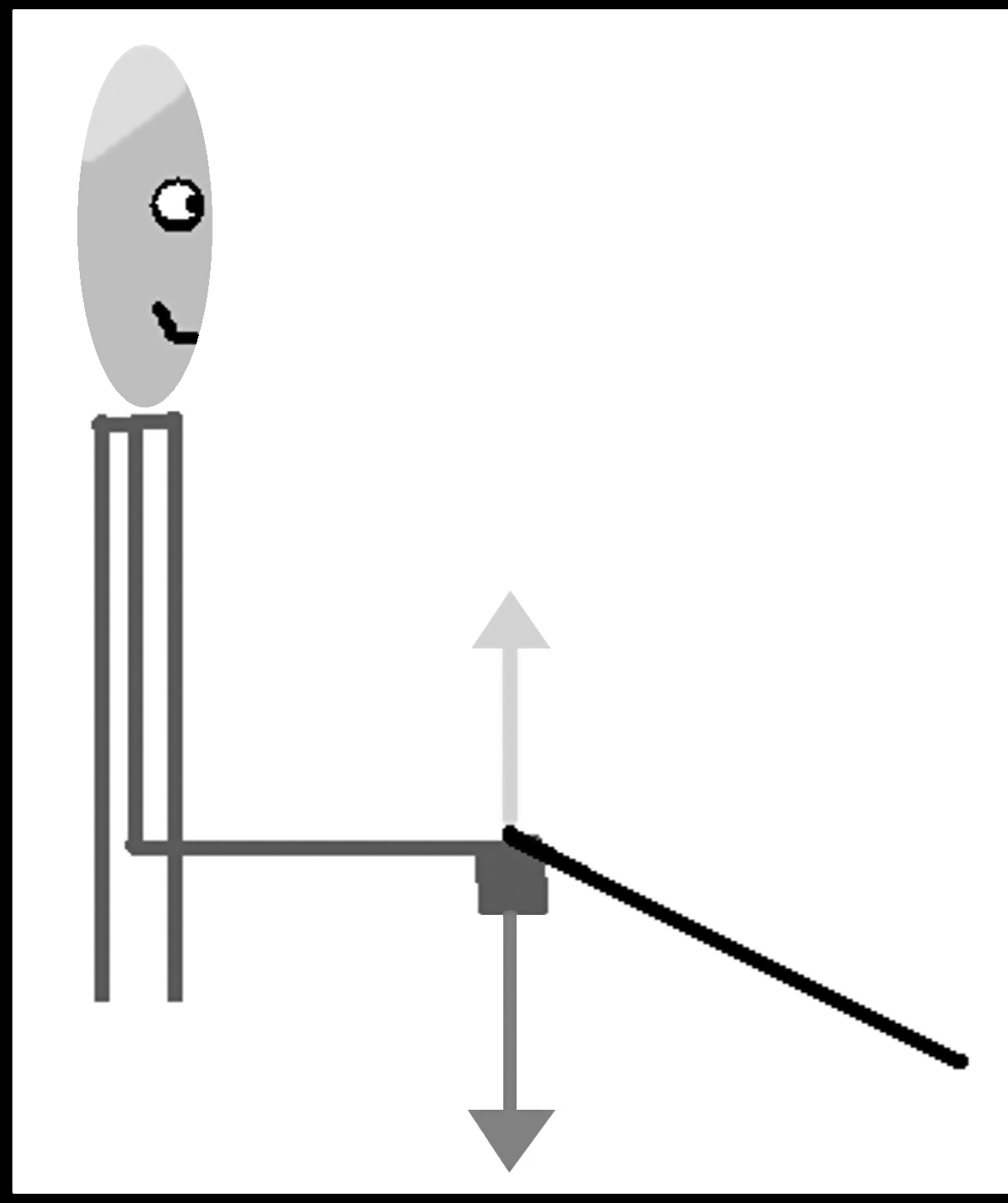
Diagram showing the comfortable movement of instruments in the vertical plane.
The angle of the instrument entering the abdominal port may be greater than 37 degrees from horizontal, if the organ is slightly medial from the edge or the abdomen becomes deeper through insufflation. This is not a problem, as the surgeon can quite comfortably adapt to this small change by either lowering the table slightly further or just raising their hands slightly, while keeping their elbows at their side. Conversely, if the patient is rolled onto their side, then the angle will become shallower, and the table can be slightly raised.
