
Abstract
Abstract
Aim:
The aim of this study was to evaluate the safety and efficacy of the Harmonic scalpel (Ethicon Endo-Surgery, Cincinnati, OH) in the closure/division of the cystic duct and artery, and bladder dissection in laparoscopic cholecystectomy as a single working instrument, with the use of a two-working-trocar technique, compared with the regular laparoscopic clip/cautery, three-trocar technique.
Methods:
This prospective study included 160 patients with symptomatic gallstone disease who were randomly assigned for laparoscopic cholecystectomy by either Harmonic shear as a single working instrument, with the two-trocar technique (group 1 = 80 patients) or group 2 (regular clip/cautery, three-trocar technique) comprising 80 patients.
Results:
No significant complications were encountered in either group; however, 1 case in the regular laparoscopy group suffered mild leakage that was treated conservatively. Intraoperative bile spillage was insignificantly comparable in both groups (10 versus 13%; P = 0.46). The median operative time was statistically significantly shorter in the Harmonic group (20 versus 45 minutes; P = 0.0001). Also, hospital stay was significantly shorter in the Harmonic group (1 versus 1.5 days, respectively; P = 0.001), but no statistically significant difference was found in the incidence of postoperative complications. The overall cosmetic results and patient satisfaction was better in the Harmonic group.
Conclusions:
The Harmonic shear is as safe and effective as the clip/cautery technique in laparoscopic cholecystectomy in achieving hemobiliary stasis, with shorter operative time, especially if used solely as a working instrument. The two-trocar technique is safe, feasible, and provides better cosmetic results and patient satisfaction.
Introduction
The resulting decrease in temperature, smoke, and lateral tissue damage has placed the Harmonic scalpel in contrast to the effects seen with more traditional electrocautery. In addition, the elimination of inadvertent, sometimes unrecognized, electrical arcing injuries, with their potentially hazardous sequelae, has supported the role of the Harmonic scalpel as a potentially safer instrument for tissue dissection. 1 It tackles the concerns regarding smoke production, and inadvertent injuries to the abdominal organs and structures; 5 moreover, it shortens the operative time and decreases the rate of accidental bile spillage. 6
A single working instrument means avoidance of repeated instrument changes during the operation, as selecting different instruments breaks the natural flow of the operation and may distract the surgeon. 5 Moreover, downsizing port incisions may reduce pain after laparoscopic cholecystectomy, 7 thereby minimizing the number and scope of ports to improve postoperative pain control, rapid return to activity and work, patient satisfaction, and cosmetic result achieved by the laparoscopic method. 8 So, new techniques for laparoscopic cholecystectomy were designed to reduce the number of trocars or the use of very thin instruments, with the aim of further minimizing surgical invasiveness.9–11 Some researchers use one 1-mm Kirschner wire, introduced at the subcostal line and bent with a special designed device to hook the gallbladder and pull it up, 12 whereas others use 2-mm grasper forceps inserted directly without a trocar below the costal margin, then the fundus of the gallbladder is ligated and lifted up with a folded zero-silk string and a 16-gauge vessel cannula. 9 These feasible, safe, and minimally invasive techniques result in a much smaller wound, with less pain than the conventional laparoscopic cholecystectomy, and is considered as an alternative way to deal with gallstone disease, especially for younger women, who tend to be more concerned about cosmetic outcome. 13 This study was undertaken to demonstrate the efficiency and safety of the Harmonic scalpel as the sole instrument to achieve complete hemobiliary stasis in the performance of laparoscopic cholecystectomy, with the use of the two-trocar technique.
Patients and Methods
Patient population
From January 2008 to July 2009, a sample of 160 cases of symptomatic gallstones were included in this study from unit C, General Surgery Department, Assuit University Hospitals (Assuit, Egypt).
Clinical and diagnostic workup
All patients were subjected to 1) full history taking, 2) clinical examination, and 3) investigations that included routine lab tests (i.e., blood count, random sugar, and serum creatinine), routine chest X-ray, electrocardiography, etc., liver function tests, prothrombine time, and abdominal ultrasonography. Additional investigations were needed sometimes, in some doubtful cases, such as computed tomography and magnetic resonance cholangiopancreatography.
