
Abstract
Abstract
Background:
Laparoscopic resection of gastric gastrointestinal stromal tumor (GIST) has been shown as feasible and safe in terms of oncologic results. However, laparoscopic resection has been demonstrated to be mainly suitable for small, favorably localized GIST. The robotic approach may, by its characteristics, enable the surgeon to perform atypical gastrectomies in an unfavorable location (i.e., close to pylorus or cardia). Its use in oncologic gastric surgery has been poorly defined and has never been reported for GIST.
Materials and Methods:
All patients who underwent robotic-assisted gastric resection for GIST at a single institution from 2006 to 2009 were prospectively followed-up.
Results:
There were 5 patients (3 men and 2 women), with a median age of 39 years (range, 32–74), who had a complete resection (R0). Two patients had a cardial GIST and 3 of the antrum. Median tumor sizes were of 5.5 cm (range, 4.2–7). According to Fletcher criteria, 4 tumors (80%) were classified as intermediate or high risk. No postoperative morbidity and mortality were noted. One patient had a conversion to open surgery because of a suspicion of diffuse adenocarcinoma on fresh frozen section and necessitated a total gastrectomy with a radical lymph node dissection. Median operation time was 192 minutes (range, 132–285). With a median follow-up of 18 months (range, 11–27), disease-free survival rate was 100%.
Conclusions
: The da Vinci® robot (Intuitive Surgical, Inc., Sunnyvale, CA) is a valuable instrument for oncologically safe resection with esogastric or duodenogastric junction preservation for an unfavorably located gastric GIST. Moreover, the three-dimensional, high-definition vision, instrument mobility, and ease of performing a difficult suturing enable a safe, large atypical gastrectomy, close to the pylorus or cardia.
Introduction
Laparoscopic resection of gastric GIST has been shown to be feasible by many researchers.10–18 However, some limitations to laparoscopic resection for GIST have been quite uniformly recognized and moved the National Comprehensive Cancer Network (NCCN) to edit guidelines for laparoscopic GIST resection. 19 Among them, GIST size may be a limitation for laparoscopic resection, and the NCCN recommends it for tumors of less than 2 cm.9,18,20–23 Thus, laparoscopic resection of gastric GIST has been shown to be suitable, but only for small, favorably localized tumors.
Robotic surgery is gaining increasing acceptance as a therapeutic tool for visceral surgery. Recently, robot-assisted gastrectomy, with radical lymph node dissection for gastric cancer, has been demonstrated as feasible and safe.24–26 However, the use of a robot in gastric GIST surgery has not been defined and has never been reported for these tumors, so far. The aim of this prospective study was to evaluate surgical and oncologic outcomes of these patients.
Materials and Methods
Patients
This prospective cohort study consisted of patients suffering from gastric GIST, who were treated by robotic surgery (da Vinci®; Intuitive Surgical, Inc., Sunnyvale, CA) at the Department of Surgery, University Hospital of Geneva (Geneva, Switzerland) from 2006 to 2009. Histologic diagnosis of all tumors was confirmed by pathologists of the Department of Pathology, Medical University of Geneva. According to Fletcher criteria, 27 tumors of less than 2 cm in diameter and with a mitotic count (MC) of less than 5 of 50 high-power fields (HPFs) were classified as very low risk. Low risk was identified when size ranged from 2 to 5 cm and the MC was less than 5 of 50 HPFs, intermediate risk when tumor size was less than 5 cm and 6–10 MC of 50 HPFs or the tumor size was 5–10 cm and the MC less than 5 of 50 HPFs, and high risk was determined when tumor size was greater than 10 cm or the MC was greater than 10 of 50 HPFs or the tumor size was greater than 5 cm and the MC was greater than 5 of 50 HPFs. All data were collected prospectively. Operative time was calculated as the time between skin incision and port-site closure.
