
Abstract
Abstract
Background:
Conventional laparoscopic distal pancreatectomy (DP) is now regarded as a safe, effective treatment modality; however, pancreatic transections are mostly believed to be somewhere between the body and tail of the pancreas. Laparoscopic DP, with its division at the pancreatic neck (subtotal pancreatectomy [STP]), is more challenging because there are major vascular structures, such as the celiac axis, coronary vein, and superior mesenteric vein-splenic vein-portal vein (SMV-SV-PV) confluence around the pancreatic neck portion to be dissected.
Patients and Methods:
Ten patients underwent laparoscopic STP with pancreatic division at the level of SMV-SV-PV confluence for benign and borderline pancreatic disease.
Results:
Three patients were male and 7 were female, with a median age of 60 years (range, 28–73). All patients had benign or borderline malignant tumors in the body near the neck of the pancreas, with a median tumor size of 3 cm (range, 1–9.2). The operation time was a median of 287.5 minutes (range, 160–480). The intraopeative bleeding was a median of 300 mL (range, 100–700). Spleen preservation was carried out in 8 patients. Compared with open DP with the division of the pancreatic neck, a more frequent rate of spleen preservation (P = 0.004), longer operation time (P = 0.006), and early postoperative recovery presented by early intake of a soft diet (P = 0.001) and earlier discharge (P = 0.03) were significantly more frequent in the laparoscopic STP group. In a comparative study with laparoscopic DP, the longer segment of resected pancreas (P < 0.001), smaller amount of blood loss (P = 0.019), and high rate of spleen preservation (P = 0.019) were also noted in the laparoscopic STP group.
Conclusions:
Laparoscopic DP with division of the pancreatic neck is considered feasible and safe.
Introduction
All laparoscopic DPs are not thought to be similar procedures. The technical demand may be different, according to the division line of the pancreas (dividing the body or tail of the pancreas versus division of the pancreatic neck), because the laparoscopic distal pancreas with the division of the neck of the pancreas (referred to as subtotal pancreatectomy [STP]) is thought to be a much more demanding procedure. Division of the pancreas at the neck often implies greater risk to the underlying retroperitoneal vasculature due to the proximity of these structures to the dissection. Careful dissection is required when separating the pancreas neck from the underlying portal venous system and to avoid injuring the celiac trunk or hepatic artery during the division of the pancreas. A recent large series of laparoscopic DPs seemed not to consider this issue,5,7–9,19 and only a few reports have been published in dealing with this specific type of laparoscopic DP resection.3,4,19 In this retrospective study, we would like to provide our early experience with laparoscopic STP in benign and borderline malignant tumors near the proximal body of the pancreas.
Materials and Methods
From January 2007 to January 2009, the patients who underwent laparoscopic STP for benign and borderline malignant pancreatic lesions were retrospectively reviewed.