Management
All patients were randomly assigned for laparoscopic cholecystectomy. Group 1 (the clipless Harmonic group) included 80 cases. The Harmonic scalpel was used as a single working instrument, with only two working trocars. Patients were positioned in an anti-Trendelenburg position, with some rotation to the left side to help in good visualization and manipulation of the gallbladder, if difficulty was still encountered. Thereafter, a curved Kirschner wire (1 mm) was introduced in the subcostal area and hooked the gallbladder fundus, with gentile retraction upward, or by the direct introduction of the laparoscopic trocar wound-closure forceps through the subcostal region, with gentle retraction of the gallbladder upward. However, these maneuvers were rarely resoled to during the work. An ultrasonic shear (Olympus Keymed Sono surg version G2 220–240 V 3A, 50/60 Hz; Tokyo, Japan) was used as the only working instrument during the procedure, through a 10-mm epigastric port, for the dissection and cutting of the cystic artery and duct. Then, gallbladder dissection from the liver bed was helped by a grasper, through the right midclavicular 5-mm port, to attain complete hemobiliary stasis. Last, the gall bladder was retrieved from the epigastric 10-mm trocar site.
Group 2 (the clip/cautery group) included 80 cases. The conventional instruments were used with the application of clips and the use of cautery in a three-working-trocar laparoscopic cholecystectomy technique. One small catheter drain was inserted in all cases, which was removed a few hours later. All patients were followed up in the General Surgery Department at Assuit University Hospitals, with the appropriate postoperative treatment in the form of broad-spectrum antibiotic prophylaxis, and analgesics, according to the amplitude of pain, using a “pain scoring system,” where a single shot of narcotics was sufficient to kill pain of a moderate type, but more doses were needed (double) with severe types of pain, 14 until being discharged from the hospital. The recording of all patient data was done and categorized as follows: intraoperative difficulty, intraoperative perforation of the bladder and biliary spillage, intraoperative injuries or complications, operative time, as well as postoperative complications, postoperative pain and the need for analgesics, and hospital stay.
Follow-up
Patients were followed up in the outpatient clinic for the detection of any complications, with an assessment of the cosmetic results and, also, patient satisfaction of the surgery.
Ethical considerations and informed consent
The study protocol was approved by the local ethical committee and was explained to each patient. All patients' informed consent was obtained prior to entry into the study.
Statistical analysis
Results were expressed as the mean ± standard deviation and number (%). Statistical analysis was performed with SPSS software (version 12; SPSS, Inc., Chicago, IL), using the Student's t-test to determine significance for numeric data and the chi-square test to determine signs for nonparametric data. The P-value was determined as significant if P < 0.05.
Results
Age and sex incidence in both groups
This study included 160 cases, most of whom were female (100; 62.5%), compared to males (60; 37.5%), with the male-to-female ratio at about 1:1.6. All data on age groups are shown in Table 1.
