
Abstract
Abstract
Background:
Complex laparoscopic tasks are nearly impossible to complete when the telescope is pointed toward the operator (i.e., paradoxic image). Attempts at image manipulation have been reported, but altered monitor displays may introduce even more confusion. The availability of high-quality, lightweight, head-mounted displays (HMDs) now allows individualization of the laparoscopic image. We studied the effect of manipulation of the paradoxic image on task performance.
Study Design:
Fifteen surgical residents (PGY levels 1–5) were timed while performing the standard “bead pass” skill from the Fundamentals of Laparoscopic Surgery (FLS®) course. Conventional diamond-shaped configuration, with telescope and camera in line with the operator and overhead image projection at the opposite end, served as control. A paradoxic image was created by placing the telescope at the opposite side of the box trainer (180 degrees from operator), and the task was repeated with different image corrections: (1) paradoxic image as-is; (2) left-right reversed image (mirror); and (3) left-right reversed and upside-down image (i.e., inverted mirror). Times were recorded and analyzed for intra- and interoperator variance and compared with control.
Results:
Time-per-bead was 7.5 ± 1.5 seconds (standard error of the mean) in controls. With the as-is paradoxic image, time-per-bead was 164.1 ± 80.8 seconds/bead. All but 2 residents failed to complete the task. Times were 120.0 ± 55.9 seconds/bead for the mirror image and 46.7 ± 26.0 seconds/bead for the inverted mirror image (P < 0.01; ANOVA and Kruskal-Wallis).
Conclusions:
The difficulty of performing a relatively simple laparoscopic task with paradoxic image display was almost insurmountable. Left-right image inversion was not sufficient to correct the handicap. Inverted mirror-image projection significantly improved performance, which almost reached control levels. The availability of personal image-display devices may, in the future, allow image customization for task performance in suboptimal conditions during endoscopic surgery.
Introduction
One of the most challenging tasks during laparoscopic surgery is operating when the camera is directed toward, rather than away from, the operator. This produces a mirror image, also known as a paradoxic image. Mirror imaging creates paradoxic motion and requires a high degree of voluntary disconnect between visualization and hand motion while operating. Paradoxic imaging becomes more problematic during complex procedures. Given the limitations of the operating-room set-up, the surgical assistant is often placed on the opposite side from the surgeon (and the telescope) and is faced with the challenges of a paradoxic image. These difficulties also provide a barrier to effective resident teaching of laparoscopic procedures. A simple solution might be to produce a mirror image of the telescopic view for the assistant—thereby “correcting” the paradoxic motion. Johnston et al. 10 reported improved performance from using an image converter, which essentially produced a simple mirror image (projected on the assistant's monitor). Test subjects were able to improve their ability to perform simple laparoscopic procedures in these suboptimal conditions. A simple mirror image does not correct all aspects of the paradoxic motion, however. In addition to the awkward mirror-image view of the operating field, to-and-fro motions remain uncorrected: As an instrument travels away from the assistant, it travels toward the telescope and, therefore, appears as “zooming in” on the image display. In addition, the projection of altered images on a large screen, visible for all, creates added confusion to other members of the operating team. The introduction of light-weight head-mounted displays (HMDs) may usher in an era of personalized laparoscopic image display, which, in turn, could allow more sophisticated image manipulation. We sought to further examine the effects of paradoxic image correction.
Methods
Fifteen surgical residents (PGY levels 1–5) were timed while performing the standardized “bead pass” skill from the Fundamentals of Laparoscopic Surgery (FLS®) course. All test subjects were first timed while performing the exercise in the classic configuration. The set-up was slightly modified from the standard FLS camera system by using a 10-mm 0-degree telescope (Karl Storz Endoscopy, Culver City, CA) and laparoscopic camera control unit (model 22-2000; Karl Storz Endoscopy). The image was projected overhead on the wall immediately behind the endotrainer unit via an LCD projector (model XL8U; Mitsubishi, Irvine, CA). This exercise served as the control.