Surgery
A brief operative procedure was introduced. The patient was placed in the supine position with the head and left side elevated (a mirror image to the usual laparoscopic cholecystectomy). The surgeon and a camera-assistant surgeon stood on the right side of the patient, while another assistant surgeon and scrub nurse stood on the opposite side of the patient. A total of four trocars (one 12-mm for the laparoscope and one 12-mm and two 5-mm trocars for working) were used for this surgical procedure (Fig. 1). Two monitors, a carbon-dioxide (CO2) pneumoperitoneum (12 mm Hg), a 30-degree laparoscope, a 5-mm endo-clip, a Harmonic scalpel (Ethicon Endo-Surgery, Cincinnati, OH), and an Endo-GIA stapler (blue [60-3.5]; Covidien) were used. We began with the division of the gastrocolic ligament without the division of the left gastroepiploic artery. The lienocolic and gastrolienal ligaments were not divided in case of concomitant resection of both splenic vessels. The distal pancreas, containing the pancreatic mass, was mobilized by dissection of the retropancreatic avascular plane along the inferior margin of the pancreas. Careful dissection of the pancreatic neck portion could allow surgeons to identify the superior mesenteric vein-splenic vein-portal vein (SMV-SV-PV) confluence and continue to make a complete window between the pancreatic neck portion and vascular confluence (Fig. 2). The right gastroepiploric vein can be an anatomic landmark for the identification of an SMV-SV-PV confluence. The continuous careful dissection along the right gastroepiploric vein can lead to the lateral aspect of main SMV. Another technical tip for the identification of an SMV-SV-PV confluence is to find SV during the dissection of the distal part of the pancreas. Careful dissection toward the pancreatic neck portion can lead to the inferior mesenteric vein and, eventually, SMV-SV-PV confluence. During this procedure, usually one or two small tributary vessels between the SMV-SV and body of the pancreas need to be divided. The space between the pancreatic neck and SMV-SV-PV confluence is the avascular plane. A complete window is usually created by blunt dissection with a laparoscopic suction instrument. If the connective tissue in this plane is thought to be dense, hydrostatic dissection (i.e., injection pressure of saline through a laparoscopic suction instrument) can facilitate this blunt dissection. Nylon tape was applied to encircle the pancreatic neck portion through this window and was then used for the traction of the pancreas. To ensure a clear resection margin, laparoscopic ultrasound was freely applied. In case of a larger mass, however, it was also possible to estimate a proper division line, based on the preoperative imaging study. The pancreatic neck was transected by using an Endo-GIA 60-3.5 stapler with the nylon tape tracked toward the patient's left side. After division of the pancreas, careful dissection between the pancreas and splenic vessels was continued to the splenic hilum by Harmonic scalpel and laparoscopic dissection with a 5-m endo-clip. Soon after, several additional sutures or an endo-clip were applied along the stapled line after removing the distal pancreas (Fig. 3).

Laparoscopic port placement. A total of four laparoscopic ports were placed for this procedure. The reticulated Endo-GIA Stapler (blue [60-3.5]; Covidien) was usually introduced through the left-sided 12-mm port site.
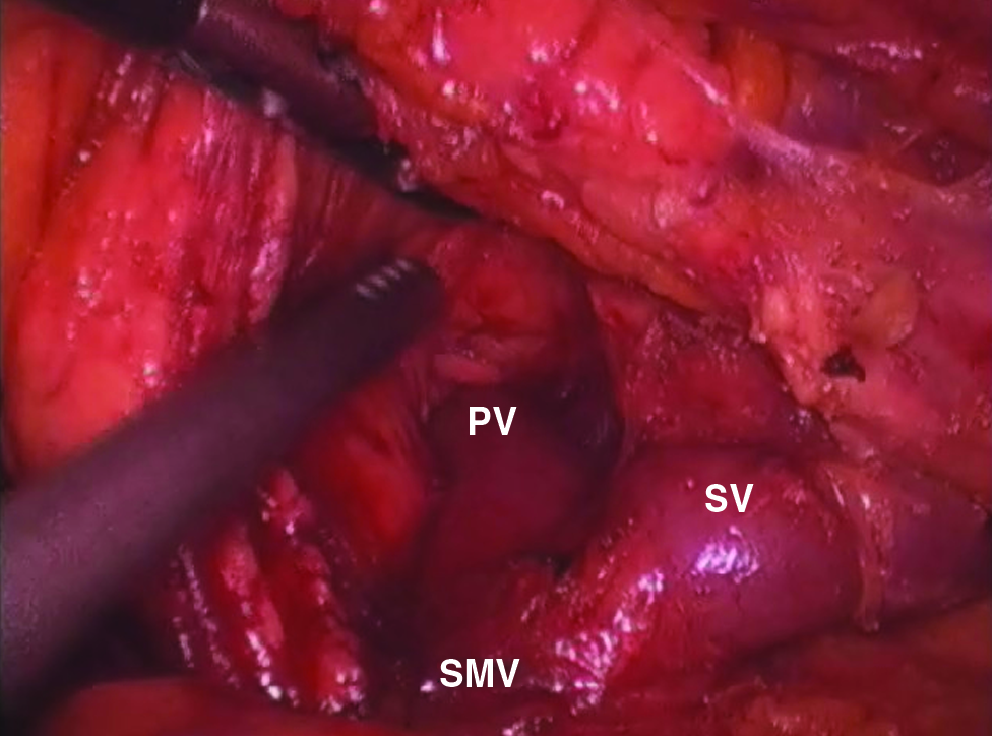
Dissection of a pancreatic neck. Careful dissection resulted in a complete pancreatic window between the pancreatic neck and SMV-SV-PV confluence. PV, portal vein; SMV, superior mesenteric vein; SV, splenic vein.