Duration of surgery
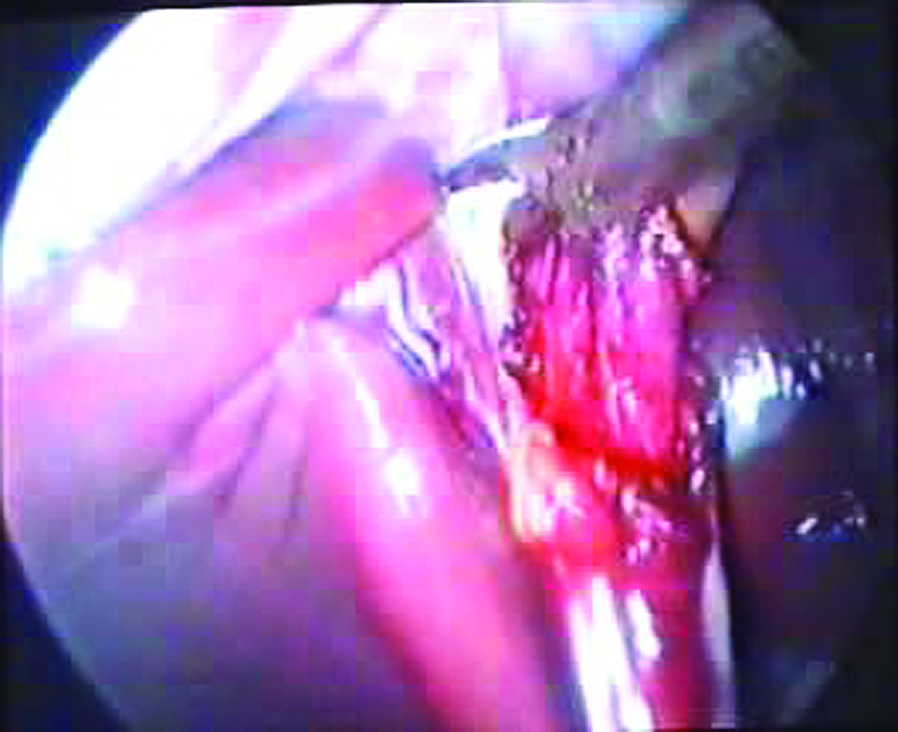
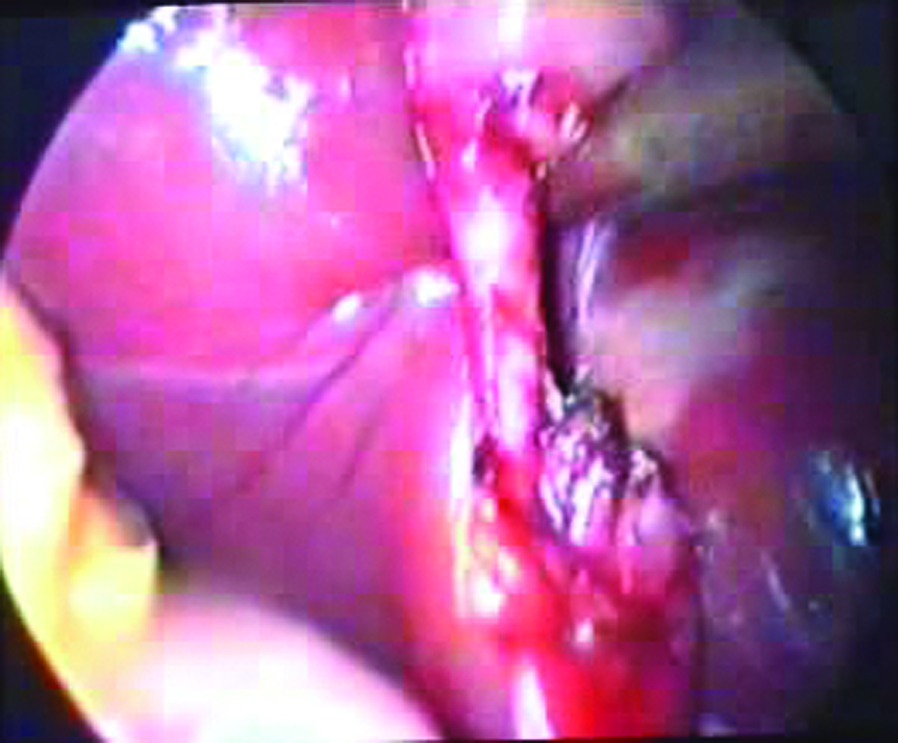
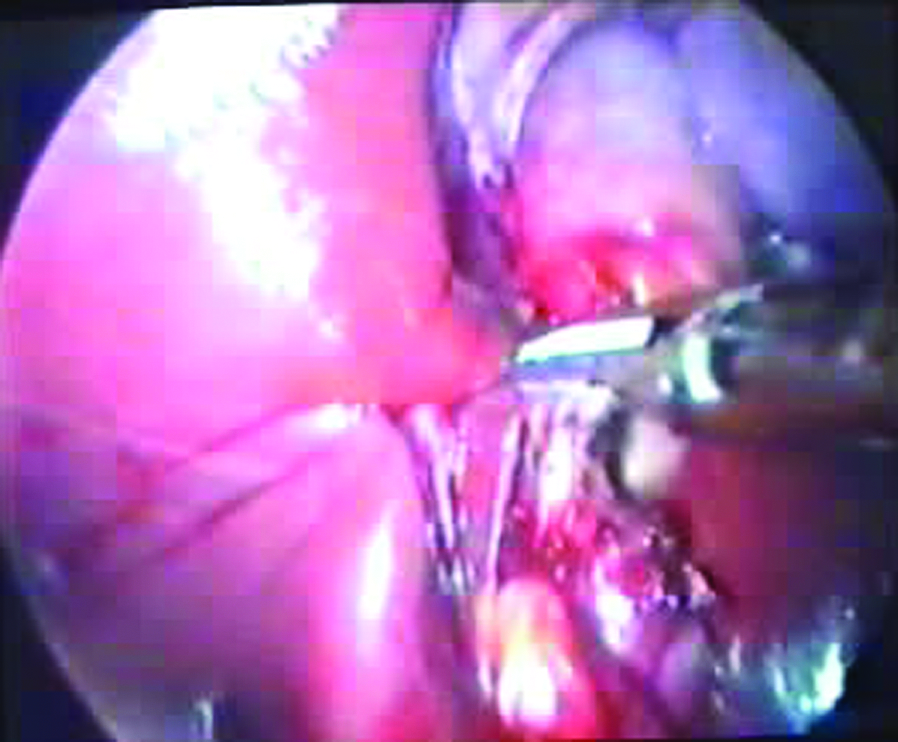
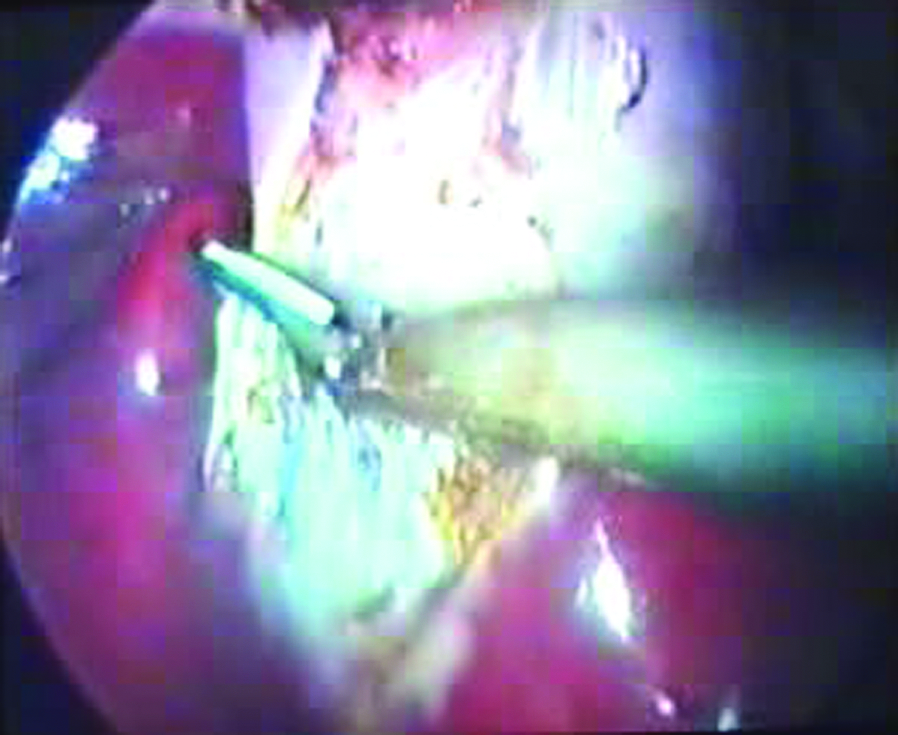
The surgical maneuver time was statistically significantly shorter in the Harmonic, compared to the regular laparoscopy, group, as shown in Table 2. Division of the cystic duct by Harmonic scalpel required approximately 2–3 minutes, depending on the ductal thickness and associated inflammation. In general, the cavitational effect on the surrounding pericholecystic tissues, especially in the region of the liver bed, allowed for easier mobilization of the gallbladder, thus avoiding inadvertent compromise of the gallbladder wall and bile spillage. No liver-bed charring or bilious seepage from any ducts of Luschka were observed (Figs. 1–10).

