
Abstract
Abstract
Introduction:
Transduodenal ampullectomy (TDA) can be performed for benign and premalignant tumors of the ampulla of Vater (AOV) as an alternative to pancreaticoduodenectomy. However, the laparoscopic approach has rarely been attempted. In this report 2 cases of benign ampullary tumor that were treated by totally laparoscopic TDA.
Patients and Methods:
Case 1 was of a 75-year-old female who was admitted with left knee pain and underwent arthroscopic debridement. On postoperative day 6, she showed elevated levels of alkaline phosphatase, aspirate aminotransferase, alanine transaminase, and gamma-glutamyl transpeptidase, without any other laboratory test abnormality. She had no complaint of abdominal pain, and physical examinations were unremarkable. Computed tomography (CT), magnetic resonance cholangiography (MRCP), and endoscopy revealed a 2-cm-sized polypoid mass at the AOV. Subsequent endoscopic biopsy showed a pathologic finding of tubular adenoma. Case 2 was of a 55-year-old man who was admitted with an duodenal mass incidentally detected by screening endoscopy in a community hospital. Abdominal CT, endoscopy, and endoscopic ultrasonography revealed a 2.5-cm-sized tumor located at the duodenal papilla with possible extension to the ampullary sphincter. Endoscopic biopsy revealed gangliocytic paraganglioma. Both patients underwent laparoscopic transduodenal ampullectomy.
Results:
Operative times were 200 and 250 minutes, respectively, and estimated blood loss during both operations was about 50 mL. Patients were discharged on the postoperative days 9 and 8, respectively, without any complication. Postoperative histologic examinations revealed tubular adenoma with low-grade dysplasia in 1 patient and gangliocystic paraganglioma in the other.
Conclusions:
These 2 cases demonstrate that laparoscopic TDA is a feasible operative procedure in selective patients with a benign or premalignant tumor at the AOV.
Introduction
Case Reports
Patients
Case 1
A 75-year-old female with a medical history of hypertension and diabetes mellitus was admitted to our orthopedics department because of left knee pain and, subsequently, underwent arthroscopic debridement for degenerative arthritis. On postoperative day 6, laboratory findings showed elevated alkaline phosphatase (352 IU/L), aspirate aminotransferase (350 IU/L), alanine transaminase (142 IU/L), and gamma-glutamyl-transpeptidase (134 IU/L) levels. Other laboratory findings, including bilirubin and white blood cell count, were within normal limits. She had no abdominal pain and physical examinations were unremarkable. An ultrasonography showed common bile duct dilatation (diameter, 1.5 cm) with a mass lesion in the AOV. On computed tomography (CT) and magnetic resonance cholangiography (MRCP) images, a 2-cm-sized mass with contrast enhancement was observed at the AOV and a cut-off sign at the distal common bile duct (CBD) with mild upstream bile duct dilatation. On endoscopy, a 2-cm-sized polypoid mass was found at the AOV, and the pathologic report of the endoscopic biopsy performed showed tubular adenoma. Endoscopic papillectomy was not performed due to the possibility of CBD involvement. The patient was referred to our department for an operation, and laparoscopic transduodenal ampullectomy was performed.
Case 2
A 55-year-old man was admitted due to an incidental finding of a tumor in the duodenum by screening gastroduodenoscopy in a community hospital. He was a chronic hepatitis B carrier but had no other specific diseases. On physical examination, his abdomen was soft and not tender without a palpable mass, and his laboratory findings were within normal limits. Abdominal CT demonstrated a 2-cm-sized well-defined tumor located at the AOV. Endoscopic ultrasonography (EUS) revealed a 2.5-cm-sized tumor at the AOV with possible extension to the submucosa and ampullary sphincter. The pathologic report of the endoscopic biopsy indicated gangliocytic paraganglioma, and the patient underwent laparoscopic TDA.