The telescope was then moved to the opposite end of the endotrainer, with the lens facing the operator, generating a paradoxic image. Each test subject performed the bead-pass test under three different circumstances. The order in which the three tests were performed was assigned randomly. The paradoxic image was projected “as is,” as a mirror image and as an upside-down (i.e., inverted) mirror image, using the image features of the LCD projector (Fig. 1). The aim was to pass six beads with a maximum time limit of 10 minutes. Times were recorded and analyzed for intra- and interoperator variance, when compared with the classic laparoscopic monitor position (control).

Experimental set-up. Paradoxic image was projected “as-is,” as a left-right mirror image and as an upside-down, left-right mirror image (“inverted mirror”).
In the control exercise, the time necessary for the full exercise (12 beads) was averaged for all 15 participants (mean ± standard deviation). Because the full 12-bead exercise could not be completed by all in the experimental exercises, time per bead was used as well. The time-per-bead values for each participant (mean ± standard deviation) was averaged for all participants (mean ± standard error of the mean; SEM). These values were used for statistical analysis between groups (single-factor analysis of variance; ANOVA). Because individual experiences varied greatly, intraoperator analysis was also performed, using a nonparametric test (Kruskall-Wallis).
Results
In the control exercise (classic laparoscopic monitor position), all 12 bead passes were completed in a mean of 90.0 ± 9.5 seconds. The mean time per bead pass was 7.5 ± 1.5 seconds (mean ± SEM). There was no difference between mean bead time between the first and last beads (8.2 ± 1.6 and 7.5 ± 1.9 seconds, respectively). In the paradoxic image experiment, only 2 residents were able to complete a six-bead transfer in the maximum allotted time of 10 minutes. The mean time per bead in the as-is (i.e., paradoxic) image group was 164.1 ± 80.8 seconds, a more than 20-fold increase over the control group. The mean time per bead for the mirror image projection of the paradoxic image was 120.0 ± 55.9 seconds. With the paradoxic image in the mirror- and upside-down position, the mean time per bead was 46.7 ± 26.0 seconds (Fig. 2). This was significantly lower than the paradoxic image (P < 0.01), although it did not reach control levels. To correct for the wide range of times (interoperator variation), times were compared for each test subject (Fig. 3). The inverted-mirror image yielded significantly shorter times than the as-is paradoxic and mirror images (P < 0.05; Kruskal-Wallis test). There was no difference in per-bead time between the first and the last bead (45.6 ± 20.0 and 42.7 ± 19.87 seconds, respectively).
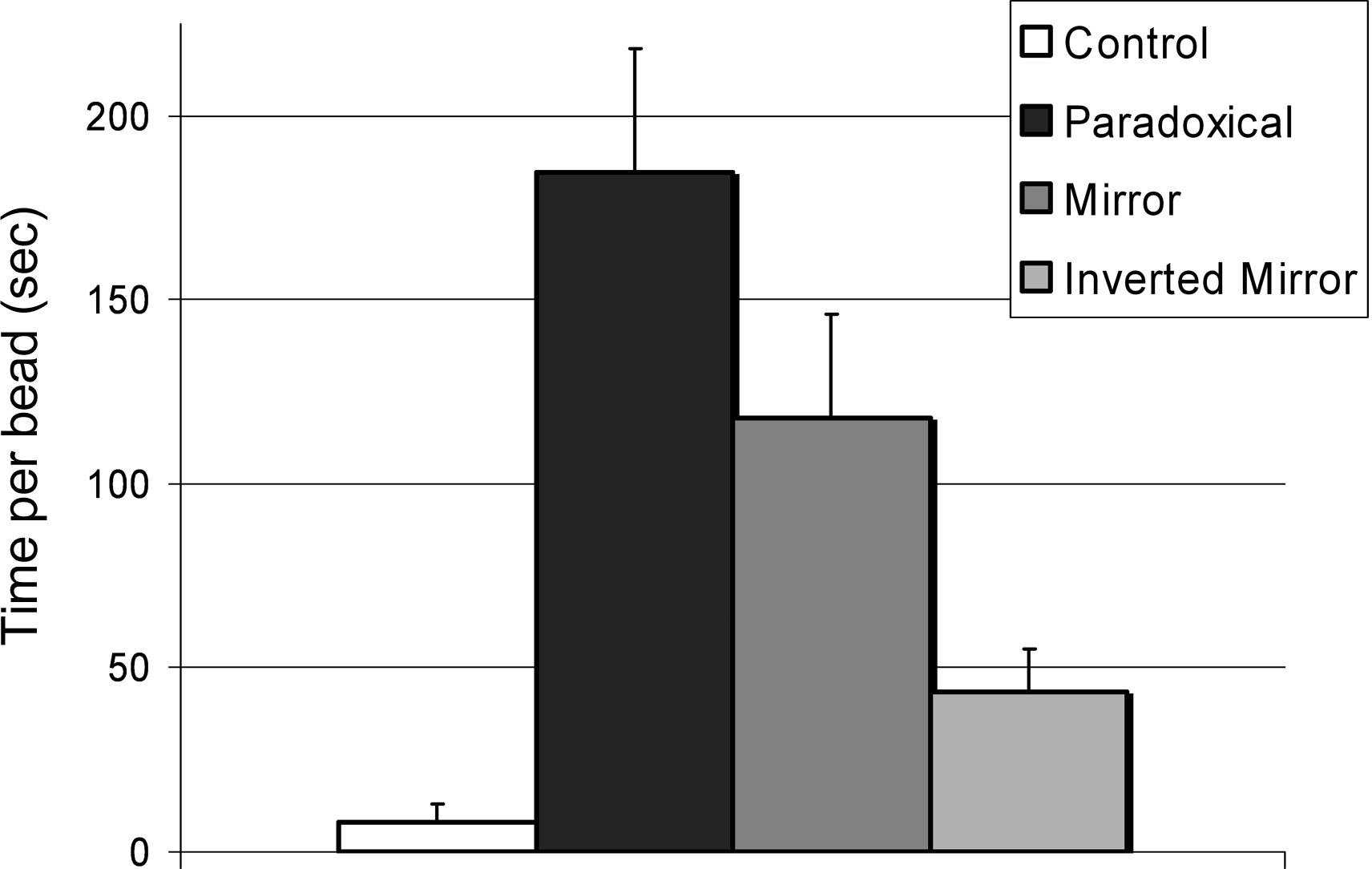
Average time per bead for each set-up (see Fig. 1 and text for details). Times represent averages for all beads and all study subjects and are expressed as mean ± standard error of the mean (SEM). Differences between groups are statistically significant (ANOVA).
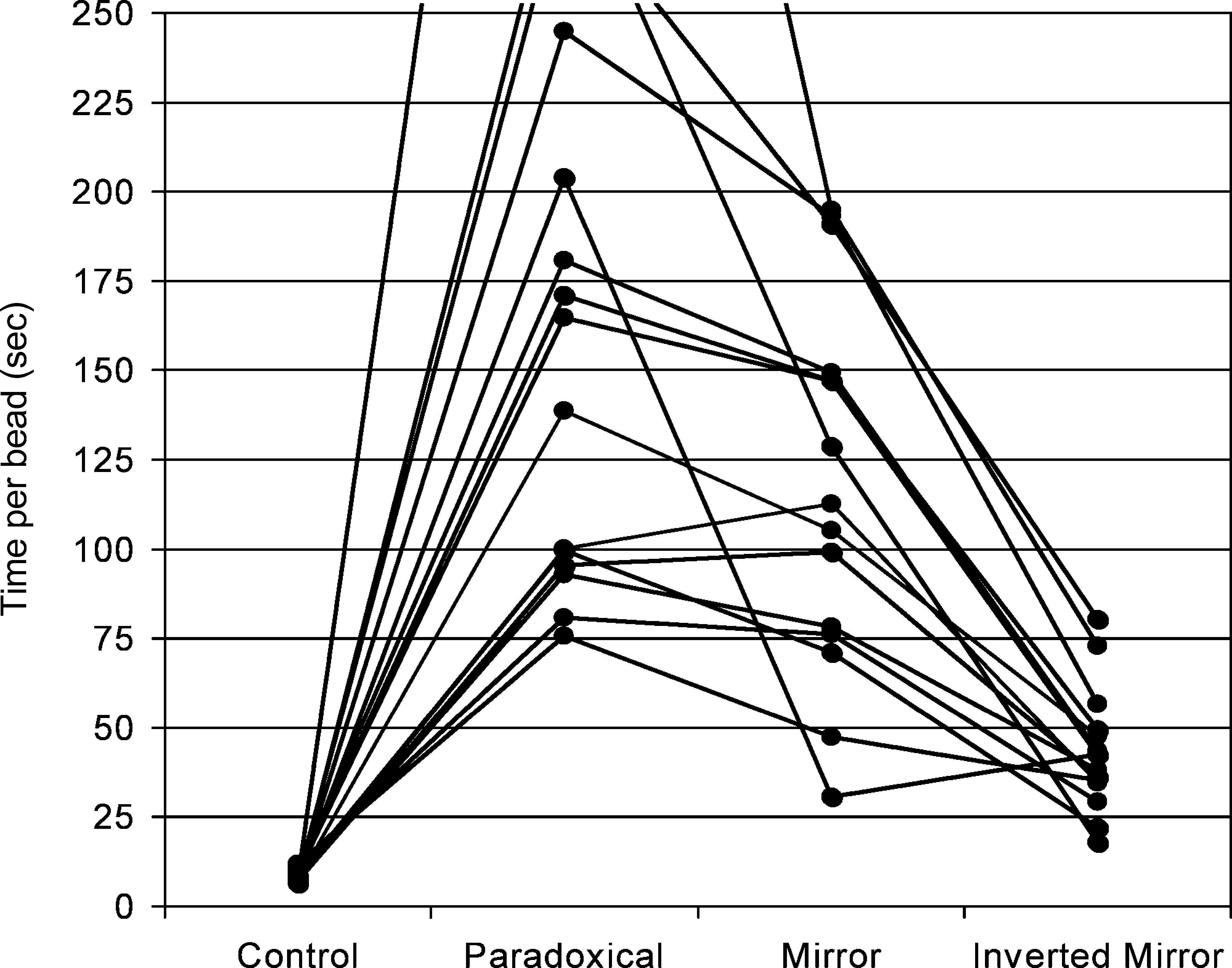