Harmonic scalpel and two working trocars.

Anterior dissection of the cystic artery.
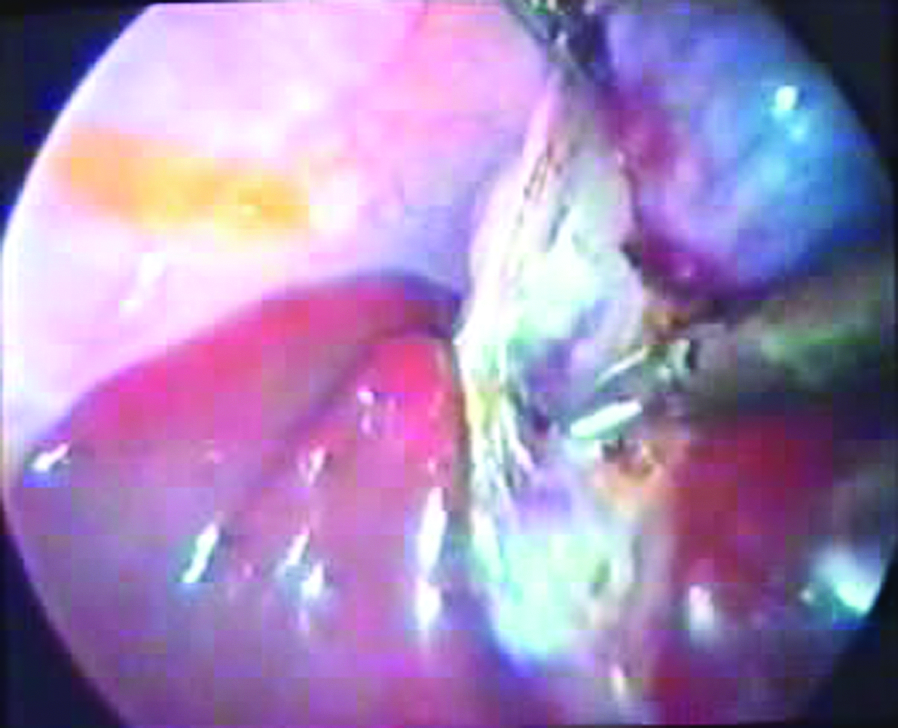
Posterior dissection.
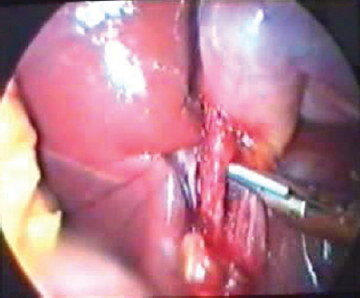
Harmonic coagulation and cutting of the cystic artery.
Skeletonization of the cystic duct.
Harmonic coagulation and cutting of the cystic duct.
Harmonic dissection of the gallbladder bed.
Dissection of the gallbladder from the liver at the fundus.
