
Abstract
Abstract
Introduction:
Bile leaks after laparoscopic cholecystectomy (LC) can be difficult to diagnose early. The aim of this study was to investigate the clinical features of minor bile leaks and to discuss how to manage patients who revisit the hospital with minor bile leaks after LC.
Patients and Methods:
From January 2001 to September 2007, 2219 LCs were performed at the Ajou University Medical Center. Twenty-four patients (1.0%) who presented with a bile leak or bile duct injury after a cholecystectomy were identified. The patients with minor bile duct injury were divided into two groups, depending on whether they revisited the hospital (group 2) or not (group 1) after LC.
Results:
Seventeen of 24 patients had minor bile leaks. The characteristics of patients in group 2 were long hospital stay, short operation time, and low frequency of indwelling surgical drains. Ten of 17 patients (58.8%) revisited the hospital at a mean of 7.0 ± 2.7 days after the LC. However, 3 of 10 patients (30%) were discharged from the ER with atypical abdominal pain and returned to the hospital again within 5 days due to recurrent abdominal pain. There was a significant correlation between hospital stay and time to endoscopic retrograde cholangiopancreatography (ERCP) (P = 0.008) and between hospital stay and PCD (P = 0.028).
Conclusions:
Most minor bile leaks were managed by ERCP and/or percutaneous drainage. However, early diagnosis was difficult when patients revisited the hospital within 7 days after the LC. Therefore, early ERCP should be considered in these patients to diagnose the bile leak early and limit needed hospital stay.
Introduction
Biliary endoscopic procedures have become the treatment of choice for the management of bile leaks; this is because surgical management of bile leaks has been associated with a high morbidity and mortality.7,8 Although some investigators prefer the endoscopic procedure, others recommend early endoscopic retrograde cholangiopancreatography (ERCP) as a way to decrease total hospital stay; the increased time in the hospital, in some studies, has been directly related to the waiting time for an ERCP. 9 However, the appropriate timing for performing an ERCP, in patients that revisit the hospital after an LC, is unknown. Therefore, this study was designed to investigate the clinical features of patients with minor bile leaks and discuss their management when they return to the hospital with minor bile leaks after an LC.
Patients and Methods
From January 2001 to September 2007, 2219 LCs were performed at Ajou University Medical Center. Twenty-four patients, who presented with bile leaks or bile duct injury after a cholecystectomy, were identified, including 7 major and 17 minor injuries. Among 24 patients, we selected 17 patients that had minor bile duct injuries and divided the patients into two groups, based on whether they revisited the hospital (group 2) or not (group 1) after the LC. The bile leaks in group 1 were immediately recognized after the LC, whereas those in group 2 were recognized only after they revisited the hospital via the emergency room (ER) after the LC. Nine patients were male and 8 patients were female; age ranged from 24 to 63 years. We collected consecutive identification information on the patients that presented with bile leakage and were managed for major bile duct injury. We retrospectively reviewed the medical records of all patients and analyzed the data, including demographic information, clinical presentation, operative records, ERCP procedures, radiologic intervention, and total hospital stay.
Major bile duct injuries were defined as transection of a major bile duct (or an incision of the lateral wall). All other injuries were classified as “minor” leaks from the cystic duct or hepatic gallbladder bed. 7 The diagnosis of a bile leak was defined as the presence of bile leakage that was confirmed by ERCP or the appearance of bile through a surgical drain or percutaneous drainage.
The LC was performed by the standard four-trocar technique (two 10-mm and two 5-mm ports). We used a closed suction drain when there was a bleeding tendency or purulent material. The indications for LC were gallbladder polyp (n = 2), gallbladder stone (n = 1), acute cholecystitis (n = 5), chronic cholecystitis (n = 7), and gallbladder adenomyomatosis (n = 2). Intraoperative cholangiography (IOC) was used when bile duct stones were suspected or in cases with anatomic complications during the dissection. In the present study, an IOC was performed in 1 patient; however, it did not reveal a bile leak. An abdominal computed tomography (CT) was performed in patients that complained of sustained or increasing abdominal pain after the LC. When there was a large fluid collection, percutaneous drainage was performed by a radiologist, using 7 ∼8-Fr pigtail catheters, under ultrasound or fluoroscopy guidance.
