
Abstract
Abstract
Vascular disturbances of the omentum, described variously as acute epiploitis, primary omental torsion, idiopathic segmental infarction, etc., is an infrequent cause of acute abdomen, often mimicking acute appendicitis, cholecystitis, or pancreatitis. In this retrospective article, we share our experiences about the incidence, diagnostic dilemma, and management of patients with omental torsion or infarction and discuss the diagnostic and therapeutic role of laparoscopy. From January 2003 to December 2008, 9 patients (7 men and 2 women; median age, 26 years; range, 5–71) with omental gangrene, including omental torsion and infarction, were operated on at our institute. Of these, 8 patients had a preoperative provisional diagnosis of acute appendicitis and 1 patient of acute calculus cholecystitis. During this period, a total of 1502 patients were diagnosed and operated on laparoscopically for acute appendicitis and acute cholecystitis. Of them, 2 patients were intraoperatively diagnosed to have omental torsion and 7 patients had segmental omental infarction. Incidences of omental gangrene presenting as acute cholecystitis and acute appendicitis were 0.11 and 1.1%, respectively. The suspected preoperative pathology was grossly normal, and histopathology of the same was noncontributory to the cause of acute abdomen. All 9 cases were managed laparoscopically, with the gangrenous omentum excised along with appendectomy in 8 patients and cholecystectomy in 1 patient. In conclusion, inspection of the omentum should be a routine part of exploration in suspected acute appendicitis.
Introduction
Materials and Methods
A retrospective review of medical records was done of all patients operated on by a single team of surgeons (headed by OT) for omental torsion or infarction at our institution during January 2003 to December 2008. The data, maintained on Microsoft Excel 2007 sheets (Redmond, WA), were retrieved from the headings of acute appendicitis, acute cholecystitis, omental torsion, omental infarction, and the clinical presentation, laboratory findings, diagnostic-imaging results, as well as operative findings and histology, were reviewed. The safety and efficacy of using laparoscopy in the diagnosis and treatment of omental torsion or infarction was assessed. Statistical analysis of variables are expressed as median, range, and proportions and Fisher's exact test, as indicated. A P-value of less than 0.05 was regarded as indicating a statistical difference.
Results
During the 6-year period, a total of 1502 patients were preoperatively diagnosed in our unit for acute appendicitis and acute cholecystitis in 628 and 874 patients, respectively, and taken up for laparoscopic surgery. The diagnosis was based on clinical, laboratory, and radiologic examination. But, on laparoscopy, 9 patients were intraoperatively diagnosed as having omental torsion or infarction, with an overall incidence of 0.6%. Of these, 8 patients were suspected preoperatively of having acute appendicitis and 1 patient of having acute calculus cholecystitis. The overall incidence of omental gangrene, found in suspected cases of acute cholecystitis, was 0.11% and in acute appendicitis was 1.1%. Seven patients (77.8%) were found to have had segmental omental infarction, and 2 patients (22.2%) had omental torsion. The suspected preoperative pathology was found to be grossly normal and noncontributory to the cause of pain, as later confirmed by histopathologic study.