A number of other measurements could be taken to help improve the ergonomics of surgeon and assistant positioning during long procedures. By comparing shoulder height with eye height and laparoscopic screen height, we determined whether we could stand our surgeons with their shoulders overlapping and still have a clear view. This would allow both the OS and AS to keep in line with the target organ and screen. The camera operator's arm can be flexed under the operating surgeon's arm, so the camera is held in the midline of the operating surgeon, as per the diamond rule. The eye height for all our surgeons was higher than anyone else's shoulders, although in 1 case, it was only 2 cm higher, potentially obstructing their view. This can be avoided by seating the camera operator in front and to the side of the operating surgeon, also allowing them to rest their elbow on the edge of the table for increased support.
Foot length was to be used as an estimate of how much space anteroposteriorly each surgeon took up. This can be measured quite diplomatically, unlike other attributes (such as abdominal girth) that would provide a similar estimate for this value. Ultimately, it was of limited use, since feet can overlap by fitting between another surgeon's and under the edge of the table, for example. We ended up drawing our surgeons as thin lines instead, making the diagrams less busy and easier to interpret. By rotating the table slightly according to the position of the target organ, we can accommodate the bent knees of the camera operator, when seated as described above.
Patients of a certain age do not require the whole table length, and all the children <10 years could fit on the operating table with the foot folded down (150 as opposed to 210 cm), giving better access to the operating team. Larger scopes are of benefit in older children, and abdominal depths seemed to correlate with the age and weight, so the larger scope (10 mm), allowing more light, should be used for patients weighing more than 25 kg or those over 10 years of age, with the smaller 5-mm scope used for patients under 25 kg and less than 3 years.
We found that for a third of the time, our surgeons were twisting >50% from their midline and a third of the time they were stretching to almost 50% of their limit. These did not always apply to the same surgeons, and a large degree of rotation was not always accompanied by a large amount of stretching. It would be interesting to see how commonly these physically demanding positions are employed in other centers and among adult laparoscopic surgeons, as there does not seem to be a great deal in the published literature on the subject.
Despite the frequency of these positions, we did not find any correlation between predicted and actual discomfort. A possible reason for this is that our scale diagrams were snapshots of a moment in time near the start of the operation. We noted from some of the recorded movements of the surgeons that they were unlikely to stay in one place if they were uncomfortable. Other errors in measuring rotation and stretch could include errors of estimation and measurement. Marking the position of port sites after the operation by measuring the distance between them, then drawing them on a rough abdominal diagram, could be made more precise by measuring the distance of each port in terms of how far proximal or distal and lateral it was relative to the umbilicus. However, this would yield only a slight improvement in the accuracy of recording stretch and rotation, as the distances involved are so small. Producing these scale diagrams by using MS Paint (Windows OS; Microsoft Corporation, Redmond, WA) was very time consuming. Those familiar with more advanced imaging programs could reduce the time taken, although surgeon movement during the procedures still makes them of somewhat limited value. Ideally, an overhead video camera would show where the surgeons were standing as well as any twisting or stretching throughout the operation. Centers where this is a possibility could perhaps benefit from observing the positions of their operating team and help improve upon our work. Recording the internal operative procedures and counting the “unforced errors” as a procedure progresses could also be used to measure the impact of progressive discomfort and concentration.
By recording a starting value, we were hoping to be able to plot graphs of “change in comfort over time” for each surgeon in each operation, and then, compare these to similar charts after implementing any recommendations to test their effectiveness. We found that since our surgeons were used to dealing with a degree of discomfort in operations, they very rarely strayed below 7 of 10 (which still rates as comfortable) even when they admitted their neck and shoulder was aching. We would, therefore, recommend simplifying this to a scale from 0 to 5, with more emphasis on the descriptions, rather than the numbers (e.g., very uncomfortable, 0; fairly uncomfortable, 1; slightly uncomfortable, 2; slightly comfortable, 3; fairly comfortable 4; very comfortable 5). We also measured mood and alertness, thinking that how tired or happy the team was might affect their comfort. They were almost always “happy” and “very alert,” so we think this could be excluded for any other studies, as starting comfort would probably account for this. The discrepancy between predicted and actual discomfort may also be partly due to the fact that we recorded reduction in comfort even if they had nonpostural causes (e.g., hunger or preexisting aches), which we would not expect to be affected by position. Discomfort did seem to increase with time in prolonged operations, but these were too few to analyze with significance. Ultimately, we need data from more operations and longer procedures to see if comfort can be significantly affected by theater layout. Obviously, the development of the purpose-built laparoscopic operating theaters, where multiple screens can be moved more flexibly in vertical, as well as horizontal, planes, should reduce the risk of twisting in the surgeon's spine. However, these are expensive to implement and hard for many pediatric centers to justify, especially where laparoscopic procedures are still relatively uncommon and the benefits of increasing surgeon comfort to improve operative outcome are hard to prove.