Operative techniques
The patient was placed in the supine position, with the main monitor above the right shoulder. A 12-mm Hg pneumoperitoneum was established by using the open technique. A 12-mm camera port was placed just above the umbilicus. Two 12-mm trocars for the robotic arms were placed under direct visualization two to three fingerbreadths below the costal margin at the right and left midclavicular line, respectively (Fig. 1), at least one handbreadth away from the camera port. The 12-mm service port for the assistant was placed one handbreadth left away from the left port. The liver retractor was placed in the epigastric area. After placing the ports, the patient was moved to about a 20-degree reverse Trendelenburg position. The robot was then docked over the patient's left shoulder.
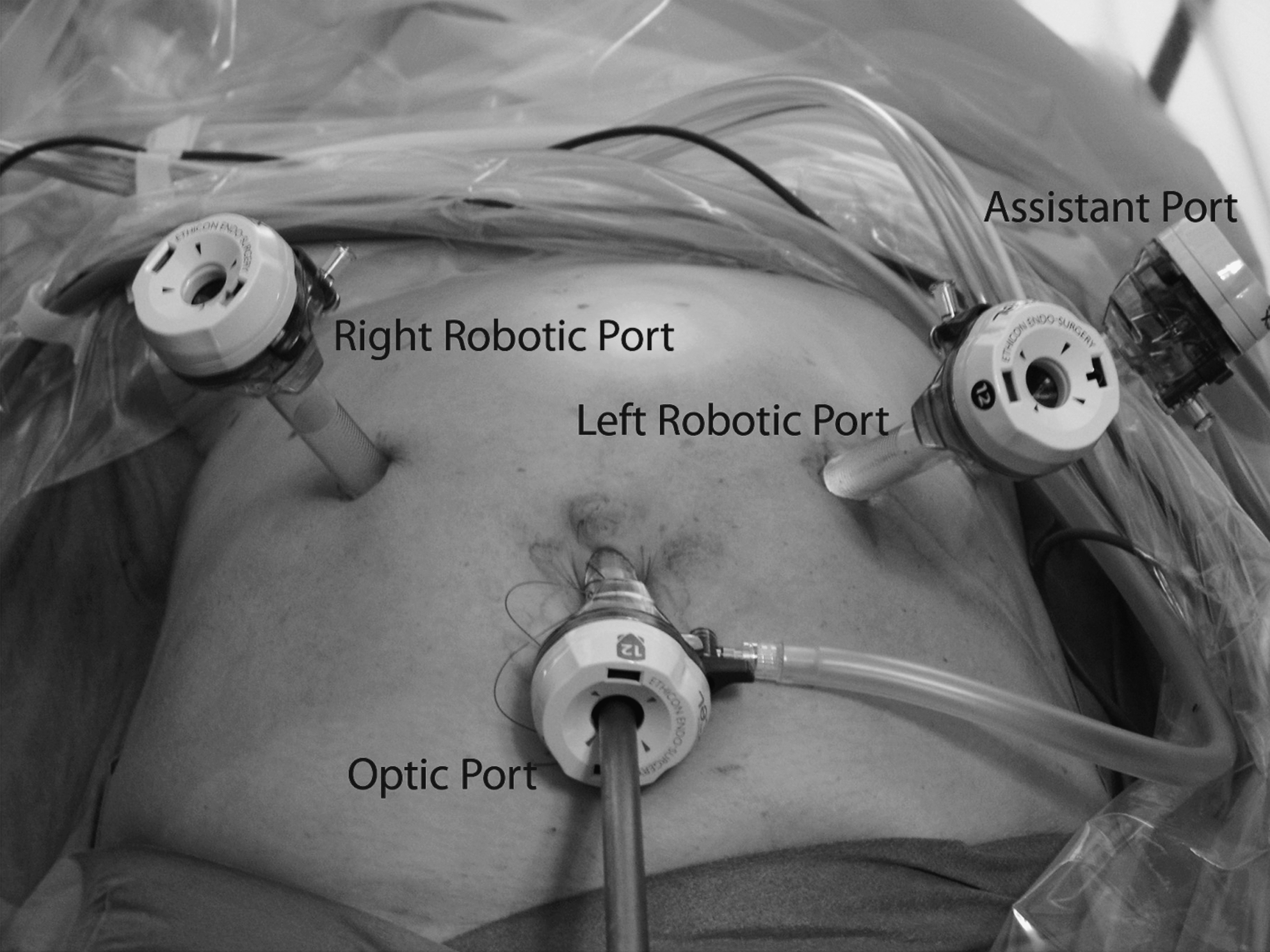
Operative port placement and robot disposition in the operating room.
