
Abstract
Abstract
Background:
Various methods for complete endoscopic resection of rectal carcinoid tumors have been reported. The aim of the present study was to evaluate the clinical usefulness of endoscopic submucosal dissection (ESD) as a new method or conventional endoscopic mucosal resection (EMR) in order to remove rectal carcinoid tumors completely.
Materials and Methods:
Between April 2004 and June 2009, 12 patients with rectal carcinoid tumors, estimated at 10 mm, more or less, in diameter, without atypical features and dissected by ESD or resected by EMR, were recruited for this analysis. The complete dissection or resection rate, complications associated with the procedure, local recurrence, and distant metastases were evaluated.
Results:
Twelve patients were 9 males and 3 females with a mean age of 47.6 years (range, 32–64). The patients had no complaints of carcinoid syndrome symptoms. Tumor size ranged from 5 to 13 mm in diameter, with an average size of 8.8 mm, and 11 of 12 patients (92.7%) had tumors of diameter less than 10 mm. Three of 12 patients (25.0%) were treated by ESD and 9 (75.0%) by conventional EMR. All lesions, including 13-mm-sized carcinoid tumors, were histologically determined to be completely dissected or resected. There were no immediate or late complications (i.e., bleeding or perforation) after ESD or conventional EMR. Histopathologically, there was no tumor invasion beyond the submucosal layer, and all were classified as classical-type carcinoids without lymphovascular invasion. Neither local recurrence nor distant metastasis were detected during a median follow-up period of 28 months.
Conclusions:
In this study, ESD as a new method or conventional EMR shows promise or potential as a useful, safe procedure to dissect or resect rectal carcinoid tumors of 10 mm, more or less, in diameter. However, long-term outcome remains to be elucidated by a large-scale, prospective study.
Introduction
Materials and Methods
Patients and lesions
Between April 2004 and June 2009, a total of 12 patients (9 males, 3 females; mean age, 47.6 years; range, 32–64) with 12 rectal carcinoid tumors, confirmed by histopathologic evaluation of endoscopic biopsy specimens and considered as good candidates, were treated by endoscopic submucosal dissection or conventional endoscopic mucosal resection at Kangnam Sacred Heart Hospital, Hallym University College of Medicine (Seoul, Korea). No patients had symptoms of carcinoid syndrome. Eleven patients (92%) underwent computed tomography (CT) or sonography in order to evaluate size and to assess whether there had been metastases to the pararectal lymph nodes. Investigation of the patients by CT showed that none of the tumors were associated either with pararectal lymph node metastases or with distant metastases. Informed written consent for ESD or EMR was obtained from all patients prior to treatment.
Endoscopic procedures
All resections were performed by experienced endoscopists. ESD (Fig. 1) or conventional EMR was performed by using a conventional single-channel Olympus endoscope (CF-Q260AL; Olympus Optical Co., Tokyo, Japan). The procedure was performed as follows. Hypertonic saline, mixed with epinephrine and indigocarmine, was, first, injected into the submucosal layer beneath the tumor to elevate it and thereby reduce the risks of perforation and resection margin involvement. Submucosal dissection or snare resection was performed by using endocut Q, effect 3, duration 3, interval 4 or endocut Q, effect 2, duration 1, and interval 4, respectively (VIO 300D; ERBE, Tübingen, Germany). The resection specimen was removed by retrieving it with a grasping forceps (Olympus Optical Co.).
