
Abstract
Abstract
The unique technique of ventral hilum exposure (VHE) was reported that it had excellent surgical outcomes in patients with intrahepatic bile duct stone. The basis of this surgical technique is that all the openings of the 2nd-order bile duct branches are exposed fully. In this article, we describe laparoscopic hemihepatectomy from using the VHE method in a patient with intrahepatic bile duct stone. Our patient was a 70-year-old female who had been diagnosed with an intrahepatic duct stone 30 years prior. Multiple intrahepatic bile duct stones in the left lateral section of the liver were revealed by abdominal computed tomography and magnetic resonance cholangiopancreatography. The patient resumed her oral intake on postoperative day 6. The patient had hyperbilirubinemia (10.3 mg/100 mL) on postoperative day 10. However, her serum bilirubin level decreased to 2.7 mg/100 mL on postoperative day 28. She was discharged without any serious complications on postoperative day 31. Totally laparoscopic left hemihepatectomy, using the VHE method, can be one option of surgical procedure in the near future, although a larger series of cases should be necessary to prove the feasibility of laparoscopic VHE.
Introduction
Surgery can produce favorable outcomes for the treatment of intrahepatic duct stones. In particular, excellent surgical outcomes have been reported when using the VHE method in patients with intrahepatic duct stones. 9 The fundamental principle of VHE is that all openings of the 2nd-order bile duct branches are exposed fully by biliotomy after dissection along the precaudate plane (Fig. 1). Laparoscopic hepatectomy is a new procedure for liver lesions, and is a minimally invasive approach. Many cases of liver disease have been operated on by laparoscopic, instead of open, surgery.10,11 In this article, we present the technique of totally laparoscopic hemihepatectomy in using the VHE method for the first time and then discuss our results for a patient with an intrahepatic bile duct stone.
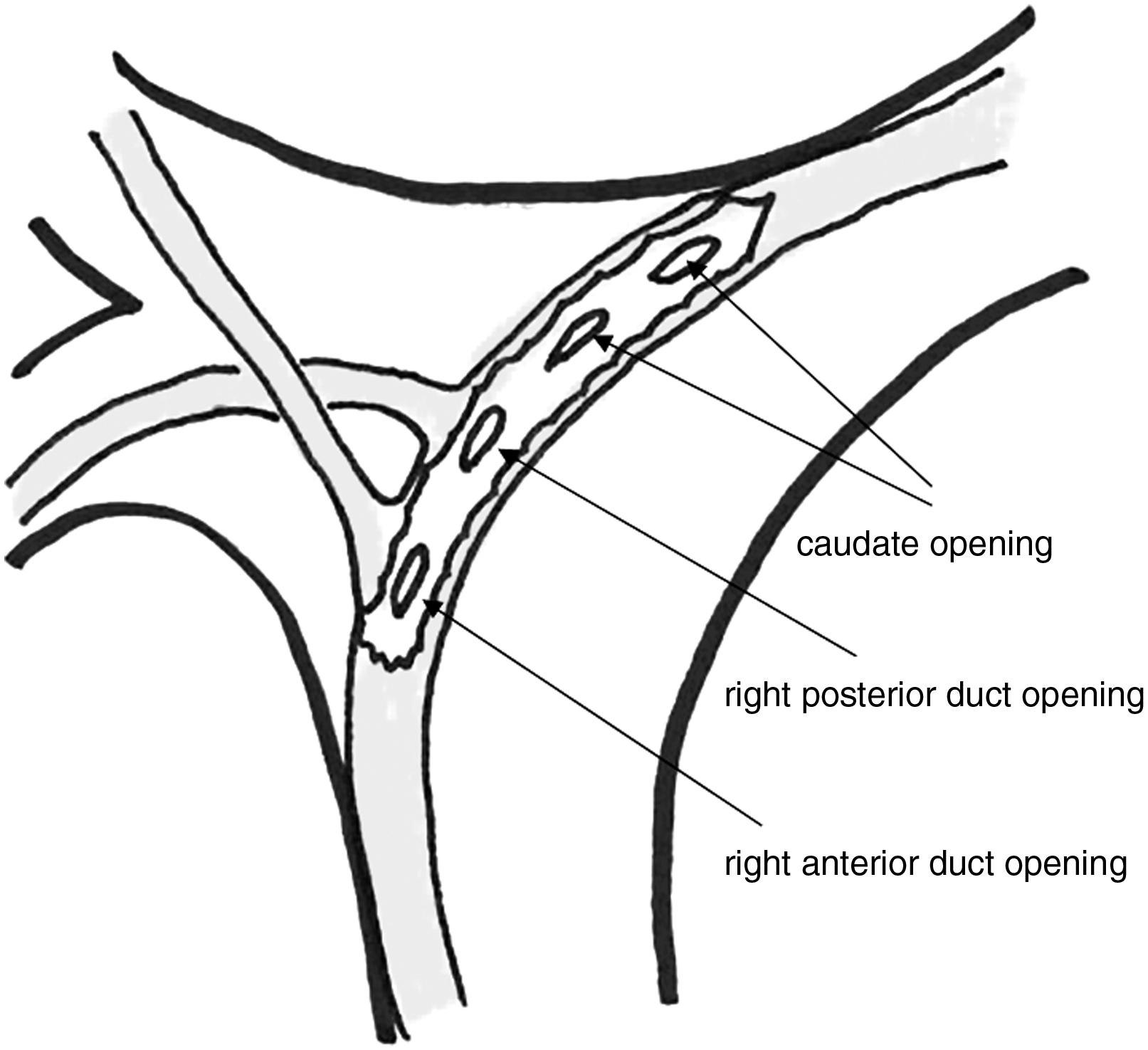
Schematic drawing of the ventral hilum exposure (VHE) method during left hemihepatectomy. The ventral portion of the hilar bile duct is opened along its direction.
Case Report
Our patient was a 70-year-old female who was admitted due to abdominal pain and general weakness for 1 month. She was transferred from the local general hospital. She had been diagnosed with an intrahepatic duct stone 30 years prior and had been admitted to the hospital on several occasions for abdominal and back pain. She had essential hypertension. An abdominal computed tomography (CT) scan and magnetic resonance cholangiopancreatography (MRCP) showed multiple intrahepatic duct stones at the left lateral section of the liver and a 4-cm common bile duct stone (Fig. 2).
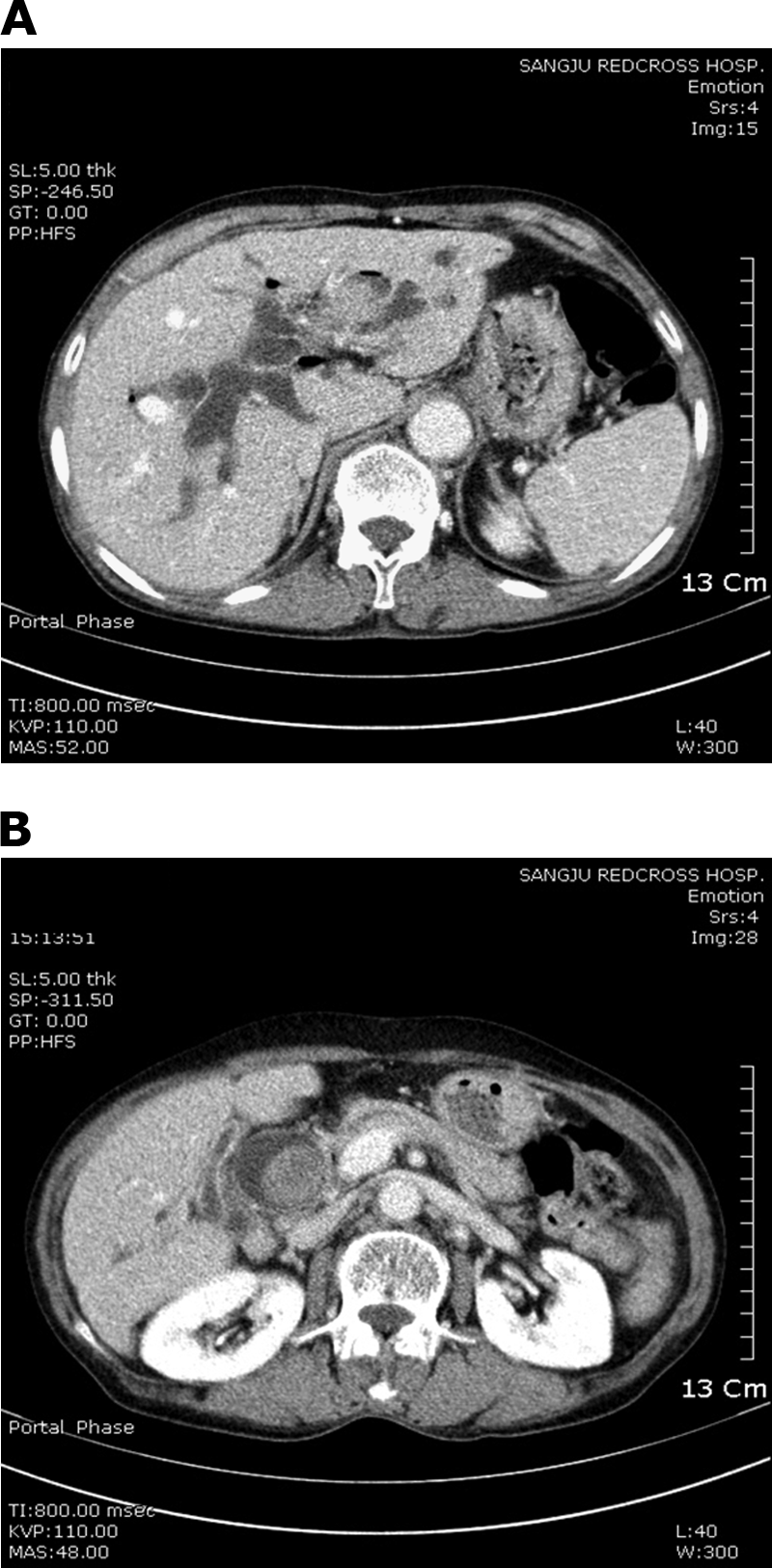
Preoperative abdominal computed tomography findings. (
Five punctures were made in the umbilical area, left midclavicular line, xyphoid, right midclavicular line, and right axillary line. All ports were 12 mm in size. Central venous pressure was maintained at 5–10 mmHg and kept above 8 mm Hg during the hepatic parenchymal dissection to