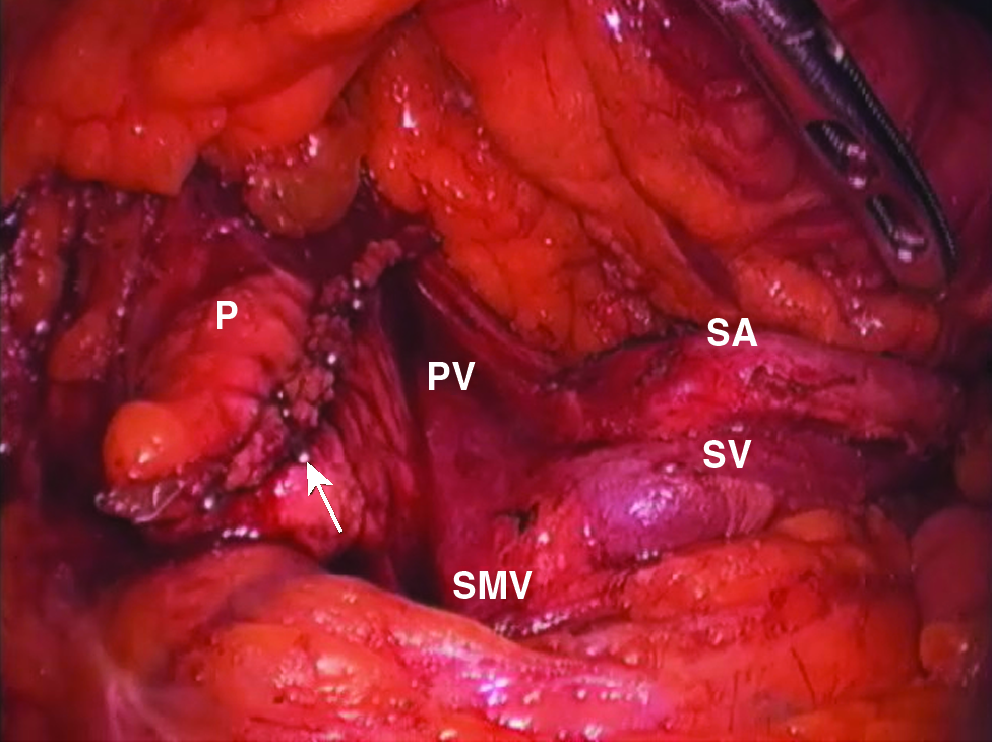
Operative view after laparoscopic distal pancreatectomy. SMV-SV-PV confluence is clearly noted. Both splenic vessels are well conserved. A serially applied 5-mm metal clip, along the line of the resected pancreas, is noted (arrow). P, pancreatic stump; PV, portal vein; SMV, superior mesenteric vein; SV, splenic vein; SA, splenic artery.
Perioperative clinicopathologic variables were evaluated. Patients who had received elective open STP for benign and borderline malignant pancreatic pathology during the last 10 years were also reviewed for the purpose of comparative analysis. In addition, we added another comparative analysis between laparoscopic STP and the usual laparoscopic DP, for which a pancreatic division line was placed between the body of the pancreas and the tail. Categoric variables were expressed as frequencies and percentages and continuous variables as mean ± standard deviation (or range). We compared pre-, intra-, and postoperative clinical variables between the two groups (open STP versus laparoscopic STP). Differences were evaluated by chi-square or Fisher's exact test (if needed) and the Student's t- or Mann-Whitney test (if needed). The values were considered significant when P < 0.05.