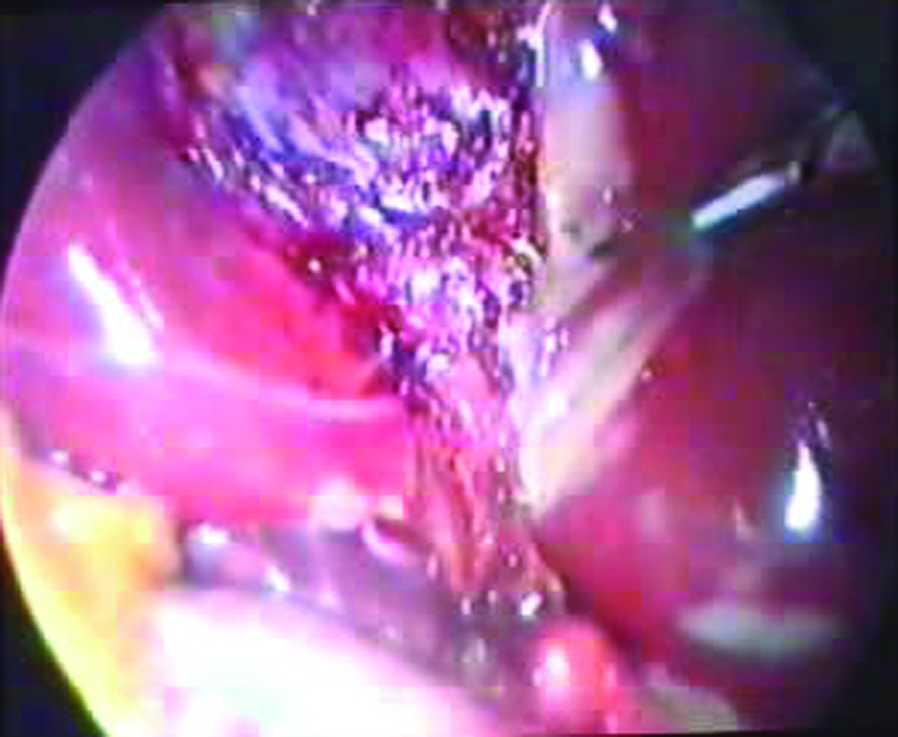
View of the gallbladder bed with complete hemobiliary stasis.

Postoperative view of the abdomen.
Highly significant.
SD, standard deviation.
Intraoperative complications
There was no statistically significant difference between the two groups regarding the incidence of intraoperative complications. However, there was a comparable incidence of intraoperative bile spillage (10 versus 13% for the Harmonic and regular laparoscopy groups, respectively), due to gallbladder perforation or leakage from its duct, with manipulation in acute cholecystitis and an obstructed, distended bladder. Also, a difficult maneuvering was seen in both groups in comparable incidences, due to distended, obstructed bladder in the Harmonic group (managed by repeatedly changing patient position) or acute cholecystitis in the regular laparoscopy group that was managed by meticulous maneuvers. Fortunately, no conversion to open cholecystectomy was encountered, as shown in Table 3.
Not significant.
Postoperative complications
There was only 1 case of postoperative bile soaking, which was treated conservatively, in the regular laparoscopy group. Postoperative pain occurred somewhat more frequently in the regular laparoscopy group, and, consequently, more doses of analgesic were needed than in the Harmonic group, as shown in Table 4.
Assessmet of pain and, consequently, narcotics was prescribed by a “pain scoring system” (see Reference 14).
Hospital stay
Hospital stay was statistically significantly shorter in the Harmonic group than in the regular laparoscopy group, as shown in Table 5.
Significant.
SD, standard deviation.
Follow-up
All patients were followed up in the General Surgery Department until being discharged for outpatient clinic follow-up, with meticulous monitoring of their satisfaction about the surgical maneuver and the cosmetic results, which were in favor of the Harmonic group more so than in the regular laparoscopy group.