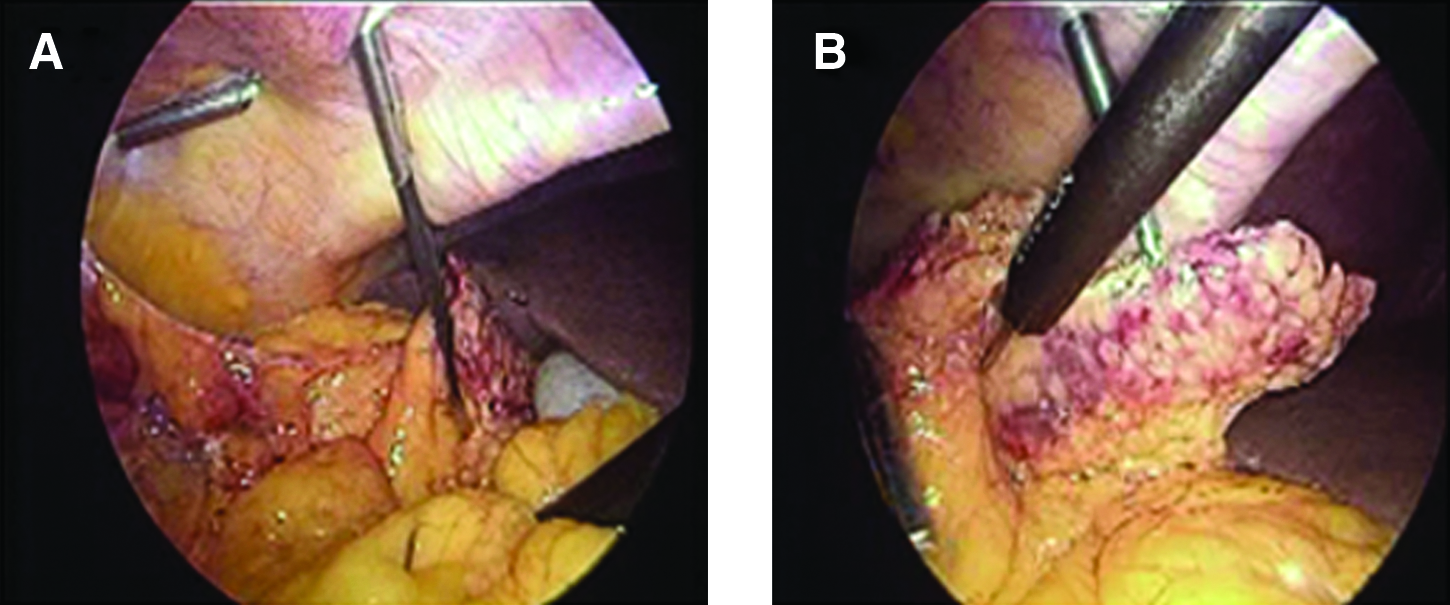
Demographic details, suspected preoperative pathology, and operative findings are shown in Table 1. The 9 cases of omental gangrene were found in 7 men and 2 women, with the median age of presentation at 26 years (range, 5–71). Two patients were in the pediatric age group, both presenting clinically as acute appendicitis, but intraoperatively were found to have segmental omental infarction (Fig. 1). Altogether, 3 (33.3%) patients had an obese build with a body mass index more than 30 (P = 0.43). None of the patients were suspected to have omental gangrene on preoperative investigations. The USG findings in all patients had shown free fluid in the abdomen, while 1 patient had an additional finding of gallstones. The 2 patients with omental torsion had a previous history of blunt trauma abdomen, but the latter required no specific treatment. All patients had an elevated leucocyte count (11,000–13,500 cells/mm3) with significant neutrophilia.

Segmental omental infarction with gangrene.
S/N, series number; BMI, body mass index; F, female; M, male; Lap, laparoscopic.
It was during the laparoscopic evaluation only that the finding of segmental ischemia or twisted mass of omentum in the right side of the abdomen was made accurately. There was the presence of serosanguinous free fluid in the peritoneal cavity in all cases. Both cases of omental torsion were secondary to adhesion of the omentum to the anterior abdominal wall (Fig. 2). Excision of the gangrenous omentum was done in all the cases. The appendix was removed in all 8 patients who were diagnosed preoperatively as having acute appendicitis in order to avoid future diagnostic dilemma. Cholecystectomy was done in the only patient with gallstones diagnosed preoperatively (Fig. 3). The histologic examination of the specimens revealed hemorrhagic ischemic necrosis of the omentum and a normal appendix. The gallbladder that was removed had histopathologic evidence of chronic calculus cholecystitis. There were no postoperative complications, and the follow-up, in majority of the patients, to 1 year was uneventful.