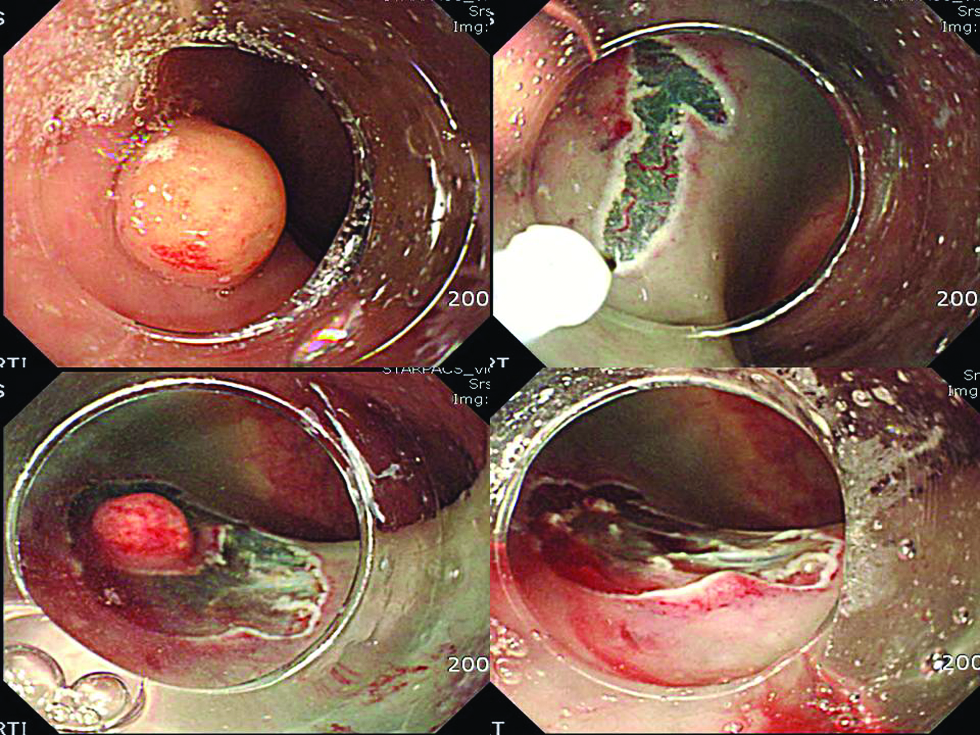
Endoscopic submucosal dissection. After marking surrounding the lesion and subsequent injection of hypertonic saline mixed with epinephrine and indigo carmine, the needle knife is advanced to dissect the submucosal layer. The mucosa is dissected from margin to center.
Histopathologic evaluation
The resected specimens were stained with hematoxylin and eosin and examined microscopically for histopathologic diagnosis, tumor size, depth of invasion, histological atypia, lateral and vertical margin involvement, and lymphovascular invasion. 8 We defined complete resection as no lateral and vertical margin involvement of the resected specimen, histopathologically.
Follow-up
Patients were followed up by chest radiography, abdominal CT (58%), and colonoscopy (42%) 1 year after treatment. Patients continued to undergo a median follow-up period of 28 months.
Results
The results are summarized in Table 1. The sizes of resected tumors ranged from 5 to 13 mm in diameter (mean, of 8.8). All tumors were sessile. Histopathologically, none of the tumors had invaded beyond the submucosal layer, and no tumors showed atypia; there was no tumor invasion at the lateral and bottom edges of any resected specimens, confirming complete resection, in all cases (Fig. 2). Neither vascular nor lymphatic invasion was observed in any resected carcinoid tumor. There were no immediate or late complications after ESD or conventional EMR. No local recurrences or distant metastatic lesions have been identified in any of the patients after a mean follow-up period of 28 months after treatment.