The tumor was then identified. When it was not obvious, a peroperative gastroscopy was performed by a gastroenterologist to localize the tumor by translumination. The tumor was then dissected by a transgastric approach, using a Harmonic Scalpel (Ethicon Endo-Surgery, Inc., Cincinnati, OH), with at least 1–2 cm of margin (Fig. 2). The specimen (Fig. 3) was removed by using a large specimen bag introduced through the 12-mm service port. The stomach was closed with a single-layer running suture (Fig. 4). No drain was left in place routinely. Ports were then closed.
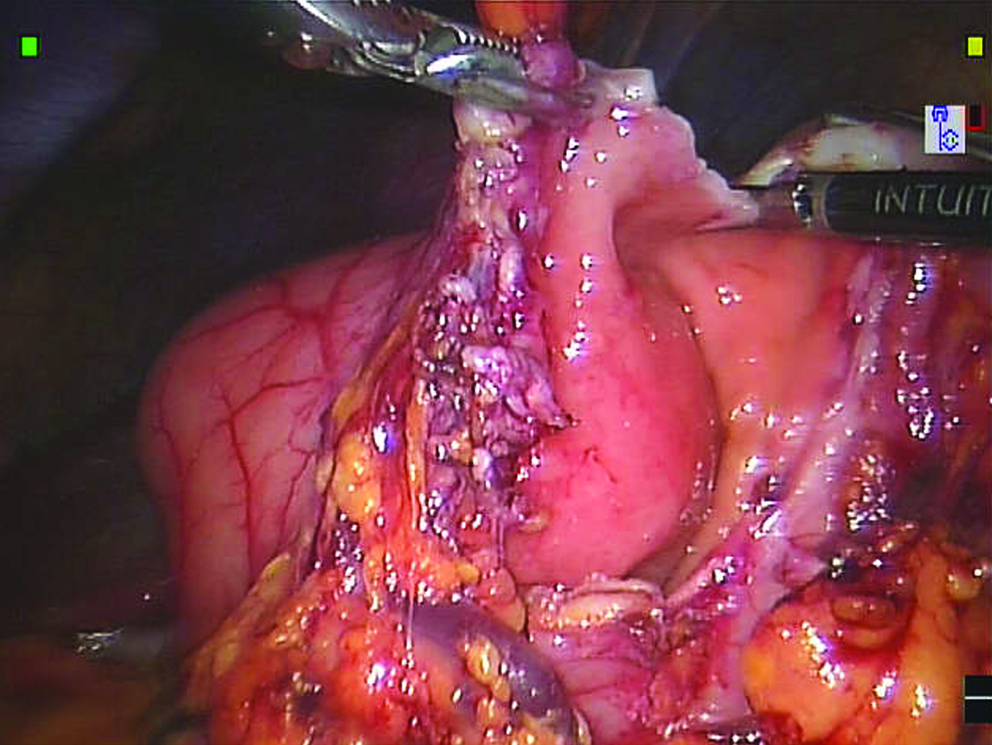
Transgastric approach, using the Harmonic Scalpel (Ethicon Endo-Surgery, Inc., Cincinnati, OH), with dissection of the GIST located in the posterior wall of the stomach.

The specimen (diameter, 7 cm) with a margin of a minimum of 1 cm all around.