Omental torsion secondary to adhesion.
(
Discussion
Vascular disturbances of the greater omentum, although an infrequent entity, are frequently misdiagnosed as acute appendicitis 1 or acute cholecystitis. Various descriptive titles are given in the literature for this condition, including primary omental torsion, omental volvulus, acute epiploitis, idiopathic segmental infarction, and omental thrombosis.2–4 Although several attempts at classification have been made,5–7 however, the most satisfactory is that of Leitner et al., who had classified the entity basically into two groups 7 : omental infarction due to torsion and thrombosis.
Primary idiopathic torsion of the omentum, first described in 1899 by Eittel, is an infrequent cause of acute abdomen. 8 Torsion of the omentum results when the greater omentum twists upon itself along its long axis, with the resultant compromise of its vascular supply. 9 It may be classified as primary or secondary. Primary torsion is said to occur when no pathologic cause is found. Secondary torsion is associated with other intra-abdominal pathologies, which include omental cysts, adhesions, hernias, or tumors. Secondary torsion is more common than primary.9–11 We had 2 patients with omental torsion secondary to omental adhesion, mimicking acute appendicitis clinically. The identified precipitating factors for primary torsion of the omentum include local trauma, overeating with resultant hyperperistalsis (this induces omental displacement), sudden change in position, coughing, and straining.9,12,13 Both our patients with omental torsion had a previous history of blunt abdominal trauma.
Primary omental torsion is more common in adults, with only 15% of cases occurring in the pediatric age group. 10 Most patients are middle aged with a male preponderance.9,14 None of our patients with omental torsion were in the pediatric age group. The right side of the omentum is the most frequently involved portion, which is believed to be due to its increased length and mobility.14–17 The patient population for primary omental torsion is usually obese.9,12,13 In our study, 1 patient with omental torsion was obese, and altogether, 3 patients with omental gangrene were in the obese group. But, the number of patients in the study group was too few for us to comment on the significance of obesity as a risk factor for primary omental torsion.
The other entity, idiopathic segmental infarction of the greater omentum, is a rare cause of acute abdominal pain, which was first described by Bush in 1896. 18 It is a disease of unknown etiology, and the right side of the omentum is involved in 90% of cases, mimicking acute appendicitis in the majority. 19 The reported incidence is 0.1% of the total laparotomies performed for acute abdomen. 20 The clinical picture simulates appendicitis, diverticulitis, or cholecystitis, depending on the site of infarction. 21 It may be rarely associated with acute appendicitis simultaneously, as reported by Battaglia et al. 22 We had the preoperative impression of acute appendicitis in 6 cases of omental infarction. One patient was diagnosed with acute calculus cholecystitis, but on operation, was found to have omental infarction without acute inflammation of the gallbladder wall, as confirmed later by histopathology.
The exact etiopathogenesis of idiopathic segmental infarction is not known. Some researchers have suggested that a congenitally anomalous fragile blood supply to the right-lower portion of the greater omentum renders this region prone to infarction. 23 Such a theory could explain the high incidence (90%) of this disease in the right side of the greater omentum. Other researchers have suggested venous engorgement after heavy meals or venous elongation produced by excessive weight of the greater omentum as a cause, since there is a higher prevalence of the syndrome in the obese population. 24 In a recent collective review of 19 cases, 25 of the idiopathic type from the last 20 years, 42% of the cases occurred in pediatric patients and female patients were affected only in 15% of the cases. We had 2 patients from the pediatric age group (28.6%) and 1 female (14.3%), who presented with segmental omental infarction.