Results
General characteristics of patients with laparoscopic STP
From January 2005 to January 2009, 10 patients who underwent laparoscopic STP for benign and borderline malignant pancreatic lesions in the proximal body of the pancreas were evaluated. There were 7 female and 3 male patients, with a median age of 60 years (range, 28–73). Two patients underwent previous abdominal surgeries, such as Mile's operation, due to rectal cancer or exploratory laparotomy for debunking ovarian cancer. All patients were incidentally found to have pancreatic pathologies during the routine medical check-up, without any specific symptoms. The da Vinci® robot system (Intuitive Surgical, Inc., Sunnyvale, CA) was used in 1 patient, and the remaining patients underwent conventional laparoscopic surgery. The median operation time was 287.5 minutes (range, 160–480). Median intraoperative bleeding was 300 mL (range, 100–700), and only 1 patient needed an intraoperative transfusion. However, we found that operation time and intraoperative bleeding has been significantly decreased as experience has accumulated (Fig. 4). Eight patients had their spleens preserved during laparoscopic STP. One patient required a concomitant splenectomy, due to uncontrollable bleeding during dissection of the pancreatic tail around the splenic hilum, and the other patients who had previously received Mile's operation due to rectal cancer were though to have both splenic and pancreatic metastasis in the follow-up imaging study. Most patients could tolerate a soft diet by postoperative day 2 (median, 1.5 days; range, 1–3) and went home on day 6 (median) after surgery (range, 5–15). Two patients experienced postoperative complications (i.e., bleeding and pancreatic fistula, grade B), but were successfully treated with conservative management.

Change of operation time and estimated blood loss over case sequence. The operation time and estimated blood loss decrease as experiences are accumulated.
Comparative analysis between open STP and laparoscopic STP
Compared with open STP, almost preoperative and operative clinical parameters were observed to be similar between the two groups (P > 0.05). However, longer operation time (P = 0.006), more frequent rate of spleen preservation (P = 0.004), early intake of a soft diet (P = 0.001), and earlier discharge (P = 0.03) were considerably more prevalent in the laparoscopic DP group (Table 1).
Two patients experienced more than grade B pancreatic fistula. One patient required an exploratory laparotomy due to associated abscess and peritonitis, and the other required a percutaneous drainage procedure.
P-value in comparison between open STP and laparoscopic STP.
P-value in comparison between laparoscopic STP and laparoscopic DP.
STP, subtotal pancreatectomy; DP, distal pancreatectomy; POD#, postoperative day number; NS, not significant; ChrPan, chronic pancreatitis; NET, neuroendocrine tumor; IPMT, intraductal papillary mucinous tumor; SPT, solid pseudopapillary tumor; MCT, mucinous cystic tumor; SCT, serous cystic tumor.
Comparative analysis between laparoscopic STP and laparoscopic DP
When we compared laparoscopic STP and the usual laparoscopic DP, a longer length of resected pancreas (P < 0.001), less intraoperative bleeding (P = 0.019), and more frequent spleen-preservation rate (P = 0.019) were noted. However, there were no significant differences in the general characteristics of patients, operation time, transfusion, tolerable diet start, length of hospital stay, complication, and mortality between the two groups (Table 1).