All ERCPs were performed by two endoscopists. In patients with a bile leak after the cholangiography, therapeutic procedures, such as sphincterotomy, retrograde biliary drainage with a stent (ERBD), and nasobiliary drainage (ENBD), were performed. Nasobiliary drains or stents of 7Fr in size were placed, according to standard techniques. The ENBD was removed when the bile leakage stopped and closure of the fistula was cholangiographically confirmed. The stents of the ERBD were removed after 8 weeks. If there was clinical and radiologic evidence to show that the bile collection had resolved and there were no signs of further leaking, patients were discharged.
Statistical analysis
Statistical analysis was performed with the chi-square test or Fisher's exact test, Mann-Whitney U test, and Spearman's correlation. A P-value of <0.05 was considered statistically significant.
Results
Clinical findings
Seventeen patients presented with a minor bile leak; 7 patients were immediately recognized as having a bile leak after the LC, whereas 10 patients were recognized when they revisited the hospital via the ER after the LC. Among the 17 patients, 15 patients electively underwent surgery, whereas 2 patients underwent urgent surgery. The characteristics and surgical outcomes of all patients are described in Table 1. The hospital stay in group 2 was significantly longer than in group 1 (P < 0.05, respectively). The operative time in group 2 was significantly shorter than in group 1 (44.5 versus 79.2 minutes) (P < 0.05). There were no significant differences in age, gender, and laboratory findings between groups 1 and 2 (P > 0.05).
LC, laparoscopic cholecystectomy; ASA, American Society of Anesthesiologists; NS, not specific.
Diagnosis and management
The majority of patients (11/17) presented with postoperative abdominal pain. However, 6 patients were asymptomatic and presented with bile drainage from a surgical drain. The diagnosis was confirmed by surgical drain in 6 patients, by percutaneous drainage after CT in 6 patients, and by ERCP in 5 patients. The diagnosis and management are described in Table 2. More patients in group 2 underwent percutaneous drainage than patients in group 1 (P < 0.05).
aRHD, aberrant right hepatic duct; PCD, percutaneous drainage; NS, not specific.
Rehospitalization after initial surgery
Ten of 17 patients (58.8%) were admitted via the ER, at a mean of 7.0 ± 2.7 days after the surgery, with the complaint of abdominal pain. The mean duration of treatment was 15.1 ± 7.3 days. The characteristics of the patients are described in Table 3. On physical examination, 6 patients presented with direct tenderness, 3 patients presented with rebound tenderness, and 1 patient had jaundice without fever. All patients underwent an abdominal CT scan to identify other intra-abdominal problems.
CDS, cystic duct stump, aRHD, aberrant right hepatic duct; ERBD, endoscopic retrograde biliary drainage; ENBD, endoscopic nasobiliary drainage; PCD, percutaneous drainage; Reop, reoperation.
Among 10 patients, 2 had bile collection on the first CT and promptly underwent percutaneous drainage. One patient (no. 1) did not need any additional procedures; for the other patient (no. 10), however, the volume of bile drainage from the percutaneous drainage did not decrease. Common bile duct stones were identified on ERCP. The patient underwent primary closure of the cystic stump on day 28 after the initial operation; however, we did not find the site of bile leakage because of fibrosis of the operative field.
The remaining 8 of 10 patients had no bile collection on the first CT, and 5 of 8 patients were hospitalized because of unresolved abdominal pain. Four patients (nos. 2–5) were evaluated again with an abdominal CT because of increasing abdominal pain with or without fever, whereas 1 patient (no. 6) underwent nasobiliary drainage plus a sphincterotomy without radiologic intervention (Fig. 1A). Of the 2 of 4 patients that were reevaluated by abdominal CT after rehospitalization, 1 patient (no. 2) was a 44-year-old woman that underwent an LC due to a gallbladder polyp. This patient visited the ER 6 days after the LC and had an abdominal CT (Fig. 1B). She was discharged on day 14 of the second hospitalization. The other patient (no. 3) was a 38-year-old man who presented with a bile leak through the surgical drain. However, the volume of bile drainage was small (i.e., less than 170 cc), and the drain was removed on day 5 after the LC. An abdominal CT was immediately performed to identify the presence of a bile collection; however, there was no fluid collection and the patient was discharged. The patient revisited the hospital, with abdominal pain, 6 days after discharge from the hospital. He underwent percutaneous drainage twice; finally, ERCP revealed bile leakage from a cystic duct stump.