Surgeon's discomfort may well contribute to surgical errors, and data suggest that at least half of all surgical complications are avoidable. 4 Previous efforts to implement practices designed to reduce surgical-site infections or anesthesia-related mishaps have been shown to reduce complications significantly. 5 A growing body of evidence also links teamwork in surgery to improved outcomes, with high-functioning teams achieving significantly reduced rates of adverse events. 6 In 2008, the World Health Organization (WHO) published guidelines identifying multiple recommended practices to ensure the safety of surgical patients worldwide. 7 We would suggest, for pediatric laparoscopic surgery, that if checklists of procedures are prepared for the four main categories of individuals involved in the procedure [anesthetist (not included in our study), surgeon, scrub nurse, and circulating theater staff ] and these are then laminated, they can be continuously written on with whiteboard markers, ticked off as having been considered, and wiped off after each operation. Checklists in surgery are becoming more mandatory and recommended. 8 Based on our findings, we suggest a number of broad categories to include in a checklist. These include scaled maps of theater layout, extraneous light sources, position of the table in theater, position of the scrub nurse and their equipment, and space for the circulating nurse. Scaled maps of the operating theater, with recommended placement and orientation of the equipment, are relatively easy to draw up.
Extraneous light is one of the main areas of distraction during laparoscopic surgery. Ambient light should be minimized to reduce the clarity and contrast of the image on the screen, and direct light sources should, ideally, always be at right angles to the screen so as not to reflect into the surgeons' eyes. The best way to work out if a light source will be a problem is to draw a line from the surgeon standing most lateral to the monitor and reflecting this off the opposite edge of the monitor screen at an equal and opposite angle (Fig. 7). Anything within this cone will reflect into the surgeon's eyes off the screen. Surgeons standing more directly in front of the screen will have a narrower reflective cone. A light source in view behind the screen will cause a surgeon's pupils to constrict, as well as leave an imprint on their retina in an otherwise darkened room.
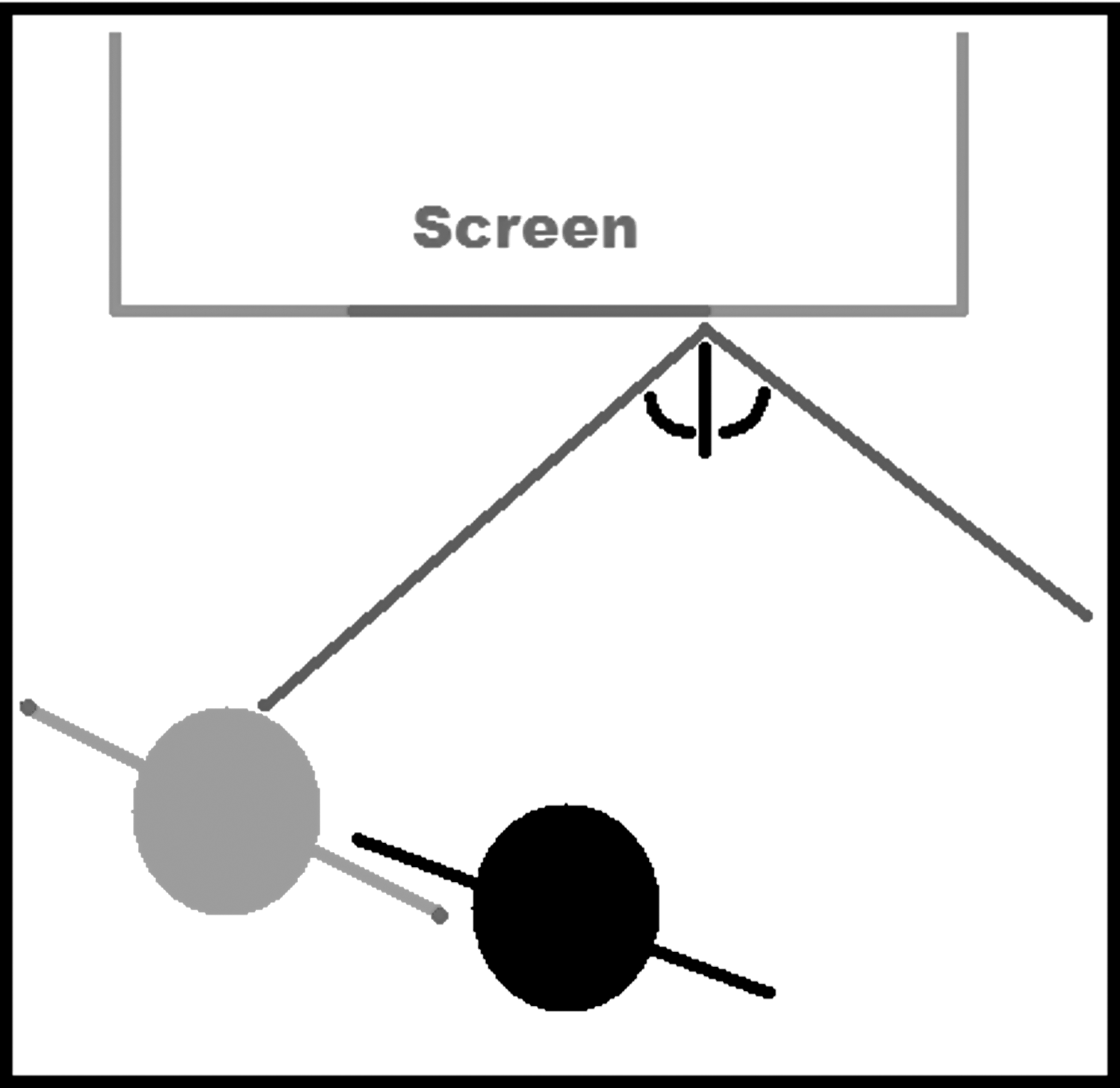
Schematic diagram showing how light reflections can be avoided by avoiding angle of direction of light source to surgeon (shown in gray).