Discussion
Several studies have demonstrated the feasibility and safety of laparoscopic DP with or without splenectomy.4,5,8–11,20–21 In their reports, researchers described their surgical techniques, such as patient position, how the working ports were placed, how to divide the pancreas, and how to preserve the spleen. However, the pancreas was believed to be divided somewhere between the body and tail of the pancreas. Actually, it is hard to find exact documentation of a laparoscopic DP when dividing the neck of the pancreas. This might be due to the following reasons. The laparoscopic STP must be a more challenging and demanding procedure for laparoscopic surgeons, compared to the usual laparoscopic DP, pancreatectomy with a transection line located between the body and tail of the pancreas. The major vessels, including the SMV-SP-PV confluence and celiac trunk containing the common hepatic and splenic arteries, are inevitably encountered while making a window around the pancreatic neck in preparing to divide the pancreas. In addition, the full length of splenic vessels (from the origin of the celiac trunk to the splenic hilum) should be carefully dissected and controlled for the preservation of the spleen in such spleen-preserving laparoscopic procedures performed on benign and borderline malignant pancreatic lesions. For these reasons, surgeons might prefer an open STP with or without a splenectomy when the pancreatic pathology requires a division of the pancreatic neck. Cuschieri et al. 3 specifically addressed the feasibility and safety of the laparoscopic distal 70% pancreatectomy and splenectomy for chronic pancreatitis in 1996. In this report, they clearly documented that the pancreatic neck portion was divided by an Endo-GIA or Endo-TA stapler. Recently, Fernandez-Cruz et al. 4 also dealt with laparoscopic STP in malignant neoplasm of the pancreas. However, they did not provide a concrete description for the benign and borderline malignant lesions.
We prefer the supine position, with the head and left side elevated (the mirror image of the laparoscopic cholecystectomy position). This position can create the same operative condition as conventional open surgery and enhance accessibility for the dissection of the pancreatic neck. It was possible to divide the pancreas, even at the right side of the SMV-SV-PV confluence, when the pancreas was divided with nylon tape around the pancreatic neck tracked toward the patient's left side. We usually applied an Endo-GIA stapler at the pancreatic neck above the SMV-SV-PV confluence for dividing the pancreas. A Harmonic scalpel was used for dividing the neck of the pancreas in 1 case of robot-assisted distal pancreatectomy. After transecting the pancreas, we promptly applied an individual ligation of the pancreatic duct, with parenchymal approximation by interrupted sutures (in the robotic surgery case) or 5-mm clips along the staple line (in the conventional laparoscopic surgery cases) as an effort to reduce the chance of postoperative pancreatic fistula. Our data show only 1 patient with a clinically relevant pancreatic fistula (grade B), who could only be successfully managed by antibiotic therapy. In fact, a 5–34% postoperative pancreatic fistula rate was reported in a recent large series of distal pancreatectomies.2,12,22–24
According to our results, laparoscopic STP seems to be feasible and safe. Even though this study was based on a retrospective design, early oral intake and shorter hospital stay were observed in comparative analysis between open STP and laparoscopic STP. When comparing to laparoscopic DP, laparoscopic STP provided a small amount of blood loss during the operation. Other clinical variables, including gender, age, previous abdominal surgery, body mass index, tumor size, transfusion, diet start, complications, and morality, were similar to laparoscopic DP. Therefore, laparoscopic STP is thought to be performed without increasing operative risk, when compared to either open STP and laparoscopic DP.
Interestingly, the spleen was successfully preserved by mostly conserving both the splenic artery and vein in 8 patients. Only 1 patient with chronic pancreatitis required a segmental resection of both splenic vessels due to difficulty with the individual ligation of tributary vessels between the pancreas and splenic vessels. However, most small tributary vessels between the splenic vessels and distal pancreas could be managed with the Harmonic scalpel, and two or three relatively large vessels needed to be ligated by several laparoscopic clips. In recently published studies comparing laparoscopic DP with open DP, the spleen-preservation rate was also found to be higher in the laparoscopic group (62 versus 17% 10 and 40.8 versus 5.7% 5 ). The laparoscopic view can provide a magnified operative field view and facilitate the isolation and dissection of small tributary vessels between the pancreas and splenic vessels. Another potential reason was due to the increasing emphasis on the role of spleen. We recently tried to avoid unnecessary splenectomy in the case of DP for benign and borderline malignant tumors. However, in this retrospective review (most open surgeries were done in the 1990s), it was true that we could not exactly know how much surgeons did try to preserve patients' spleens when they performed open laparoscopic DPs during our study period. Traditionally, the splenectomy usually combined DP just for anatomic intimacy and the comfort associated with surgical procedure. Technically, dissection between the anatomic avascular plane between the SMV-SV-PV confluence and pancreatic neck can provide a bloodless operative view for further dissection between the splenic vessels and distal pancreas, when compared with the usual laparoscopic DP. The estimated blood loss was much larger in the usual laparoscopic DP group than the laparoscopic STP, which might indirectly suggest the better chance of spleen preservation in laparoscopic STP.