Radiologic and ERCP findings of a bile leak after the LC. (
Since 3 (nos. 7, 8, and 9) of the 8 patients, who had no bile collection on the first CT, presented with unusual abdominal pain and were well controlled by pain medication, they were discharged from the ER. However, they revisited the ER at 5, 1, and 3 days after discharge from the ER. Two of the 3 patients were well managed by nasobiliary drainage plus a sphincterotomy without bile collection; however, 1 patient (no. 7) had a repeat abdominal CT and then underwent percutaneous drainage plus nasobiliary drainage. Patient 7 was discharged on day 16 because of the collection of retroperitoneal air after the ERCP procedures.
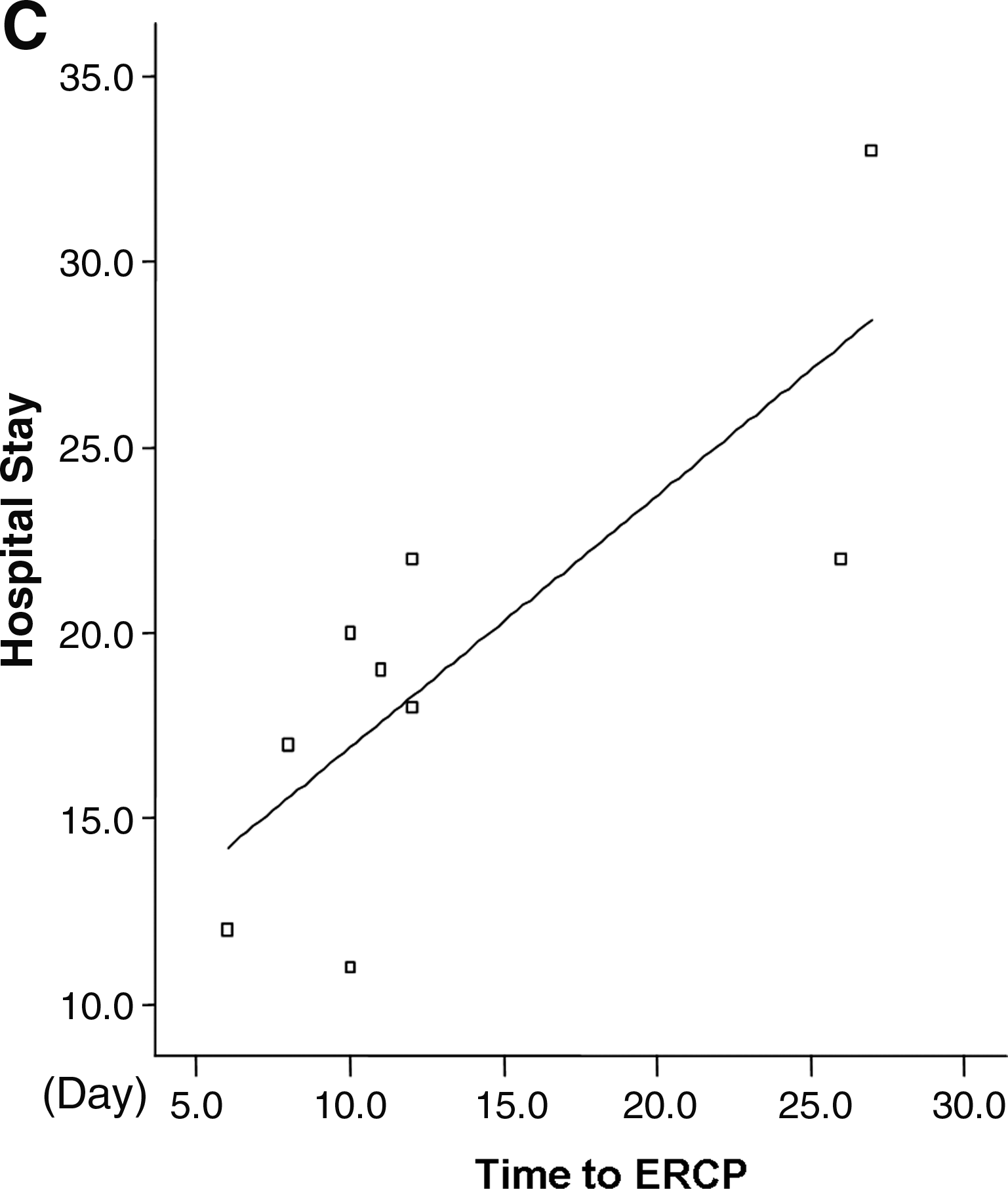
Hospital stays in rehospitalized patients
We analyzed the correlation between hospital stay, time to diagnosis, performing an ERCP or percutaneous drainage, and time to ERCP (Fig. 2). Mean hospital stay was 18.9 ± 7.2 days. There was a correlation between hospital stay and performing a percutaneous drainage (r = 0.688, P = 0.028) and between hospital stay and time to an ERCP (r = 0.814, P = 0.008). However, there were no correlations between hospital stay and time to diagnosis (P > 0.05).