protect against air embolism. Severe adhesion of the stomach, diaphragm, and colon was noted at the perihepatic area. The Pringle maneuver was performed three times through the trocar of the left midclavicular line with a 15-minute clamp and 5-minute release. Adhesiolysis was performed and the liver was mobilized. In laparoscopic VHE, in contrast to open-surgery VHE, the liver parenchyma along Cantlie's line does not need to be dissected, which we considered, at the time, to be one of the advantages of laparoscopic surgery. A biliotomy was performed at the bifurcation. All 2nd-order bile duct openings were identified by direct vision (Fig. 3). The dilated opening of the 3rd caudate branch was noted. The bile duct was divided just left of the opening of the 3rd caudate branch. A cholecystectomy was then performed. The left portal vein and left hepatic artery were isolated and ligated, respectively. Further hepatic parenchymal dissection was made with a Cavitron Ultrasonic Surgical Aspirator (CUSA™; Integra Lifesciences Corp., Plainsboro, NJ). The left hepatic vein was then ligated, and the resected specimen was delivered out thorough a newly made Pfannenstiel incision, using an endobag. A T-tube was then placed in the bile duct (Fig. 4). The previously opened bile duct was approximated intracorporeally by interrupted sutures, using 4-0 Vicryl. Two Jackson-Pratt drains were placed in the subhepatic space. The total operation time was 14 hours and 35 minutes. Blood loss and blood transfusion were 2500 and 1250 mL, respectively. She was sent to the intensive care unit after the operation.