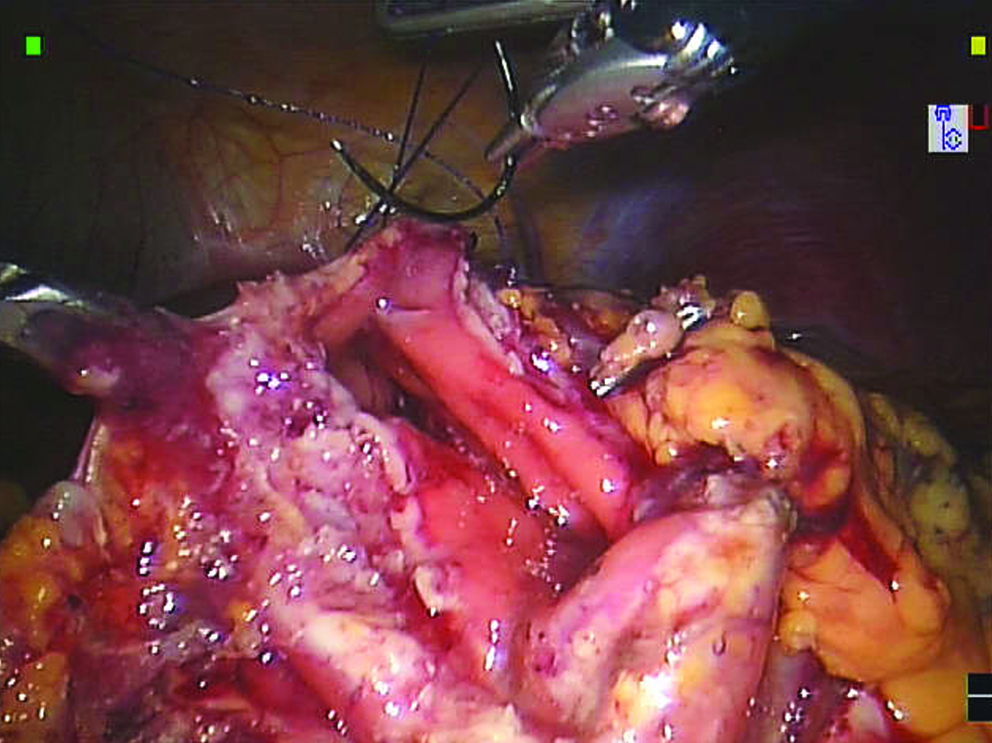
Closure of the stomach, using a single-layer running suture.
Follow-up
All patients who underwent robotic treatment of gastric GIST were prospectively followed-up between May 2006 and August 2009. Follow-up was carried out through routine visits at our outpatient oncological clinic. Investigations consisted of gastroscopy, computed tomography, and, eventually, positron emission tomography.
Results
From May 2006 to August 2009, 5 consecutive patients underwent robotic surgical resection of gastric GIST (Table 1). There were 3 men (60%) and 2 women. Median age was 39 years (range, 32–74). No patient received preoperative treatment with the tyrosine kinase inhibitor, imatinib. The tumors were located in the distal antrum (n = 3) and in the cardia/gastroesophageal junction (n = 2). The procedures performed were 4 partial gastrectomies with nonanatomic wedge resections. One patient had a conversion to open surgery because of a suspicion of a diffuse adenocarcinoma on fresh frozen section, and necessitated a total gastrectomy with a D2 lymph node dissection. Finally, histopathologic analysis revealed a high-grade GIST.
Because of a suspicion of a diffuse adenocarcinoma on fresh frozen section.
OR, operative time in minutes; R0, complete resection; LOS, length of stay in days; FU, follow-up in months.
Every patient had a complete resection (R0). There were no episodes of tumor rupture or spillage during the operations. According to Fletcher criteria, 4 tumors (80%) were classified as intermediate or high risk. Median tumor sizes were of 5.5 cm (range, 4.2–7). The median operation time was 192 minutes (range, 132–285), after the exclusion of the converted patient.
No postoperative morbidity and mortality were noted—in particular, no bleeding and no leaks. No patient experienced an anastomotic stricture. The median length of stay was 7 days (range, 5–10). Follow-up was complete in 100% of patients. With a median follow-up of 18 months (range, 11–27), disease-free survival rate was 100%.