Operative technique
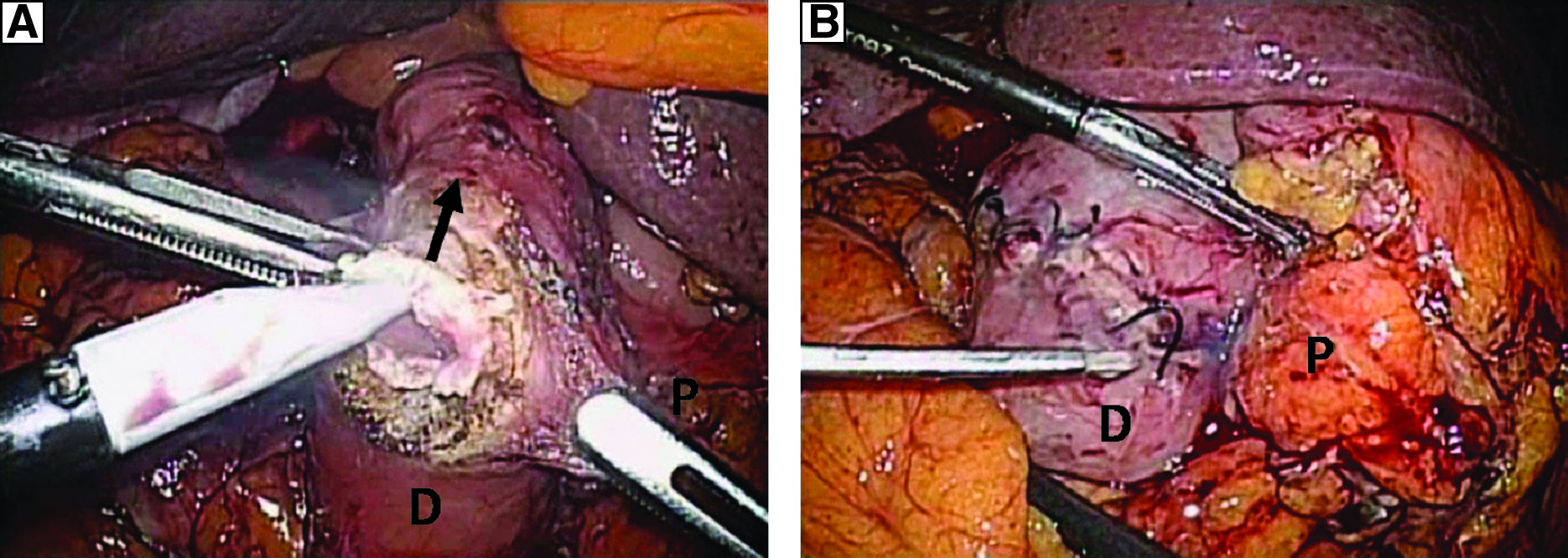
Under general anesthesia with the patient in the supine position and the surgeon standing on the patient's right side, a 12-mm umbilical port was inserted, and the pneumoperitoneum established by carbon-dioxide (CO2) insufflation; intra-abdominal pressure was maintained below 12 mm Hg. A flexible laparoscope (Olympus, Tokyo, Japan) was used, and an additional three ports (two 5-mm and one 10-mm) were inserted, as shown in Figure 1. After mobilizing the duodenum by using the Kocher maneuver, intraoperative ultrasonography was performed to locate the lesion site. After locating the tumor, a longitudinal duodenotomy of approximately 4 cm was performed on the antemesenteric side of the duodenum, just opposite the tumor (Fig. 2A). The AOV and the mass were identified (Fig. 3), and the presumed resection margin of the ampullectomy was marked by monopolar electrocautery. Ampullectomy was performed by using an ultrasonic shears and by electrocautery. Briefly, while grasping the duodenal mucosa 1 cm from the caudal side of the tumor, the duodenal mucosa and submucosa were resected inferior to superior. When the pancreatic duct was identified, it was cut sharply with care to ensure an adequate margin. Dissection was continued cephalad, and then the CBD was encountered and identified. After cutting the CBD, resection was completed while maintaining a proper margin. The cut end of the proximal bile duct and pancreatic duct were visualized within the resected area on the duodenal wall. The specimen was inserted into a vinyl bag and extracted through the wound at the umbilical port. It was then sent to a pathologist together with tumor orientation details. Frozen-section examinations revealed bile duct and pancreatic duct and lateral margins without any tumor involvement. Biliary and pancreatic ducts were sutured together into one common lumen, and then the conjoined lumen of the pancreatic and common bile ducts was sutured to the surrounding duodenal mucosa with Vicryl 4-0 (Ethicon, Sommerville, NJ) interrupted intracorporeal sutures (Fig. 4). The duodenotomy incision was then closed transversely with two-layer sutures (Fig. 2B). After inserting a drain tube, port-site wounds were closed in the usual manner.