The most frequent complaint in both conditions is pain in the right iliac fossa, which is sudden in onset and, at times, may be associated with nausea, vomiting, and low-grade fever. A past history of a similar, but less severe, pain may be present. Physical examination usually elicits localized tenderness with or without a palpable “mass.” Temperature is usually normal or slightly raised. Occasionally, the white blood cell count may be elevated. Therefore, clinically, omental torsion or infarction is difficult to distinguish from appendicitis, cholecystitis, or pelvic adnexal diseases. Goti et al. stated that 66% of these cases mimic appendicitis, and 22% cholecystitis. 26 We had 88.9% of the cases mimicking acute appendicitis and 11.1% misinterpreted as acute calculus cholecystitis in our study.
Diagnostic imaging with USG and CT scan can be useful for diagnosis, but is not very reliable. USG may show a complex mass and mixture of solid material and hypoechoic zones and free fluid within the peritoneal cavity. On the other hand, the CT scan is very sensitive for showing an omental mass, but not specific for making a diagnosis of torsion or infarction. The finding of a vascular pedicle extending from the periphery of the mass to the inferior border of the stomach ventral to the colon may help differentiate torsion of the omentum from other fatty tumors.27–29 Use of CT scans in general reduces the rate of negative appendectomy, but does not appear to be efficacious in males. 30 With the increased use of CT in assisting in the diagnosis of questionable appendicitis, omental torsion may be diagnosed more often radiologically. We had no case detected preoperatively by ultrasound. We did not have CT scans advised in any of the patients because of economic factors, nor was it expected to have changed the overall management. The treatment of this condition, if diagnosed preoperatively, can be conservative and expectant in stable patients. 31 This includes reassurance, analgesics, and antibiotics, and resolution is expected in 2 weeks.
As discussed previously, most of these patients usually mimic acute appendicitis. However, the presence of serosanguinous fluid and a normal appendix should encourage exploration of the omentum. The serosanguinous fluid is almost a universal finding.32,33 We had also found serosanguinous fluid in the peritoneal cavity in all the patients during laparoscopic evaluation. The diagnosis is likely to be missed in open surgery, as the examination can be difficult through a McBurney, or any infraumbilical, incision used for conventional appendectomy. With the advent of laparoscopy and its widespread use, omental torsion or infarction is being visualized easily, and the chances of missing the pathology at surgery are now rare. We had all our cases detected during laparoscopic evaluation while searching the peritoneal cavity. Hence, laparoscopy is probably the best method of diagnosis, therapy, and to shorten the course of this disease.
Treatment involves excision of the diseased segment of the omentum and to correct any secondary pathology, if present. Either by open surgery or laparoscopy, the rationale for excision rests on the theoretic possibility of adhesion formation about the infarct, which could obstruct adjacent bowel loops. It has been observed that if the omentum is not excised, it may become atrophic and fibrotic, and, on rare occasions, the pedicle may even autoamputate, leading to automatic clinical regression. 34 Also, at times, in case of an untreated situation, one may see omental necrosis because of hemorrhagic infarction, intra-abdominal abscesses, peritonitis, or bowel obstruction.35,36 Spontaneous derotation may be possible and may explain omental adhesions found during laparotomy that have no clear cause. We performed laparoscopic segmental omental resection along with appendectomy in all our cases in order to avoid a future diagnostic dilemma. The only case with gallstones and omental infarction underwent cholecystectomy along with segmental omental resection.
Conclusions
Omental torsion or segmental omental infarction of the greater omentum is a rare cause of acute abdomen predominantly with right-sided signs. It should be emphasized to include this vascular disorder of the greater omentum in the differential diagnosis of any patient with acute appendicitis. Inspection of the omentum should be a routine part of exploration when a more common cause of abdominal complaint is not readily obvious at operation. Although CT scans may be useful in diagnosis, they do not alter the therapeutic plan. The performance of laparoscopy as a minimally invasive surgery can be useful for both diagnosis and treatment of this uncommon condition. With the popularity of minimal access surgery increasing, more cases are being documented and reported. We would like to emphasize the usefulness of laparoscopy in patients with right-lower quadrant pain, which is both diagnostic as well as therapeutic.
Footnotes
Disclosure Statement
No competing financial interests exist.