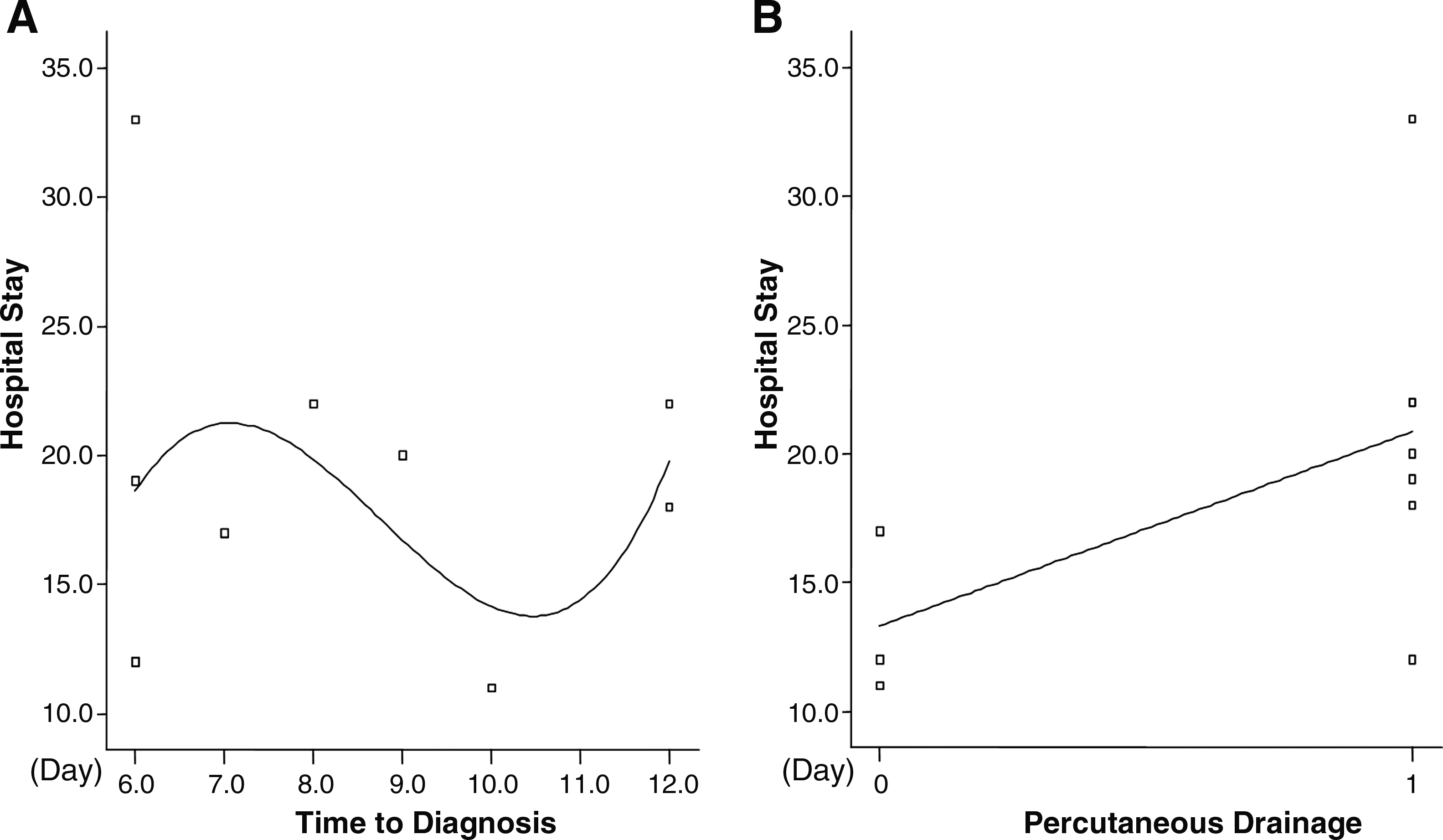
Correlation between hospital stay and other factors in group 2. (
Discussion
Major and minor bile duct injuries are uncommon after LC procedures. Treatments for bile duct injuries are well known to surgeons. Most major bile duct injuries require operative treatment, which provides good results under optimal circumstances. However, most minor injuries, including cystic duct leaks and bile duct strictures, can be treated by endoscopic procedures and/or percutaneous drainage. 10
In the present study, minor bile leaks were found in 17 patients (0.7%). According to a large series, the frequency of bile leaks after a cholecystectomy has been reported to be less than 2%,11,12 and some series have reported that the most common site of biliary leakage is the cystic duct.8,13 However, bile leaks and bile collection may have various etiologies, such as the presence of anatomic variants of the liver during dissection of the gallbladder or small biliary radicles entering the gallbladder fossa, ligation, and/or transection of the bile duct, and dislodgement or malposition of surgical clips.2,8,14 In our study, 9 of 17 patients (52.9%) presented with cystic duct leaks; because the site of the leak was not identified in 5 patients, the number appears to be small. Among the 5 patients, a bile leak from the liver bed was suspected in 3 patients.