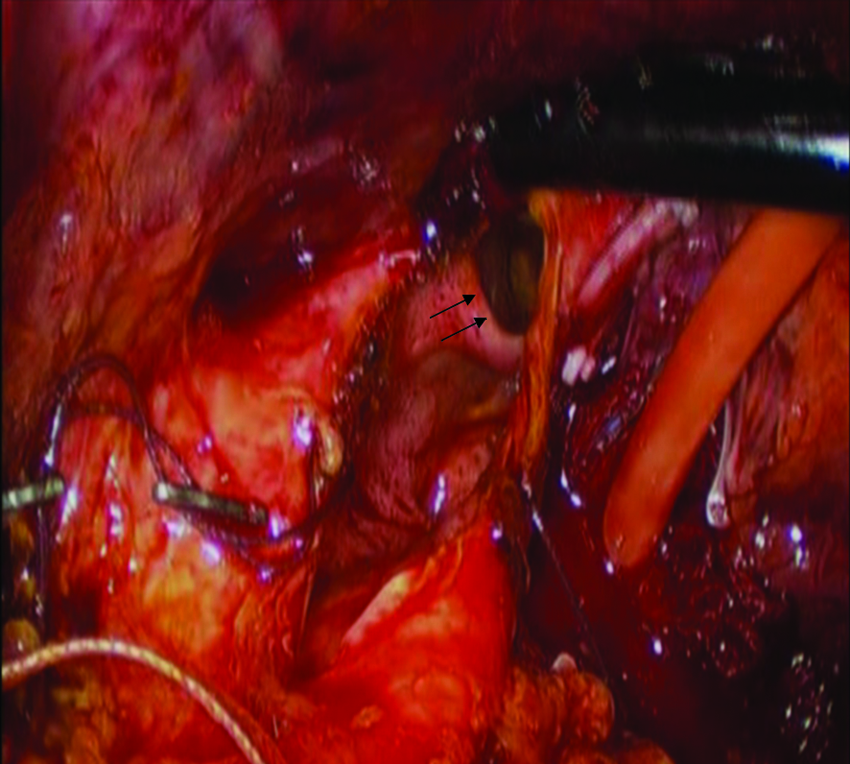
Laparoscopic view of the ventral portion of the hilar bile duct. Arrows (→) show the dilated opening of the 3rd caudate branch.
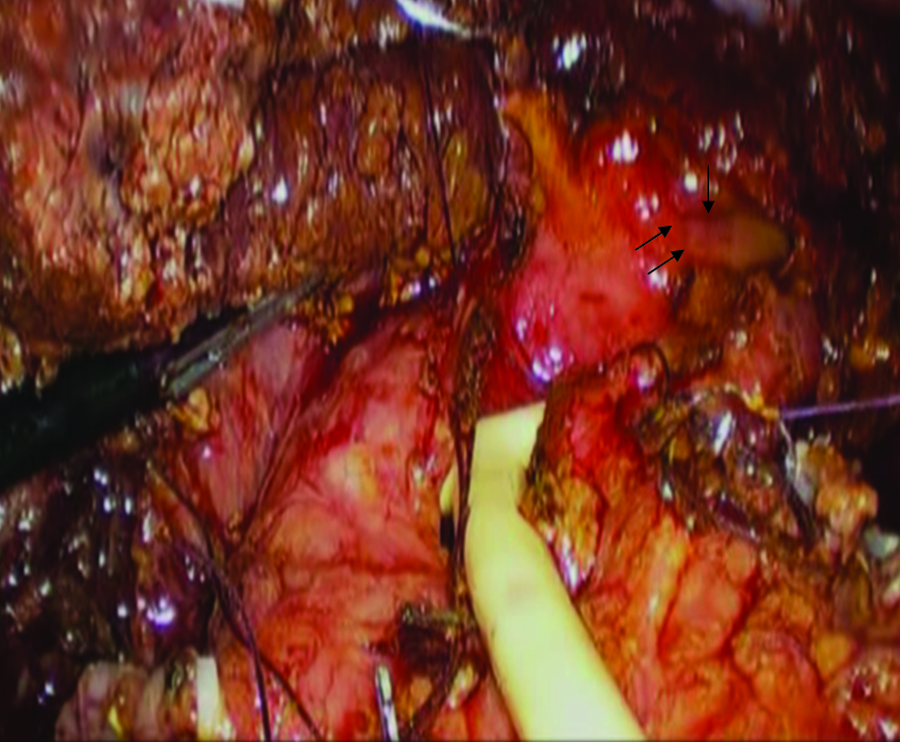
Lararoscopic view of the T-tube insertion after bile duct division and hepatic parenchymal dissection. Arrows (→) show the opening of the 3rd caudate branch.
