
Abstract
Abstract
Robotic surgery represents one of the most advanced developments in the field of minimally invasive surgery. In this article, we describe the case of an extended right hepatectomy with a left hepaticojejunostomy performed for radical resection of a hilar cholangiocarcinoma. This operation was performed by using the da Vinci® Robotic Surgical System (Intuitive Surgical, Sunnyvale, CA). In this case, the operative time was 540 minutes, with an intraoperative blood loss of 800 mL. The postoperative course was uneventful, and the patient was discharged at postoperative day 11. This report confirms the technical feasibility and safety of robot-assisted extended hepatic resections with biliary reconstruction. Further experience and a long follow-up are required to validate this initial report.
Introduction
Case Report
A 66-year-old man presented with a 1-month history of painless jaundice and significant weight loss. An abdominal ultrasound showed dilatation of the intrahepatic bile ducts. An endoscopic retrograde cholangiopancreatography (ERCP) was performed, which identified a hilar bile duct stricture. A 10-Fr biliary stent was then inserted, resulting in clinical and biochemical improvement of the jaundice. Cytologic brushing revealed a well-differentiated cholangiocarcinoma. The patient was referred to our hospital after 2 weeks for further evaluation. We performed percutaneous left internal/external biliary drainage, because the biliary stent that was previously placed endoscopically was obstructed (Fig. 1A). Computed tomography (CT) and magnetic resonance imaging of the abdomen showed an absence of hilar vessel infiltration and distant metastases. After careful preoperative clinical risk assessment, a curative resection, by an extended right hepatectomy and main bile duct resection, was planned. Since the left liver lobe volume was insufficient, a percutaneous right portal vein embolization was performed (Fig. 1B). After 4 weeks, a three-dimensional (3D) CT scan for liver-volume evaluation showed satisfactory left lobe liver hypertrophy. Total liver volume was 1244 cc, left lobe volume was 531 cc, and the patient's weight was 61 kg. After obtaining informed consent, the patient underwent surgery.

Patient preparation before surgery. (
Surgical technique
Under general anesthesia, the patient was placed supine with parted legs, with a 20-degree reverse-Trendelenburg adjustment. A Verres needle was inserted into the left hypocondrium in order to insufflate the abdomen to 12-mm Hg pneumoperitoneum. A 12-mm trocar was placed at the umbilicus. Following preliminary laparoscopic exploration, four additional trocars were introduced for the robotic instruments and camera, as shown in Figure 2. The assistant surgeon was positioned between the patient's legs to perform complementary maneuvers (i.e., suction, stapling, retraction, and laparoscopic ultrasonography) through the 12-mm port at the umbilicus.

Port placement for robotic extended right hepatectomy.
The da Vinci® Robotic Surgical System (Intuitive Surgical, Sunnyvale, CA) was placed at the patient's head, and the arms were docked to the ports. Intraoperative ultrasonography was performed to confirm the absence of undetected liver metastases. Initially, the hepatic flexure of the colon was mobilized with the Harmonic dissector, and a partial Kocher maneuver was performed. Starting at the superior border of the pancreatic head, a lymphadenectomy of the common hepatic artery was performed, using a monopolar hook and bipolar forceps, to expose the origin of the gastroduodenal artery. The inferior aspect of segment IV was retracted upward by using the fourth robotic arm, and the common bile duct (CBD) was dissected and sectioned at the superior border of the pancreatic head. The distal stump of the CBD was sutured, and a frozen section at this level showed the absence of neoplastic invasion (Fig. 3A). The right hepatic artery was dissected and divided at its origin from the proper hepatic artery between ligatures, then transfixed with polypropylene 4/0 sutures (Fig. 3B). The dissection reached the left hepatic duct, which was transected at the left umbilical fissure (Fig. 3C). A frozen section performed at this level confirmed the absence of neoplastic invasion.
