
Abstract
Abstract
Objectives:
Laparoscopic pyeloplasty and ureteric reimplantation are complex urologic operations requiring delicate surgical skill. The use of a robot may provide benefits in performing these reconstructive operations. In this article, we report our early experience in the use of the robot in pediatric urologic operations.
Methods:
Children who underwent robotic-assisted reconstructive urologic operations were reviewed and analyzed.
Results:
From November 2005 to April 2008, 8 children underwent robotic-assisted reconstructive urologic operations. Three children had extravesical ureteral reimplantation performed for vesicoureteric reflux (VUR), and 5 children had pyeloplasty performed for pelvic-ureteric junction obstruction. There was no conversion to open procedure and no intraoperative complication. The operative time ranged from 105 to 420 minutes (mean, 219). Postoperatively, 1 patient had urinary retention and 1 patient had postoperative fever. Hospital stay ranged from 3 to 10 days (mean, 4.8). Mean follow-up time was 38 months (range, 17–46). VURs were resolved for the 2 children with simple VUR and was downgraded for the child with duplex kidney. All patients who underwent pyeloplasty showed satisfactory urinary drainage after the operation.
Conclusions:
From this early experience, robotic-assisted urologic operations in children were safe and feasible. It was particularly useful in reconstructive operations that required precise suturing, such as ureteric reimplantation and pyeloplasty.
Introduction
Materials and Methods
A retrospective review was carried out for all children undergoing robotic-assisted laparoscopic reconstructive urologic operations from November 2005 to April 2008. It included 3 children who had vesicoureteric reflux (VUR) and 5 children who had pelvic-ureteric junction obstruction (PUJO). At the start of the operation, a urethral catheter was inserted. A 12-mm robotic trocar was inserted subumbilically by the open Hasson technique. The carbon-dioxide (CO2) pneumoperitonium was maintained at 10–12 mm Hg. A 12-mm laparoscope was used. For children with VUR, two 5- or 8-mm robotic trocars were inserted on the left and right sides of the umbilicus. A Lich-Gregoir extravesical ureteric reimplantation was performed. The peritoneum over the distal ureter was incised, and the ureter was mobilized. A vertical detrusor incision was made and was taken to the level of the mucosa for approximately 2.5–3 cm. A detrusor tunnel was developed. The distal ureter was then wrapped by the detrusor flap, using 5-O absorbable sutures (Fig. 1). The peritoneum was closed with the sutures. The urethral catheter was kept overnight.
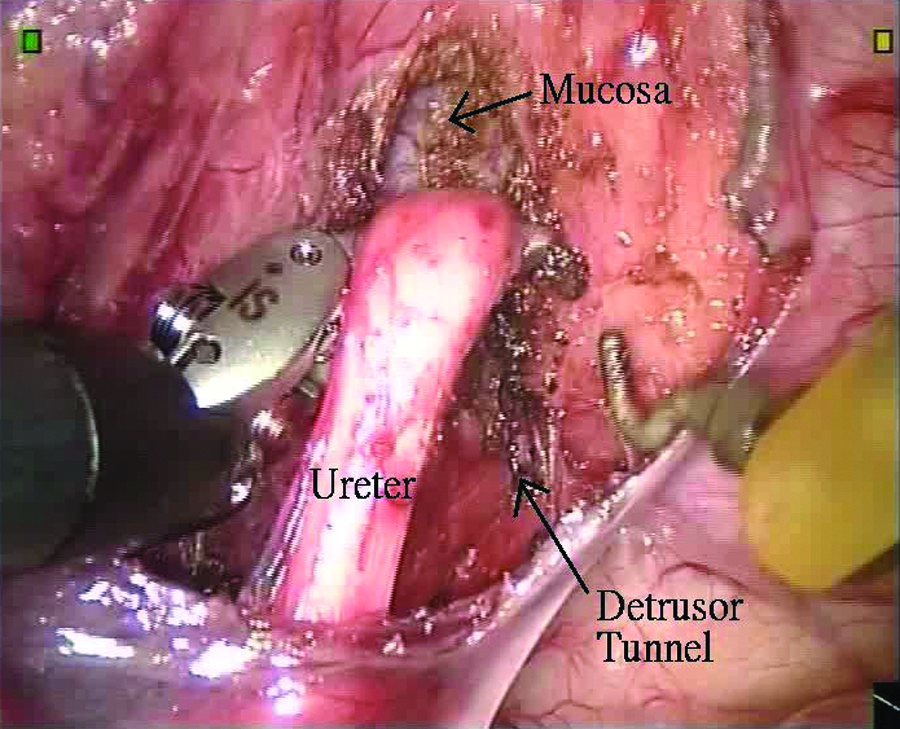
Extravesical reimplantation of the left ureter.