The patient was transferred to the general ward on postoperative day 5. She resumed her oral intake on postoperative day 6. She had no complications, such as bile leakage. Laboratory tests showed hyperbilirubinemia of 10.2 mg/100 mL on postoperative day 8, of which we were concerned might be a sign of hepatic failure. However, her serum bilirubin level was 2.7 mg/100 mL on postoperative day 28. The patient was going to be disacharged on postoperative day 20, but she was discharged on postoperative day 31 due to her personal financial difficulties. Pathology results confirmed the diagnosis of benign hepatolithiasis.
Discussion
Kim et al. 9 first described the VHE method. The goal of VHE is total exposure of the hilar bile duct. A sagittal liver parenchymal dissection along Cantlie's line is made until the right hilar Glisson's pedicle is reached. Then, the sagittal dissection plane is rotated 90 degrees to the left along the coronal or precaudate plane. Generally, the hilar bile duct is situated at the extreme anterosuperior aspect in the hilar Glissson's pedicle. This can be confirmed by needle-puncture aspiration of bile, and the anterior wall of the hilar bile duct can then be opened safely along its direction without hilar Glisson's sheath dissection. In this way, the openings of the 2nd-order branches of the intrahepatic bile duct can be visualized, allowing a precise evaluation of the distribution of intrahepatic stones and the hilar stricture (Fig. 1). The VHE method is used primarily for high-grade Tsunoda type III and IV stones, that is, left and/or right intrahepatic duct stones with stricture.9,12
The VHE method is based on anatomy, as follows.13,14 The precaudate plane is defined by two anatomic landmarks, which are the ventral margin of the ligamentum venosum and the ventral margin of the hilar plate. VHE is a safe surgical procedure and results in favorable outcomes when used to treat hepatolithiasis. This procedure has the advantage that the intrahepatic bile duct stricture can be confirmed and corrected directly during surgery. Some anatomic variation, such as origin of the right posterior or anterior bile duct branch from the left main bile duct, can be overcome safely, because all bile duct openings can be visualized directly from using the VHE method.
Regardless of whether open or laparoscopic surgery is performed, the conventional hilar approach in left hemihepatectomy involves dissection of the portal pedicle outside the liver parenchyma with separate ligation of the left hepatic artery, portal vein, and bile duct. Generally, the conventional hilar approach and VHE method have similar operative risks and outcomes. However, in complicated hepatolithiasis cases or patients with severe inflammation, dissection of the hilar bile duct from the hepatic artery and portal vein can be difficult to perform, and it may also be challenging to differentiate between the multiple branches of the caudate lobe and the IV segment. We strongly suggest that left hemihepatectomy when using the VHE method is superior to the conventional hilar dissection in these cases. Additionally, although we did not perform hepatic parenchymal dissection before opening the hilar bile duct in this case, we believe that hepatic parenchymal dissection before VHE would have made for a facilitated management of the bile duct.
The focus of this report is not the clinical course compared with open surgery. We think many physicians do not agree to accept laparoscopic VHE as one option of a surgical technique because of the long operation time and significant blood loss in this patient. We do not insist on the feasibility of laparoscopic VHE only with this case. A larger series of cases should be necessary to prove the feasibility of this procedure. More experience of laparoscopic VHE can make operation time and blood loss decrease, similar to a lot of other laparoscopic procedures in the recent laparoscopic era.
Conclusions
Totally laparoscopic left hemihepatectomy when using the VHE method can be one option of surgical procedure in the near future, although a larger series of cases should be necessary to prove the feasibility of laparoscopic VHE.
Footnotes
Disclosure Statement
No competing financial interests exist.