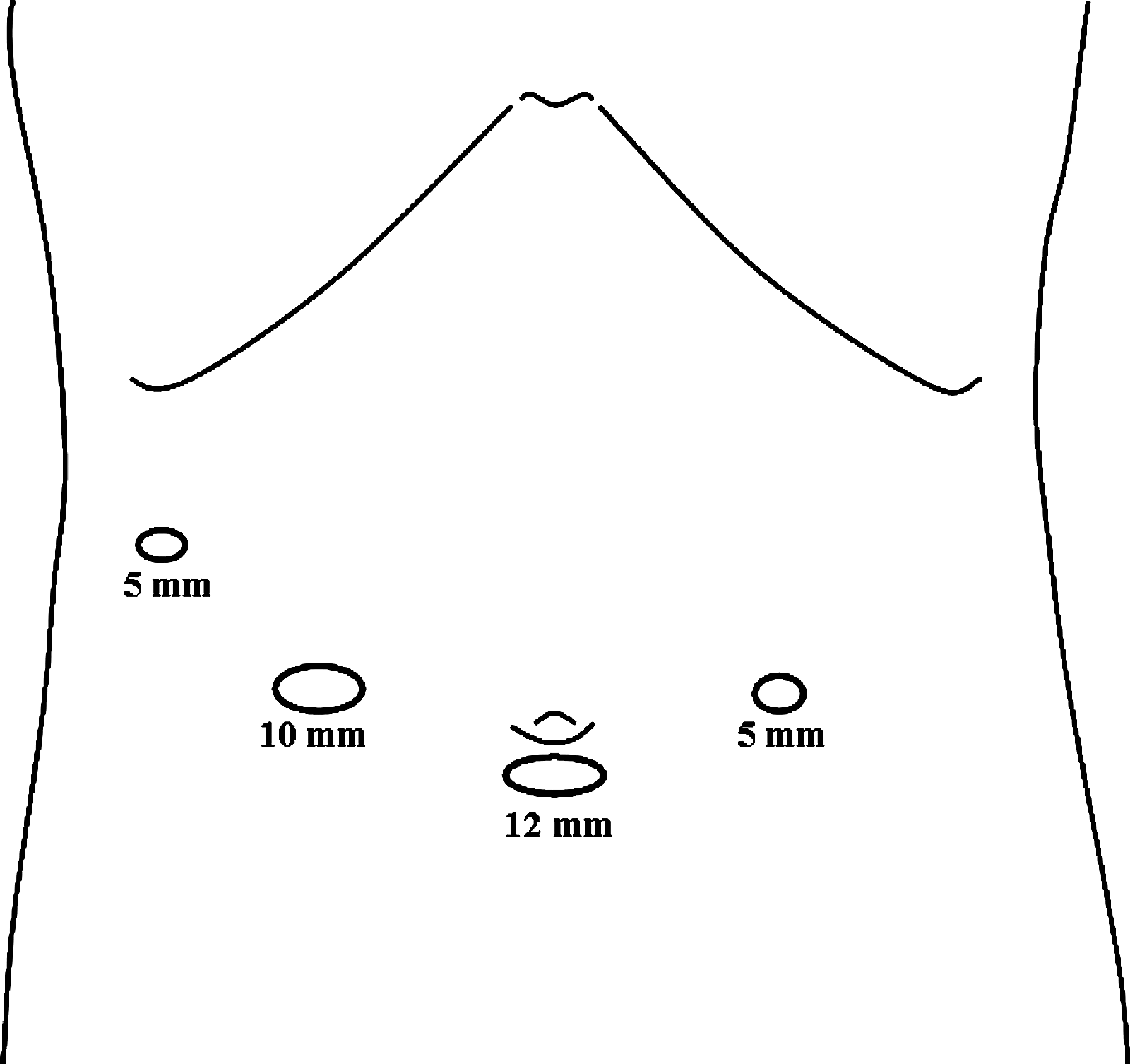
Trocar positions.