The theater could be completely blacked out, but this does not allow the anesthetist light to work by, and is impractical and possibly dangerous for circulating personnel, increasing the risk of tripping over cables while fetching things for the operating team. In our theater, the anesthetic room light and lay-up room lights were left on, as these were outside the surgeon's direct light arcs. The lay-up room window was blinded by placing a screen or drape over it, and the PACS computer screens (for viewing X-rays) were switched off when not in use. The table position within the theater is often not changed during a procedure. For some operations, we identified important variations in the operating table position. By rotating the table, the surgeon was able to stay in line with the stack and target organ. By moving the table and not the stack, it was ensured that the stack was always in an optimum position and angle. This table rotation also allowed space for the AS to sit in front and to the side of the OS. If the table were straight, there would be no room for a sitting person's legs in front. This configuration also lowered the AS, so the OS stood perfectly in line with the screen, with their elbows by their sides.
The scrub nurse's equipment table was placed opposite to the surgeon, giving everyone more room and allowing the passing of instruments face to face with the surgeon. A stool set aside for the scrub nurse to sit on during long operations is helpful for comfort but could reduce scrub-nurse movement. A second screen, if available, may be placed at right angles to the main screen outside the reflective arc, as neither the scrub nurse nor the anesthetist would be able to see the main screen in the initial arrangment. Last, space should be left around the edge of the movable equipment, so that circulating personnel can move freely around the theater.
Based upon these principles, we suggest that plans for operations could be produced for surgical procedures on organs in each of the four main quadrants of the abdomen (upper and lower left, upper and lower right) (Fig. 8). These would allow theater staff to set up any basic theater in a more optimum configuration for laparoscopic procedures. For hospitals without dedicated or purpose-built laparoscopic theaters, such as an OR1, these plans allow for operative layout to be modified before a surgeon begins to operate, improving efficiency and reducing stress to the team during the procedure. In turn, this should improve operating outcomes and reduce morbidity to the patient.