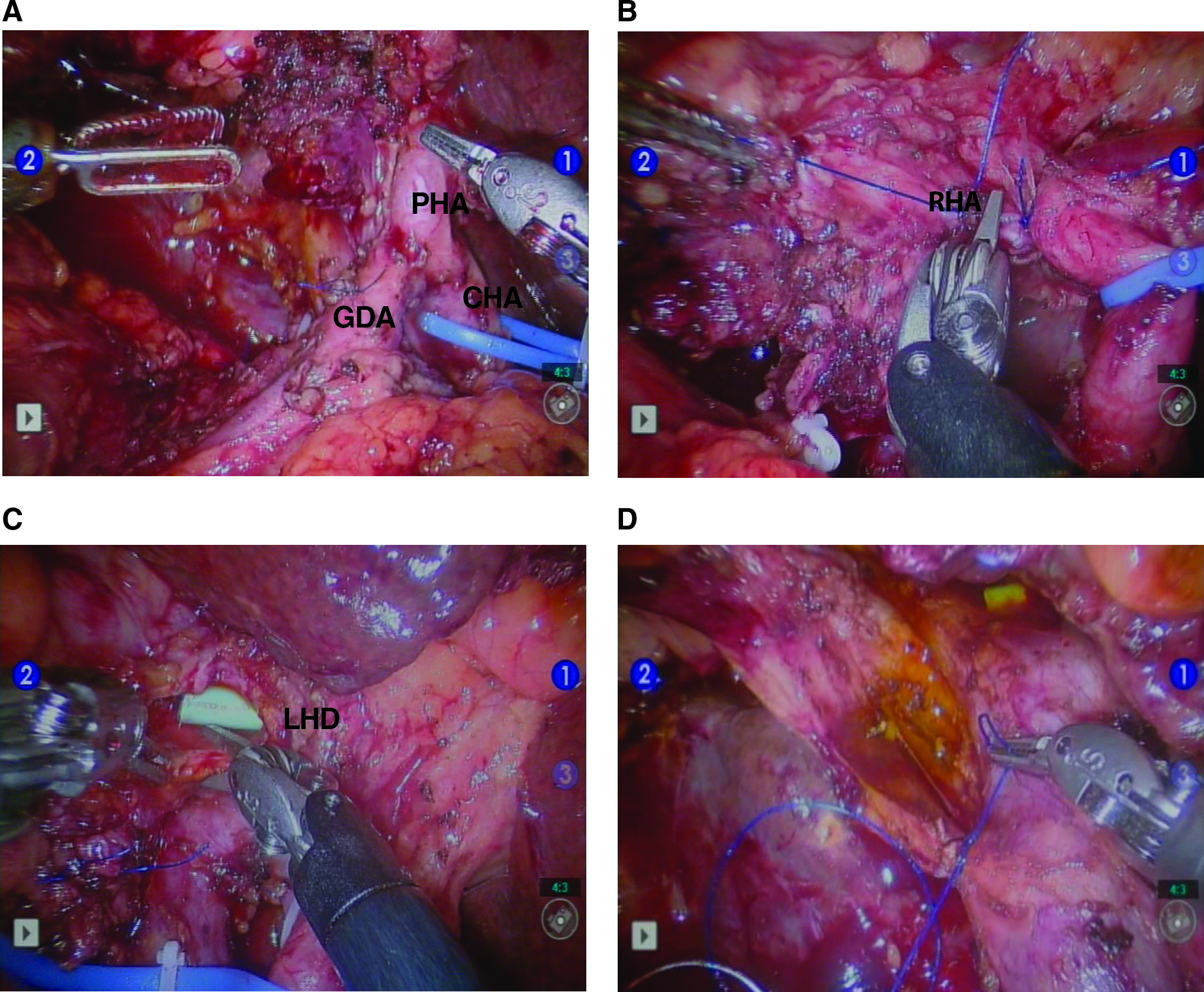
Intraoperative view of hepatic pedicle dissection: (
Following this, the two separate right portal branches were dissected, divided between ligatures, and transfixed with polypropylene 4/0 sutures (Fig. 3D). The right liver lobe was then mobilized from its peritoneal attachments. This was done by sectioning the falciform ligament and the anterior half of the coronary ligament, until the anterior side of the inferior vena cava (IVC) and the right hepatic vein was reached (Fig. 4A). The hepatorenal ligament and the right triangular ligament were then divided by using a monopolar hook. The fourth arm was used to retract the inferior aspect of the right liver lobe upward. In this way, the right side of the IVC was exposed. The accessory hepatic vein was suture-ligated with 4/0 polypropylene sutures, and the dissection proceeded until the inferior aspect of the right hepatic vein was reached (Fig. 4B).

Intraoperative view of vena cava dissection and parenchymal transection. (
After sectioning the bridge of parenchyma between segments IV and III, the parenchymal transection was carried out along the right aspect of the falciform ligament by the robotic Harmonic scalpel (Intuitive Surgical), starting at the anterior border of the liver (Fig. 4C). The recurrent vessels from the umbilical fissure to segment IV were divided with a 45-mm white-cartridge laparoscopic stapler (Ethicon, Endo-Surgery, Cincinnati, OH) (Fig. 4D). Metallic clips and 4/0 prolene sutures were used for the hemostasis of minor bleeding. The middle hepatic and right hepatic veins were then divided intraparenchymally, using a 45-mm white-cartridge laparoscopic stapler (Ethicon, Endo-Surgery).