In children with PUJO, the operative side was elevated with a gel wedge to about 30 degrees. Two 8-mm ports were inserted over xiphisternum and on the midabdomen over the operative side. The pelvic-ureteric junction was approached either through the mesenteric window or after reflection of the colon. A 4-O nonabsorbable suture was passed percutaneously and hitched up the renal pelvis. The dysplastic proximal ureter and the adjoining renal pelvis was resected. The ureter was spatulated laterally. The posterior anastomosis was first performed by using 5-O absorbable sutures. A guidewire was passed percutaneously and through the spatulated ureter into the bladder. A double-J catheter was then inserted, with one end inside the bladder and the other side in the renal pelvis. Finally, anterior anastomosis (Fig. 2) was performed and the renal pelvis was closed. No drain was inserted, and the mesenteric defect was not closed. The urethral catheter was kept for 2–3 days. The double-J catheter was kept for 6 weeks.
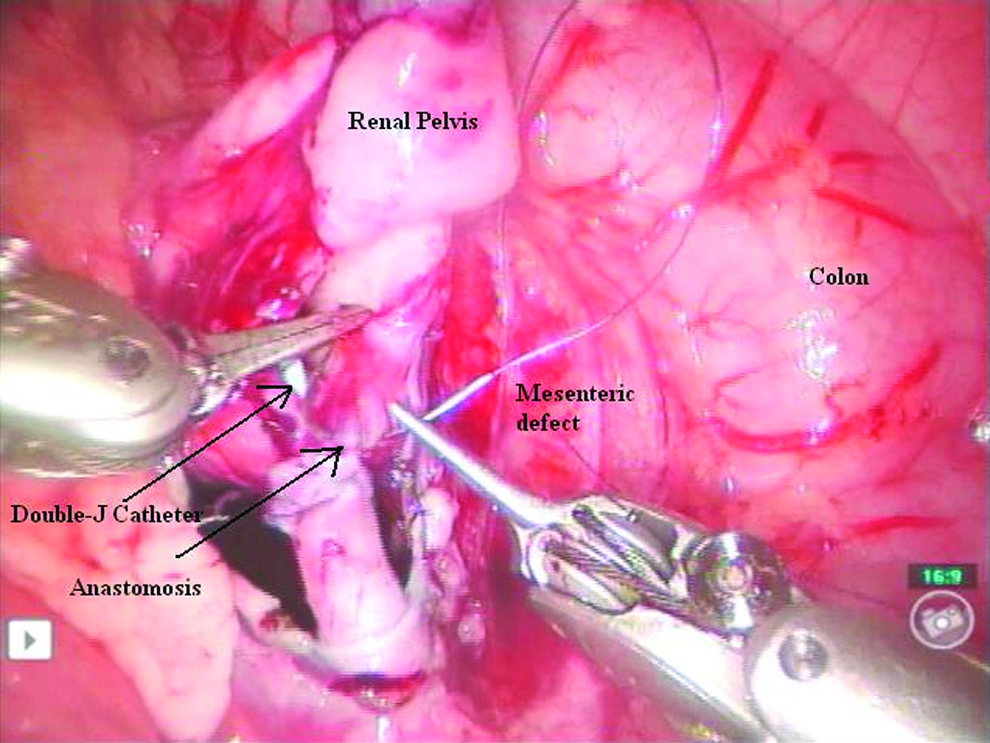
Anastomosis of the spatulated ureter to the renal pelvis.
Results
Three boys underwent robotic-assisted extravesical ureteral reimplantation for VUR, and 5 children (4 boys and 1 girl) underwent robotic-assisted pyeloplasty for PUJO (Table 1). The mean age was 5.9 years (range, 11 months to 12 years). There was no intraoperative complication or conversion to open procedure. The hospital stay ranged from 3 to 10 days (mean, 4.8). The mean follow-up time was 38 months (range, 17–46).