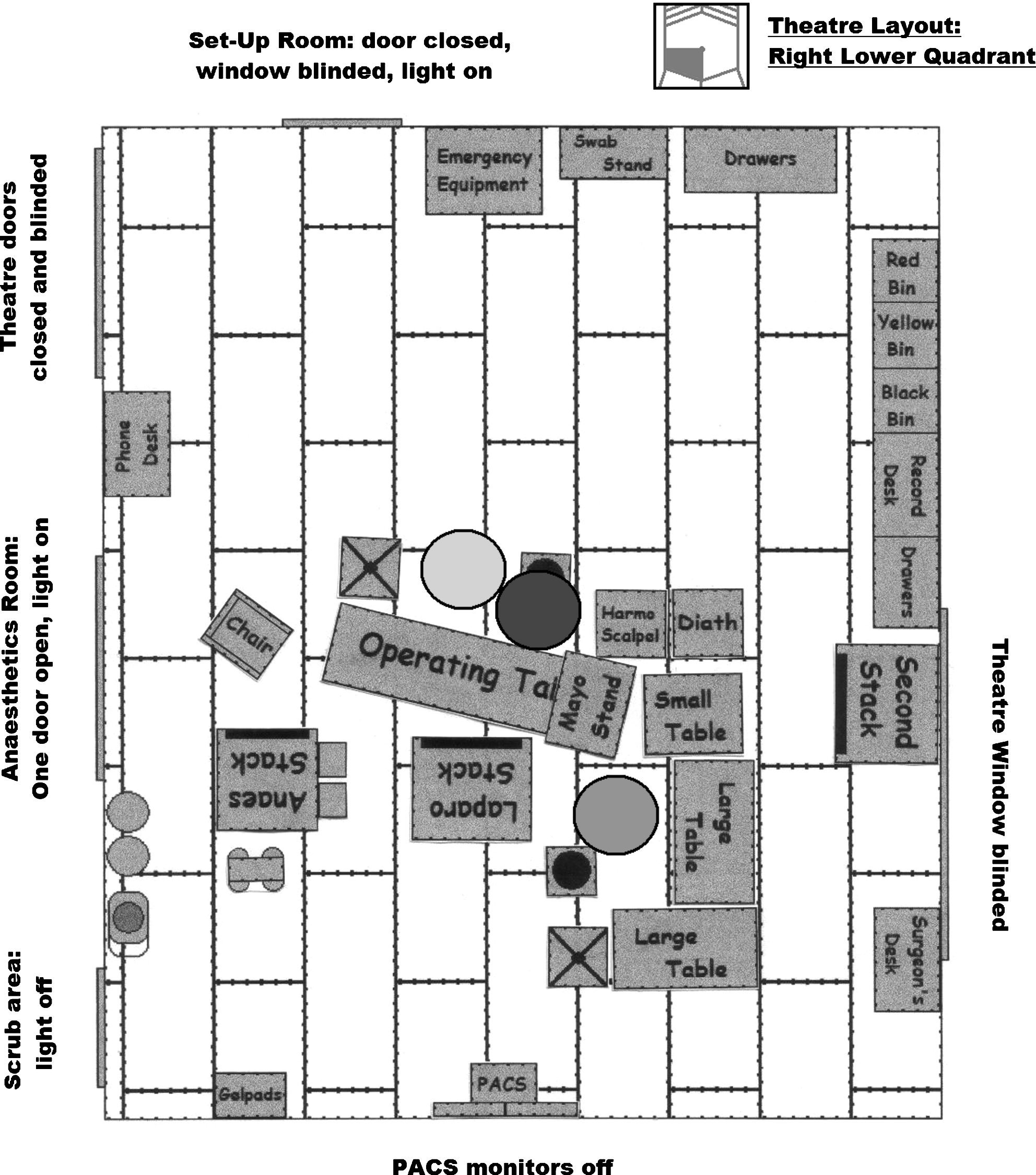
Sample final theater layout plan for an operation in the right-lower quadrant.
Conclusions
Our study has shown that it is possible to calculate the best table height relative to the operating surgeon for laparoscopic procedures. A wide variety of potentially uncomfortable positions are adopted during laparoscopic procedures. However surgeon comfort does not seem to be affected by position during short procedures and more work is required to measure position and discomfort during longer procedures. Taking measurements and producing scaled diagrams could allow teams to improve the ergonomic lay out of their theatre for laparoscopic surgery, although video footage may be of more use in assessing surgeon posture.
Disclosure Statement
No competing financial interests exist.