The specimen was placed in a plastic endobag, and the pneumoperitoneum was stopped. The robotic cart was then removed from the operative field. A 7-cm midline was performed, through which the hepatectomy specimen was retrieved. A segment of the proximal jejunum was exteriorized, and a Roux-en-Y anastomosis was performed 40 cm distal to the ligament of Treitz. The pneumoperitoneum was restarted after the bowel was repositioned into the peritoneal cavity, and the da Vinci robot was docked to the ports. After passing the constructed loop via the antecolic route, a left hepaticojejunostomy was performed with robotic instruments and two running sutures of PDS 4/0 (Ethicon, Endo-Surgery) (Fig. 5). The remnant left liver was fixed in its anatomic position by suturing the falciform ligament. The resection surface was then inspected for bile leaks, and surgical glue was applied. Two closed-suction subphrenic drains were placed in the subhepatic and -diaphragmatic areas.

Intraoperative view of robotic left hepaticojejunostomy.
Results
The surgery lasted 540 minutes, with an intraoperative blood loss of 800 mL. One unit of red blood cells was transfused. The patient was transferred to the intensive care unit for postoperative care and, subsequently, to the general ward on postoperative day 3. An intestinal transit was recovered on postoperative day 3, and an oral liquid diet was reintroduced. Intravenous administration of analgesic was necessary until postoperative day 3, as well. Histopathologic examination demonstrated a moderately differentiated 22-mm cholangiocarcinoma on the hilar bile duct confluence extending into the right hepatic duct without lymph node metastases (T2N0). The margins of the resection were free of tumor. The postoperative course was uneventful, and the patient was discharged on postoperative day 11. At 8 months of follow-up, the patient is alive and has had no recurrence of this disease.
Discussion
Extended liver resections in conjunction with extrahepatic bile duct resection, lymphadenectomy, and, sometimes, portal vein resection represent the gold standard of treatment for resectable hilar cholangiocarcinoma. This “aggressive” surgical strategy has increased the rate of curative resection and long-term survival of patients affected by this disease.10,11 The adoption of laparoscopy for liver resections has gained acceptance worldwide as the safety, feasibility, and advantages of this approach for resection of the anterior and lateral segments of the liver have been reported.12–14 Technical limitations and oncologic concerns, however, have hindered the use of laparoscopy for the treatment of biliary malignancies. Initial studies on incidental gallbladder carcinomas have shown a poor outcome for patients operated on laparoscopically, as compared to those who underwent open cholecystectomy.5,6 Other reasons contributing to the less-than-widespread use of laparoscopy for the treatment of biliary malignancies is the fact that major liver resections are considered technically demanding laparoscopically. 15
The main challenges encountered during laparoscopic major hepatectomies have to do with the hepatic hilum dissection, right lobe mobilization, proper section-line exposition, and safe, effective bleeding control during parenchymal transection.16,17 Moreover, the necessity of a complex biliary reconstruction adds an additional challenge to this procedure, when performed laparoscopically. 18 Robotic surgery offers significant advantages over laparoscopy. Specifically, the da Vinci robotic system enables the surgeon to have 3D stereoscopic visualization, intuitive finger-controlled movements, and EndoWrist technology. This translates into more careful, precise dissection of fine structures and superior dexterity in knot tying and suturing.
Based on our previous experience with robot-assisted hepatic resections (more than 70 resections performed, to date), we felt confident in applying this approach in the case presented in this report. The intervention was well planned, allowing for optimal preparation of the patient before surgery, and included left percutaneous biliary drainage and preoperative portal vein embolization to achieve sufficient left-liver remnant. During the operative procedure, a laparoscopic exploration was performed first in order to confirm the absence of undetected metastases. 19 In this case, we used a limited abdominal incision for the extraction of the specimen and the construction of a Roux-en-Y loop to speed up the procedure. The bilioenteric reconstruction was performed with robotic instruments on a bile duct of a small caliber.
The increased degree of freedom of the instruments, combined with magnified 3D vision, made it easy to perform an anastomosis, as had been previously experienced for biliary reconstruction during duodenopancreatectomy. The postoperative course was uneventful. The patient had an early recovery of intestinal transit, a low need for analgesic medications, and an early oral feeding. We believe, however, that increased experience with this specific procedure can further reduce the length of postoperative stay, which, in this case, was relatively long for a minimally invasive procedure.
Conclusions
This report suggests that, in experienced hands, a robot-assisted extended right hepatectomy with a biliary reconstruction is safe and feasible. This approach can reduce the morbidity correlated with open liver surgery in the case of extended liver resections. Large, prospective studies will be necessary to see the benefit and results of this approach over open surgery for hilar biliary malignancy.
Footnotes
Disclosure Statement
No competing financial interests exist.