
Abstract
Abstract
An accessory spleen is present in about 10–30% of the population and, usually, does not cause symptoms. We present a case report of an unusual presentation of accessory spleen infarction, with a literature review. A 12-year old male presented with acute left-upper quadrant pain that slowly resolved. An ultrasound and computed tomography scan showed a 3.5 × 2.5 × 2 cm solid mass abutting and displacing the splenic flexure of the colon, with surrounding inflammatory changes. This was interpreted as a colonic duplication cyst, and the boy was treated with antibiotics and underwent elective laparoscopic exploration. It was removed laparoscopically without complication and, on pathologic examination, proved to be consistent with an infarcted accessory spleen. Less than two dozen similar cases of accessory spleen infarction have been reported in the literature, most presenting with acute abdominal pain. Preoperative diagnoses included appendicitis, ovarian torsion, neoplasm, and, in our case, colonic duplication. The natural course of infarcted accessory spleen would be to atrophy, but, even with advanced imaging techniques, it may be impossible to diagnose infarcted accessory spleen with enough confidence to avoid surgery.
Introduction
Case Presentation
A previously healthy 12-year-old boy presented to a community hospital with a 6-day history of colicky abdominal pain limited to the left-upper quadrant. This was followed by nausea, vomiting, and fever, leading to his admission. On physical examination, he had stable vital signs, fullness in the left-upper quadrant, and tenderness to deep palpation. Ultrasound and computed tomography (CT) examinations of the abdomen were obtained. Ultrasound demonstrated a round heterogenous mass measuring 3.5 × 2.8 × 2 cm in the left-upper abdomen, located adjacent to the splenic flexure of the colon. A CT scan described the mass with a density of 65 HU and with minimal surrounding edema (Fig. 1). Since it was closely related to the bowel, displacing it anteriorly and inferiorly, it was suggested as bowel duplication related to the splenic flexure.
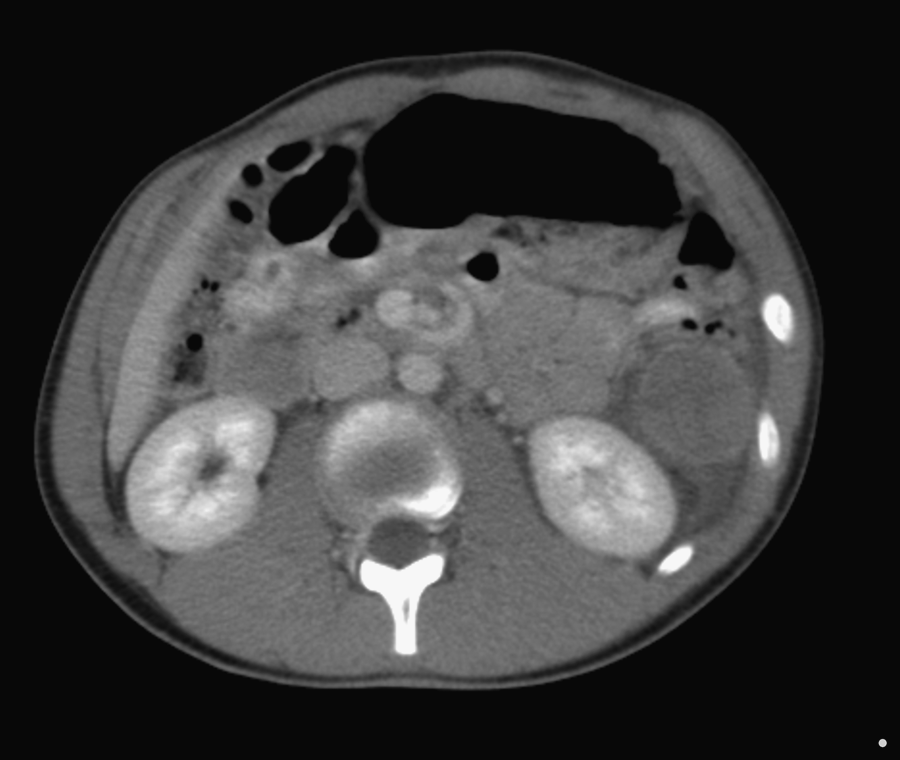
Axial computed tomography image of the left-upper quadrant mass with a density of 65 HU, indicating complex fluid with minimal surrounding edema.
The patient clinically improved, was discharged, and referred to the pediatric surgery outpatient clinic. He was scheduled for elective laparoscopic resection of the colonic duplication and was given oral antibiotics for 1 week. At laparoscopy, there was evidence of inflammation in the left-upper quadrant with flimsy adhesions to the anterior abdominal wall. The transverse colon was freed up and the mass was found to be completely separate from the colon (Fig. 2). It was freed up completely and removed by using minimal extension of the umbilical port. The recovery process was unremarkable. The mass was solid, measuring 3.5 × 2.5 × 2 cm, and the cut surface appeared reminiscent of the spleen. Histopathology showed that the nodule was completely infarcted beyond recognition, but with the aid of reticulin stain, the “skeleton” of sinusoids and vessels were well preserved and the report confirmed it was consistent with completely infarcted accessory spleen (Figs. 3 and 4). In retrospect, a small arterial branch originating from the splenic vessels was visualized on CT scan (Fig. 5).