However, this study was a retrospective design with relatively long study period, especially in the group of open STP. During the last 10 years, potential selection bias needs to be considered in interpreting current results. Currently, as a fast-track recovery program has been actively applied in open surgery, a relatively small number of asymptomatic patients is increasing due to incidental discovery during the routine medical check-up, and our management strategy of DP in benign and borderline malignant disease recently has changed from conventional open surgery to laparoscopic surgery. However, an important message from our results is that even laparoscopic STP is feasible and safe in well-selected patients in our clinical practice.
We think this technique of laparoscopic STP seems to provide potential usefulness in clinical practice. The concept of radical antegrade modular pancreatectomy (RAMP),25,26 which provides early transection of the pancreas with subsequent right-to-left dissection in the distal pancreas, is thought to be applied by this approach. However, early vascular division and splenectomy were omitted in this technique, because the pancreatic pathology was benign and borderline malignant lesions deserved spleen preservation. Therefore, we feel this technique might also be useful for treating well-selected patients for left-sided pancreatic cancer. As Fernandez-Cruz et al. 4 have already demonstrated, we could clearly identify the celiac trunk containing the common hepatic, left-gastric, and splenic arteries after dividing the pancreatic neck. The splenic vein is also thought to be safely divided at the junction of the SMV-SP confluence. After dividing vascular control, a right-to-left distal spleniopancreatectomy with soft tissue around the major vessels is thought to be possible. Despite the fact that applying laparoscopic pancreatectomies for pancreatic cancer is still controversial, 6 anterior RAMP is thought to be sufficiently performed in well-selected patients by this laparoscopic approach. In fact, we recently experienced 4 cases of laparoscopic anterior RAMP for pancreatic cancer. Pathologic reports were all of margin negative resection, but careful follow-up is still mandatory.
Laparoscopic central pancreatectomies have been reported.13,14 Considering the fact that the central pancreatectomy has been performed in rare cases and only a few surgeons are available for laparoscopic central pancreatectomies because of the high rate of central pancreatectomy-related postoperative complications, the laparoscopic STP may be an alternative, comparable approach for benign and borderline malignant pancreatic tumors around the pancreatic neck portion because the proximal pancreatic transection line in central pancreatectomy may be identical to that of laparoscopic STP. In this study, we did not deal with follow-up residual pancreatic function, because the follow-up period was too short to allow for accurate conclusions (median follow-up period: less than 6 months). Actually, we recently have performed 5 cases of robot-assisted central pancreatectomy (not published). A future comparative study between our two groups might be another interesting issue in managing benign and borderline pancreatic lesions near the neck and the proximal body of the pancreas.
Conclusions
In conclusion, our results suggest laparoscopic STP in benign and borderline malignant lesions is also feasible, safe, and dose not provide a negative impact on the spleen-preserving rate, compared to open STP or laparoscopic DP. More experience and careful follow-up studies should be conducted.
Footnotes
Acknowledgments
This study was supported by a faculty research grant of Yonsei University College of Medicine for 2006 (6-2006-0086).
Disclosure Statement
No competing financial interests exist.
Part of this article was presented in the 2nd Biennial Congress of the Asian-Pacific-Hepato-Pancreato-Biliary Association (March 25–27, 2009) held in Bangkok, Thailand.