Discussion
Cholecystectomy is a commonly performed operation for patients with symptomatic gallstone disease. 5 Laparoscopic cholecystectomy today is the standard operation, and it has given new impulses to surgery of the gall bladder and has been proven to be an effective, patient-friendly alternative to open surgery.15,16
Two-working-trocar technique
Many important advantages of laparoscopic surgery are produced by preservation of the integrity of the abdominal wall, including less operative trauma and complications, better recovery, and good cosmetic results. 10 Several attempts have been made to reduce operative trauma further by decreasing the number and size of the trocars, with the use of three trocars instead of four, and the use of mini-instruments is definitely a step in this direction.17,18 In this study, two working trocars were used in the Harmonic clipless group, instead of three working trocars as in the other group. Consequently, the harmonic two-working-trocars group had better cosmetic results and more patient satisfaction in follow-up, which is in agreement with the worldwide attention of minimal invasiveness seeking a further reduction of operative trauma, preservation of the integrity of the abdominal wall, with better recovery, and improved cosmetic results.9,10 The use of two working trocars, instead of three, is definitely a step in this direction, 11 with improvement of postoperative pain, return to activity and work, and better patient satisfaction. 8
Single working instrument
In this study, the Harmonic scalpel was used as a single working instrument not only to document the efficiency of a single working instrument, but also to evaluate its use in dissection and achieving hemobiliary stasis. As agreed on by Nicholas Marshall, a single instrument means avoidance of repeated instrument changes during the procedure, and selecting different instruments breaks the natural flow of the operation and may distract the surgeon. 5
Harmonic scalpel uses
This study clearly demonstrates that the Harmonic scalpel provides complete, reliable hemobiliary stasis without clinically significant immediate or remote postoperative complications, as evident from studies by other researchers. 19 It was feasible, easily handled, and very efficient. As stated by Westervelt, 19 the use of the Harmonic scalpel did not adversely affect the length of the procedure; moreover, it significantly shortened operative time, and this was proven in our work (20 vs. 45 minutes, respectively, for Harmonic and regular laparoscopy; P = 0.0001). In fact, the properties intrinsic to the Harmonic scalpel (i.e., cavitations and smokeless coagulation) seem to provide an advantage over electrocautery in the dissection of the gallbladder and may enhance surgeon performance,1,6,19 which is in agreement with other researchers, that its application shortens operative time. 8 Moreover, the Harmonic scalpel division of the cystic duct could be utilized independently of the direction of the gallbladder dissection with effective hemobiliary stasis. 1
Intraoperative bile spillage was slightly trended more downward in the Harmonic group than the regular clip/cautery group (10 versus 13%, respectively; P = 0.46). There was no intraoperative blood soaking, in comparison to 1 case from the regular laparoscopy group, and this may be attributed to the effectiveness of the Harmonic scalpel in gallbladder dissection with hemobiliary stasis. The small incidence of bile spillage encountered in the Harmonic group was not due to gallbladder perforation, but was attributed to the early experience with the device without efficient closure of the cystic duct; hence, it was seen only in the initial cases. Most researchers denote that Harmonic clipless cholecystectomy is associated with a significantly lower incidence of gallbladder perforation and bile spillage.2,3,19
Postoperative complications
One patient suffered from postoperative bile leakage, from the regular laparoscopy group, and was treated conservatively. But, no major postoperative complications or injuries were encountered in either group. This proved the effectiveness of the Harmonic scalpel to prevent bile leakage from the liver bed that may contribute to postoperative pain, small bilomas, and the associated return to the operative room, as documented by Nazih and others1,2,6,19,20; hence, patients in the Harmonic group suffered less postoperative pain, with the need of a single dose of analgesics postoperatively, in comparison to the regular laparoscopy group, who needed double that dose.
Hospital stay
In this study, hospital stay was statistically significantly lower in the Harmonic than in the regular clip/cautery group (1 vs. 1.5 days, respectively; P = 0.001). But this is not a solid document, as it may have been biased by the nonblinded format of the study groups. However, it is in agreement with data documented by other researchers, that Harmonic scalpel clipless cholecystectomy decreases hospital stay.1,5,19 Despite Tsimoyiannis 21 having demonstrated comparable recovery times, subjective observations throughout this study do not substantiate this finding.
Conclusions
The Harmonic scalpel is a safe, efficient, and practical instrument to use during laparoscopic cholecystectomy, especially if used as a sole working instrument, with complete hemobiliary stasis. Its application shortens operative time and decreases accidental bile spillage; consequently, it decreases postoperative complications and may shortens length of hospitalization. Downsizing the number or size of laparoscopy trocars improved the results of minimal invasiveness that may lead to better recovery, less pain, improved cosmesis, and better patient satisfaction.
Footnotes
Disclosure Statement
No competing financial interests exist.