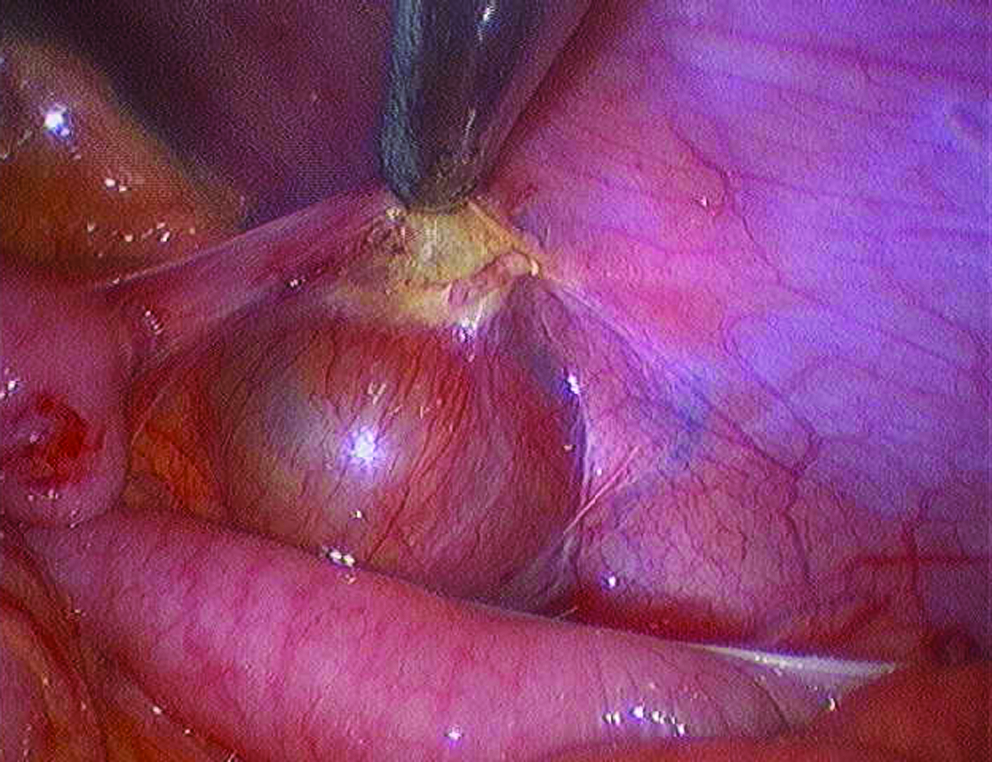
Laparoscopic image of retroperitoneal mass behind a splenic flexure of the colon, with surrounding inflammation.

Hematoxylin and eosin staining of specimen showing ghost cells consistent with infarcted tissue.
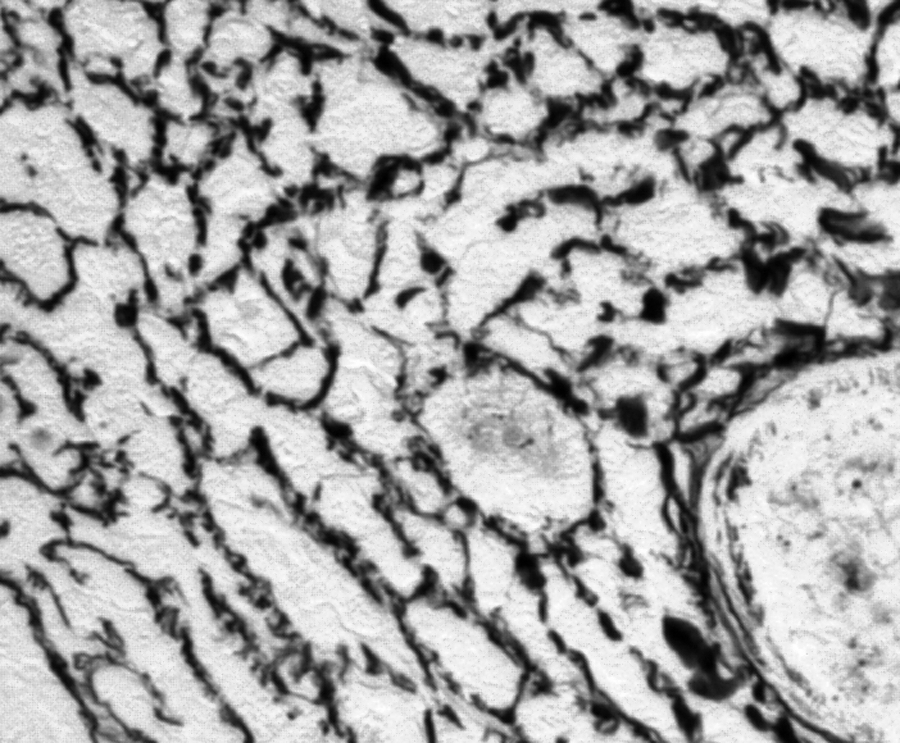
Reticulin staining showing preserved sinusoidal architecture, confirming accessory spleen structure.