For the treatment of a bile leak, a variety of surgical repair techniques, percutaneous drainage, and endoscopic biliary drainage procedures have been used. Surgery was used as first-line management, for some cases, in several studies,11,15 whereas biliary endoscopic procedures are currently the treatment of choice for the management of bile leaks. This is because surgical management of bile leaks is associated with a high morbidity and mortality.7,8 The results of this study showed that 15 of 17 patients (88.2%) were treated by ERCP procedures and/or percutaneous drainage. However, the remaining 2 patients (11.8%) underwent a reoperation. One patient in group 1 had a cystic stump stone, and the other patient, in group 2, had common bile duct stones. None of the 17 patients with minor bile leaks had persistent sequelae.
The findings of this study showed that 10 of 17 patients (58.8%) were admitted via the ER after surgery. It is of interest to note that only 2 patients (20%) presented with a bile collection observed on the first abdominal CT. Moreover, 3 patients (30%) were discharged from the ER because of atypical abdominal pain without the identification of a significant bile collection. As a consequence, this injury was not detected during the early postoperative period because of the minimal amount of fluid collection. Therefore, it is important to recognize postoperatively the characteristic symptoms of this injury; unusual severe abdominal pain, fever, jaundice, and a mild leukocytosis. 16 However, fever and jaundice were not usually present in the patients reported in this study. Previous reports suggest that bile peritonitis is the principal manifestation of an abdominal bile collection; however, this is an uncommon presentation during the early course.17,18
Imaging studies are helpful for confirming diagnosis and aiding in the decisions for subsequent therapy. 19 Moreover, by means of imaging and interventional techniques, bile collections can be effectively drained by percutaneous catheters. 20 When the volume of bile drainage is large, the diagnosis can readily be made, and a prompt ERCP is indicated. Some investigators have suggested that early ERCP may decrease total hospital stay; increased time in hospital has been directly related to the waiting time for an ERCP. 9 The results of this study also showed that there was a correlation between hospital stay and time to ERCP and between hospital stay and PCD in group 2. However, hospital stay was not correlated with surgical drains. Figure 3 shows an algorithm for management of bile leak after an LC in our hospital.
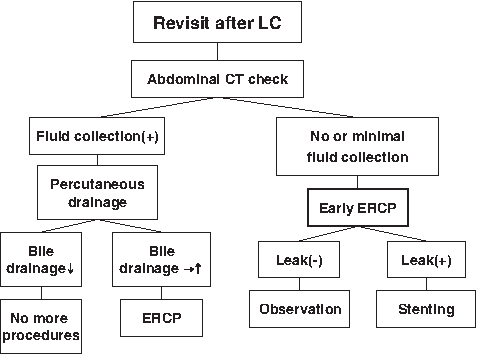
Algorithm for management of bile leak after an LC.
Conclusions
In conclusion, most minor bile leaks can be managed by ERCP and/or percutaneous drainage. However, bile leaks can lead to long hospital stays, because an early diagnosis is difficult when patients revisit the hospital within 7 days after the LC procedure. Therefore, although there may be very limited fluid collection in patients that revisit the ER with unusual abdominal pain after an LC, early ERCP should be considered to diagnose early bile leaks and decrease the length of needed hospital stay for further treatment.
Footnotes
Disclosure Statement
No competing financials interests exist.
This article was presented at the Semiannual Meeting of the Korean Association of Hepato-Biliary-Pancreatic Surgery in Seoul, Korea, November 13, 2008, and at the 21st Annual Meeting of the Japanese Society of Hepatobiliary and Pancreatic Surgery, June 11, 2009.