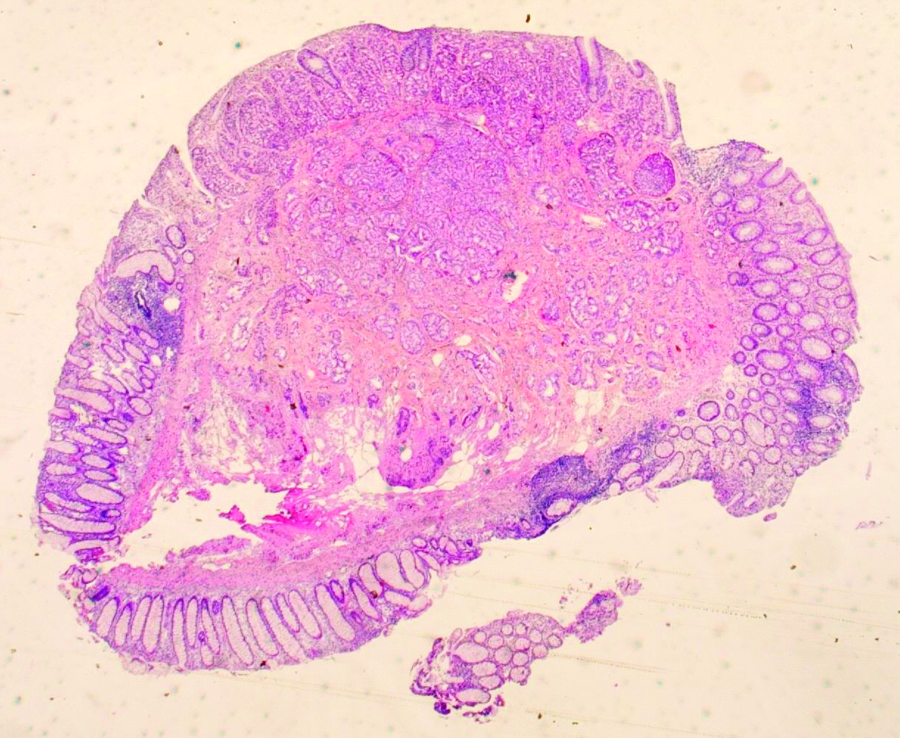
Histologic view of a rectal carcinoid tumor obtained by endoscopic submucosal dissection. The tumor was confined to the submucosa and resected completely, with tumor-free surgical margins. Tumor cells arranged in nests and rosette-like structures (hematoxylin and eosin stain; ×100).
ESD, endoscopic submucosal dissection; C-EMR, conventional endoscopic mucosal resection.
Discussion
Prevalence of rectal carcinoid has been reported as 0.07% in healthy subjects 5 and 0.10% in subjects of total colonoscopy in Japan. 9 Rectal carcinoid tumors estimated endoscopically as small, less than 10 mm in size without atypical features, and confined to the submucosal layer without lymphovascular invasion rarely metastasize and can thus be treated by local resection.2–4 Rectal carcinoid tumors are treated by surgical operation with the trans-anal approach 10 or various types of endoscopic resection techniques,11–15 such as strip biopsy, aspiration resection, band-snare resection, endosonography probe-guided band ligation, conventional EMR, and ESD as a new method. We have reported that ESD or conventional EMR are sufficient for complete resection, although the number of cases we investigated was small and included only 12 patients. We conducted this retrospective analysis to establish the effectiveness and safety of ESD or conventional EMR in a large number of lesions. In our study, ESD or conventional EMR provided an overall high complete resection rate of 100.0% (12/12). No lesion resulted in margin involvement after ESD or conventional EMR and were histopathologically considered as complete resections. No local recurrence or distant metastasis was detected within a short period after ESD or conventional EMR. As the rectal wall is thick and supported by surrounding connective tissue, ESD or conventional EMR could be performed to achieve a deeper vertical margin without perforation. Therefore, it provided a higher complete resection rate in our series. The number of cases in each procedure was relatively small, however, so we should increase the number of cases in the future. Rectal carcinoid tumors are, most frequently, detected in the rectum, 8 cm from the anorectal junction. 2 Therefore, almost all rectal carcinoid tumors could be removed completely by ESD or conventional EMR without any procedure-related complications. The most frequent complications associated with endoscopic resection are bleeding and perforation. In our study, we had no major bleeding or perforations. We experienced no complications requiring surgery or blood transfusions. Therefore, ESD or conventional EMR could be performed safely for the resection of rectal carcinoid tumors.
Conclusions
In conclusion, ESD or conventional EMR might be a most effective, minimally invasive, and safe procedure to completely remove rectal carcinoid tumors of 10 mm, more or less, in diameter that have remained within the submucosal layer.
Footnotes
Disclosure Statement
No competing financial interests exist.