In retrospect, a small arterial branch originating from the splenic vessels was visualized on the coronal computed tomography scan image (arrow). The mass (M, infarcted accessory spleen) is next to the splenic flexure of the colon.
Discussion
An accessory spleen is a relatively common condition, appearing in about 10–30% of autopsies. 1 They are mostly found in children, 2 since they tend to atrophy with age. 3 Accessory spleens are congenital foci of normal splenic tissue that are separate from the main body of the spleen. They are thought to be due to a failure of the fusion of splenic rests forming in the dorsal mesogastrium during development. Distant accessory spleens are thought to develop from primordial splenic buds that form in remote locations. 4
An accessory spleen is located in the hilum of the spleen in 75% of cases and in the tail of the pancreas in 20% of cases. 5 The remaining 5% of accessory spleens occur in the greater omentum, lienorenal or gastrosplenic ligaments, mesentery, jejunal wall, scrotum, and mediastinum. 6 The accessory spleen resembles a lymph node; the size varies from a few millimeters up to 1.5–2 cm and, usually, has no clinical significance. 7 However, if the location is atypical, an accessory spleen may be mistaken for a tumor. 8
Interestingly, after splenectomy, an accessory spleen may enlarge dramatically, sometimes appearing as a left-upper quadrant mass, causing a recurrence of problems in patients who have undergone splenectomy for hematologic disorders, 9 such as idiopathic thrombocytopenic purpura. 2 In those patients, it is important to try to identify an accessory spleen at the time of splenectomy. 8 If the disease recurs, it is important to test for the absence of residual splenic function by identifying Howell-Jolly bodies in a peripheral blood smear postsplenectomy. 9 CT is useful in the accurate diagnosis of an accessory spleen.7,8 It usually is seen as an ovoid or round mass with the same density of the normal spleen pre- and postcontrast. Scintigraphy, using 99mTc-sulphur colloid 9 or Tc-99m-phytate, 10 is used when it is imperative to identify an accessory spleen, such as a recurrence of idiopathic thrombocytopenic purpura after splenectomy.
Torsion of the accessory spleen with resultant infarction is extremely rare, with only 9 pediatric cases reported in the English literature from 1940 to 2001. The youngest patient in the literature was described by Gardikis et al. in a 14-day-old female infant. 4 The diagnosis was made at an emergency laparotomy done for signs of acute abdomen. The cause for the splenule necrosis was torsion of its pedicle. Several reports were described in the literature since then, increasing the total number to about 18 cases, 12 of which are pediatric.1,6,11,12,13 Most of the reported cases presented with acute abdominal signs and symptoms, and all went on to excision of the mass.
Wacha et al. reported the value of diagnostic laparoscopy in finding an accessory spleen; the laparoscopy was done for chronic lower abdominal pain. The pain resolved postresection of the pedunculated accessory spleen. 11 Grinbaum et al. reported a similar case in a 21-year-old female in 2006. 12 In our case, the preoperative diagnosis suggested a colonic duplication, on which we based our operative indication. The appearance of the mass on CT and ultrasound and close relation of the mass to the adjacent splenic flexure suggested the diagnosis of bowel duplication with complex cystic content. Duplication of the colon and rectum are found in 17% of all bowel duplications. However, cystic duplications are quite rare. They usually contain colonic mucosa and, possibly, ectopic gastric mucosa. Excision is the treatment of choice. 14 Other differential diagnoses arising in that anatomic location are lymphatic malformation with secondary infection, a neoplastic lymph node, or phlegmon/abscess due to inflammatory bowel disease. Had we known the diagnosis with any degree of confidence preoperatively, we might have chosen to treat the patient conservatively and follow him with serial imaging until the mass involuted, as suggested by Seo et al. 5 Involution or atrophy is the natural history of infarcted splenic tissue, as evident from our understanding of autosplenectomy happening in sickle-cell anemia patients.
Conclusion
A high index of suspicion and diligent interpretation of the imaging might prove to be the only way to entertain an accessory splenic infarction in the differential of a patient with acute abdominal signs.
Footnotes
Disclosure Statement
No competing financial interests exist.