Individual times, illustrating the wide variability between study subjects. Differences between inverted mirror image and paradoxic image are significant (P < 0.05; Kruskal-Wallis).
Discussion
Port placement and image positioning are crucial to efficient laparoscopic surgery. The most natural set-up is the diamond-shaped configuration, with the telescope at the opposite end of the target organ (i.e., surgeon's eyes) and an instrument (i.e., hand) on either side of the telescope-target axis. Slight variations of this configuration are inevitable in real-life laparoscopy, but major deviation significantly decreases surgical performance.1,11,12 Meng et al. 13 studied how varying the optical angle, defined as the angle formed by the line of action (i.e., working ports) and the line of vision (i.e., telescope) affected the time to accomplish a standardized task of tying a square knot. They found that the optimal position is at an optical angle of 0 degrees and the optimal range is 0–60 degrees. As the optical angle increased from 0 to 180 degrees (paradoxical image), the time to perform the task increased. Additionally, several of their subjects were unable to perform the task while operating at optical angles between 120 and 180 degrees. In a similar study by Medina, 14 intracorporeal knot tying at any angle greater than 60 degrees was significantly more difficult than at the standard 0-degree angle (diamond configuration). The worst position was with the camera placed at 180 degrees. Half of the surgeons required 14–25 minutes to perform a single intracorporeal knot while operating with a paradoxic image.