(
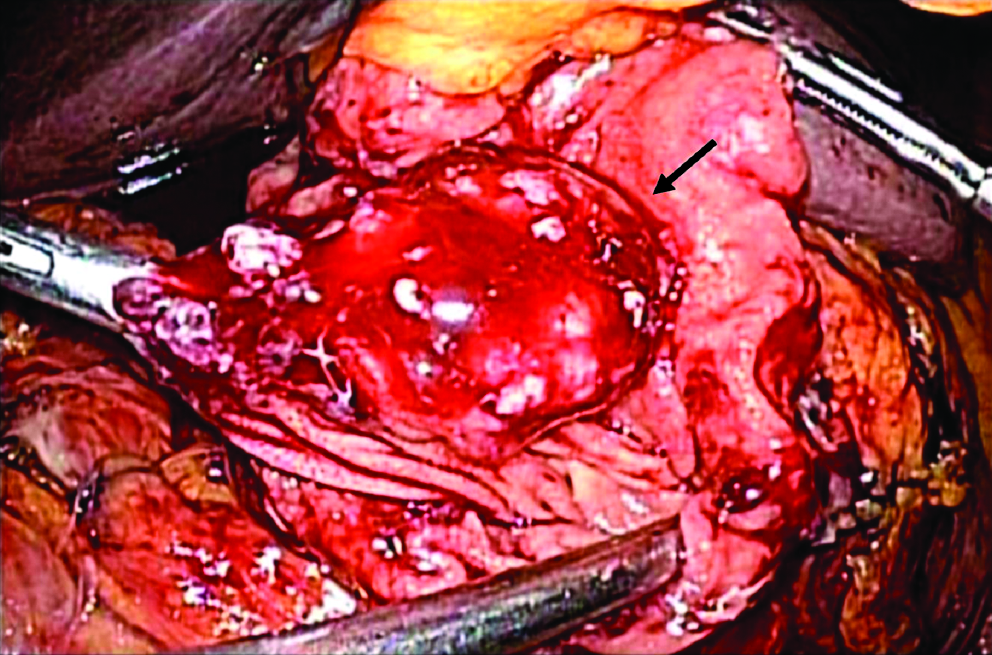
Intraoperative finding of the AOV mass in patient 1 (arrow indicates AOV mass).
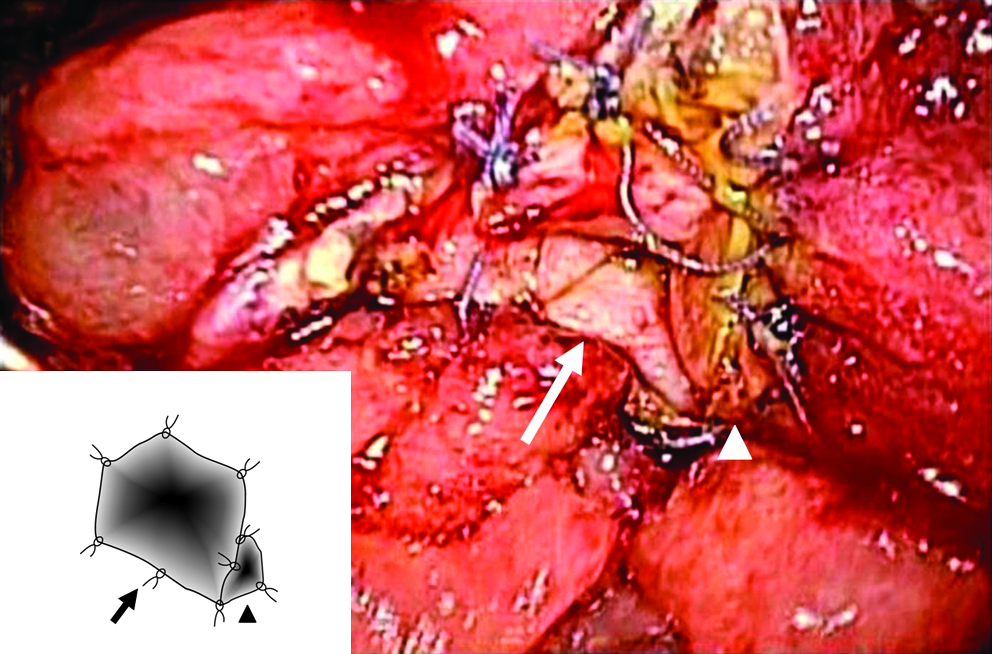
Intraoperative finding of patient 1 after anastomosis of the bile (arrow) and pancreatic (arrowhead) ducts.
Postoperative outcome
Case 1
The operative time was 200 minutes, and estimated intraoperative blood loss was ∼50 mL. On postoperative day 6, an upper gastrointestinal (GI) series with gastrograffin showed no leakage or passage disturbance. The patient was discharged on postoperative day 9 without any postoperative complication. Postoperative histology showed a tubular adenoma with low-grade dysplasia confined to the mucosa of ampulla. The tumor size was 2 × 1 × 0.2 cm with clear ductal and lateral resection margins of 0.5 cm (Fig. 5).