VUR, vesicoureteric reflux; PUJO, pelvic-ureteric junction obstruction; UTI, urinary tract infection.
For the children with VUR, they all presented with urinary tract infection (UTI). It included 2 children with unilateral grade IV VUR. The operative time was 105 minutes in each case. Postoperatively, 1 child suffered from retention of urine. Postoperatively, cystourethrogram showed the refluxes were resolved. One boy had duplex right kidney. He had had a laparoscopic right-lower moiety nephroureterectomy performed in the past. Preoperative imaging showed grade IV reflux to the right-upper moiety and grade II VUR to the left ureter. Subureteral injection for the left VUR and robotic-assisted excision of the right-lower moiety ureter stump were performed, together with an extravesical reimplantation of the right-upper moiety ureter. Operative time was 420 minutes. Postoperative imaging showed a downgrade of the right VUR to grade III and a resolution of the left VUR. There was no urinary tract infection postoperatively.
For the 5 children with PUJO, 1 child presented antenatally with hydronephrosis. Two children presented with UTI, and 2 older patients presented with loin pain. Mean operative time was 224 minutes (range, 160–255). One child who had a postoperative fever responded to antibiotic treatment. Isotope imaging, performed 3 months postoperatively, showed that all patients had satisfactory isotope drainage and all children are symptom free.
Discussion
Laparoscopic reconstructive urologic operations, such as pyelopalsty and extravesical ureteric reimplantation, were surgically feasible but technically demanding. A long learning curve in laparoscopic reconstructive operations was universally observed.6,7 One of the benefits on the use of the da Vince robotic system was the short learning curve and was even feasible for surgeons who were not familiar with laparoscopic techniques.8,9 Robotic-assisted pyelopalsty was the most common published urologic operation in children.10–15 With our experience in complex MIS in pediatric urology,16,17 we did found the operative setting was just the same as the routine laparoscopic operation. Although the number of operations we performed was not as many as some of the published series,10–15 our operative time was comparable to their results. Our results suggested the learning curve of robotic surgery was fast.
The surgical management of VUR included subureteral injection as well as extra- or intravesical reimplantation. 18 There were only limited reports on laparoscopic extravesical reimplantation.3,6 This operation was very technical demanding because of the deep location of the vesicoureteric junction and the unfavorable position on laparoscopic suturing. Because robotic surgical arms provided seven degrees of freedom, rather than four degrees of freedom in ordinary laparoscopic instruments, suturing during reimplantation was relatively simple. The 3D telescope provided excellent perception during incision of the detrusor muscle during the creation of the detrusor tunnel. Urinary retention was one of the known complications in extravesical reimplantation. The incidence was reported up to 10% in bilateral reimplantation.19,20 One patient had urinary retention after reimplantation. Recently, the use of nerve-sparing extravesical reimplantation was reported to minimize the risk of urinary retention. 21
In our institute, we only perform robotic-assisted urologic operations that require complex reconstruction. Although a 5-mm robotic laparoscope was available, it only provided 2D imaging. Thus, the beneficial effect of depth perception provided by the 12-mm scope was absent. On the other hand, the design of 8- and 5-mm instruments were different. We found that the 5-mm robotic laparoscopic instruments were less user friendly than the 8mm instruments, because the noninsulating portion of the 5-mm instruments was longer. 10 With respect to the use of the 5- and 3-mm laparoscopic instruments in ordinary laparoscopic pediatric urology operations, the robotic-assisted operation did not provide superior cosmesis, when compared to the traditional laparoscopic operation. We do not think that the use of a robotic system had an obvious advantage in the simple laparoscopic urology operation, such as nephrectomy, for dysplastic kidney or the management of undescended testis.
Conclusions
Our early experience showed robotic-assisted laparoscopic reconstructive surgery in pediatric urology can be safely performed and can achieve a good outcome. A fast learning curve and the advantages in delicate suturing and dissection were observed. The development of smaller robotic instruments and a 3D laparoscope can provide additional benefits to cosmesis, when compared to traditional laparoscopic surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.