This paradoxic image projection renders the performance of complex laparoscopic tasks nearly impossible. Any motion to the right will show on the screen as a movement to the left, and near-to-far instrument movement by the operator appears as a far-to-near movement. Because of patient and operating-table limitations, this situation often occurs during thoracoscopy, when the surgeon and assistant must stand on opposite sides of the field. The use of a second monitor alleviates the need for the assistant to operate while looking back at the primary monitor—but the projected image on the accessory monitor is paradoxic. 1 Despite two decades of research and refinements in endoscopic image acquisition and display, the problem of the paradoxic image has rarely been addressed. One now-defunct device allowed the creation of a mirror image. 10 We studied the effect of two forms of image manipulation to overcome paradoxic motion in laparoscopic surgery.
A typical laparoscopic instrument has six degrees of freedom, which represent four separate motions: motion in a horizontal plane (y-axis, or yaw), motion in a vertical plane (z-axis, or pitch), and to-and-fro motion along the instrument's axis (x-axis), combined with axial rotation of the instrument (roll). In a paradoxic image set-up, some of these motions are distorted: Uncorrected, the paradoxic image leaves motion along the z-axis unaffected (up-and-down motion is reproduced faithfully on the screen), but all other motions are distorted. In a mirror-image projection, motion along the z-axis (pitch) remains unchanged; Roll and yaw are now corrected, but the to-and-fro motion (x-axis) remains paradoxic: As the instrument tip moves away from the operator, it moves toward the observer and vice-versa. In an inverted mirror-image projection, this fourth motion (to-and-fro along the x-axis) is corrected, although the pitch is now inverted. Our study shows how image manipulation of a paradoxic image can affect an operator's ability to perform simple tasks laparoscopically. The average time to transfer a single bead in a paradoxic image situation (almost 3 minutes) was nearly 20 times greater than under control circumstances (7–8 seconds). When the paradoxic image was projected as a mirror image, bead-transfer times improved only marginally, and many study subjects still failed to complete six transfers under the allotted 10 minutes. Although left-to-right motions or displays were corrected, the to-and-fro movements were not. When the image was not only mirrored, but inverted (i.e., upside-down), bead transfer was completed by all subjects and average times neared controls. Reality was obviously distorted with using an inverted mirror-image projection, as was the pitch (motion along the z-axis), but this was more than compensated for by the correction of all other degrees of freedom. The likely explanation is that, in laparoscopic surgery, pitch is less important than to-and-fro motion of the instrument: As the telescope (camera) and instrument are not pointing at each other, but are both angled toward the surgical target, the perception of pitch excursion is substantially reduced—whereas the near-to-far (i.e., to-and-fro) motion becomes more important, particularly during fine-motion procedures.
It is interesting to note that some are more troubled by paradoxic motion than others, and this variability did not correlate with level of training or surgical experience. Yet, as Figure 3 shows, even the most facile subjects benefited greatly from the inverted mirror-image projection (P < 0.05, Kruskal-Wallis test). The average time was similar for all transferred beads (first and last bead time 43 and 46 seconds, respectively), suggesting that the study subjects did not need a period of adaptation to perform in this unusual image environment. On the other hand, even this extreme manipulation could not completely eliminate the handicap of paradoxic image display, as average per-bead times remained substantially greater than in controls.
Conclusions
This is the first study to show how the manipulation of a paradoxic image to an inverted mirror image can improve laparoscopic tasks. It is premature to suggest that accessory monitors in the operating room should display an upside-down mirror image of the laparoscopic target, as this would create more confusion for other members of the surgical team. However, the introduction of lightweight individual head-mounted displays (i.e., video goggles) may facilitate the customization of the image display. 15 In the future, temporary modulation of the displayed image could be achieved at the flick of a switch, enabling a surgeon to perform a task in paradoxic circumstances, while everyone else sees the “real image.” Clearly, this theory will have to be tested with more complex manipulations in vitro and field tested in vivo.
Footnotes
Disclosure Statement
No competing financial interests exist.
Presented at the Annual Meeting of the Society of American Gastrointestinal and Endoscopic Surgeons, April 9–12, 2008, Philadelphia, Pennsylvania.