Postoperative specimen of the Patient 1. (
Case 2
The operative time was 250 minutes, and estimated intraoperative blood loss was ∼50 mL. On postoperative day 6, an upper GI series with gastrograffin showed no leakage or stricture. The patient was discharged on postoperative day 8 without any postoperative complication. Postoperative histology showed a 1.0 × 0.9 × 0.7 cm gangliocystic paraganglioma confined to the mucosa, submucosa, and ampullary sphincter with a clear resection margin of 0.4 cm.
Discussion
Operative treatments for ampullary tumor vary from local resection to PD. Although ampullary adenoma is considered benign, it is a premalignant disease and can harbor foci of coexistent carcinoma. 12 Further, a preoperative diagnosis of a benign character can be misleading, because reported false-negative rates of endoscopic biopsies range from 25 to 60%.4,13–15 Occasionally, ampullary adenoma can recur as invasive adenocarcinoma after local excision.4,16 Therefore, some researchers advocate radical resection even for benign ampullary tumor.14,17 In contrast, several reports have been issued on the safe application of local resection in ampullary adenoma with low recurrence rate.4,18 Further, even after recurrence, it can be treated by reexcision or radical excision. 19
Endoscopic papillectomy also can be applied to benign or borderline ampullary tumors, but its application is subject to certain limitations. Endoscopic papillectomy can be applied to small (<2 cm) villous or tubulovillous adenomas of the papilla without ulceration that do not invade the duodenal muscularis or infiltrate into the pancreatic or bile ducts.9,10 If an adenoma of the papilla extends into the AOV beyond major papilla or the sphincter of Oddi, endoscopic resection is inadequate. TDA can be applied to larger, deeper lesions than endoscopic papillectomy and can be performed when ampullary adenoma extends into the AOV and further into the orifice of the main pancreatic or bile duct. 20 TDA can be also applied to adenoma of the papilla with high-grade dysplasia, large (>2 cm) villous or tubulovillous adenoma of the papilla, or adenoma with carcinoma in situ 9 and other benign tumor, such as gangliocytic paraganglioma.21,22 The application of TDA to early malignancy appears incongruent because even in small (<1 cm) Tis or T1 cancers, lymph node metastases and CBD or pancreatic duct mucosal involvement can be present. 23 However, there are some reports that TDA can be applied to selected patients with high operative risk.5,24
Obtaining adequate margins is important in terms of reducing the likelihood of recurrence. 25 Some reports have mentioned high recurrence rates even for benign tumors of the AOV after TDA,15,25,26 and adequate resection margins would undoubtedly reduce these recurrence rates. If a resection margin is involved, conversion to PD is necessary because villous or tubulovillous adenoma are premalignant neoplasms and often harbor occult foci of carcinoma.12,25 To ensure complete excision with an adequate margin, it is necessary to excise the ampulla and reconstruct the CBD and pancreatic duct orifices. 4 After tumor resection, gross and microscopic margins should be confirmed by frozen section. The careful selection of lesion of the AOV by adequate preoperative evaluation and the use of intraoperative frozen-section biopsy to assess grade of tumor differentiation and margin involvement ensures the acceptability of TDA. 25 Adenoma and gangliocytic paraganglioma of AOV can be recurred as invasive cancer, so regular follow-up after TDA for surveillance of recurrence is advocated.4,18,21,22 Although there are no standard surveillance strategies, endoscopic follow-up every 6 months for 2 years, then yearly for 3–5 additional years, is recommended. 4 If there is any evidence of recurrent dysplasia or carcinoma, PD should be considered. 4
Laparoscopy has been used for tumor staging in ampullary or distal bile duct tumor. 27 In this case series, laparoscopic excision of ampullary tumor was also proven beneficial. Laparoscopic TDA offers the advantages associated with minimally invasive techniques. 11 The major concerns regarding laparoscopic TDA are how to determine the location of the AOV and obtain an adequate resection margin. In laparoscopic TDA, tumor location can be identified by intraoperative ultrasonography. Resected specimens, including the bile and pancreatic ducts, should be forwarded for pathologist examination to confirm a free tumor margin. The most difficult aspect of laparoscopic TDA is the intracorporeal anastomosis of the bile and pancreatic ducts to the duodenal wall after ampullectomy. Although laparoscopic suturing is a challenging procedure, intracorporeal suturing can be aided by magnified visual field by laparoscopy.
Conclusions
In summary, these two cases demonstrate that laparoscopic TDA is a feasible operative procedure in patients with a benign periampullary tumor.
Footnotes
Disclosure Statement
No competing financial interests exist.