Discussion
The current study was a case series of 4 patients undergoing a totally robotic gastric resection for GIST with promising short- and middle-term outcomes. The robot is a useful instrument to facilitate traditional laparoscopic procedures, allowing complex, advanced operations to be carried out with a minimally invasive approach. While, recently, several studies have shown that robot-assisted laparoscopic gastric resection with D2 lymph node dissection was feasible and safe,24–26 so far, its use in oncologic resection for gastric GIST has not been reported, to our knowledge. For several years, laparoscopic resection of gastric GIST has been shown to be feasible by many researchers.10–18 However, some limitations of laparoscopic resection for GIST have been quite uniformly recognized, and this approach has been demonstrated to be suitable only for small, favorably localized tumors.9,18–23 With the laparoscopic approach, for a large or unfavorably placed GIST, it could lack instrument mobility and the suturing becomes too difficult for the procedure to be performed. In this study, we have shown that image magnification, tremor filtering, and fine robotic arm movements could help to perform a large gastric GIST resection, without complication and no recurrence at 18 months. Because certain tumor localization may limit laparoscopic resection, 10 other studies demonstrated that conversion to an open approach is more likely to occur in patients with a tumor near the gastroesophageal junction.18,28
Whatever the technical therapeutic option chosen, surgery should be radical, without intra-abdominal dissemination. 5 Robotic-assisted resection could help to obtain a margin-free specimen. A 1–2 cm margin was thought to be necessary for an adequate resection.9,29 In our study, we were able to achieve a complete R0 resection, in each case, with good margin. Although it is difficult to demonstrate a clear, real advantage for patients over laparoscopic surgery, 30 we strongly think that the robot-assisted gastric resection for GIST could help the surgeon to perform a difficult suturing and dissection. Moreover, it could help to accomplish the large wedge gastrectomy, with preservation of pylorus or cardia, for unfavorably placed large tumors. In general, robotic surgery is reported to require a longer operative time than conventional surgery (open or laparoscopic). 25 The prolonged operative time is caused by the additional setting time for the robotic arms. 30 However, in this report, the total operative time averaged 192 minutes, which compared relatively favorably with the most recent literature for laparoscopic resection (range, 92–180).12,14,15–18
In 2003, Walsh et al. 31 published their initial clinical experience with 13 gastric GIST resections, using a percutaneous endoluminal technique. The surgical results and short-term outcomes were good. This technique is probably a step toward natural orifices transluminal endoscopic surgery (NOTES) procedures, but data are still limited, and the real application for large, unfavorably placed gastric GIST still remains unclear. Recently, Nakajima et al. 32 reported their initial clinical experience of NOTES partial gastrectomy for GIST in 2 women. They showed that it was feasible and safe, but it remained complex and challenging. However, the tumors were quite small (i.e., 4 and 3 cm) and relatively well placed (i.e., anterior antrum and posterior corpus). Finally, the tumors were stapled by a transvaginal approach in these two small women (159 and 149 cm), which could be more difficult in the taller patient.
Another team reported the intragastric approach for GIST located at the posterior gastric wall in 3 cases. 33 The tumors were again small (i.e., 2–4 cm), and an R0 resection was achieved in each case. However, this technique may be useful only for posterior and relatively small GIST, as Privette et al. 14 proposed, too. Hiki et al. 34 reported a cooperative technique between laparoscopic and endoscopic surgery, with good results. However, it is too early to generalize these interesting new techniques.
This study had a couple of limits, which deserve some comments. First, the sample was small, with 5 patients enrolled and only 4 who underwent the totally robotic procedure. However, so far, this is the first series to report the safety and feasibility of a robotic wedge gastrectomy for gastric GIST. Moreover, the oncologic results are promising after 18 months of follow-up, without any recurrence. Indeed, all patients benefited from a R0 resection. Then, although this study was not designed to compare the laparoscopic and the robotic approach, we recommend the use of the latter for large, unfavorably localized tumors. We strongly think that the capacities of the robot can help the surgeon to perform suturing in difficult-to-reach areas, such as close to the pylorus or the cardia.
Conclusions
In conclusion, the da Vinci robot is a valuable instrument for the oncologically safe resection of the large gastric GIST. Moreover, the three-dimensional, high-definition vision, instrument mobility, and ease of performing difficult suturing enable a safe, large wedge gastrectomy, pylorus, or cardia preserving resection in an unfavorably placed large gastric GIST. However, long-term oncologic outcomes and experience from other institutions are necessary to determine the exact role of robot-assisted surgery in gastric GIST and to compare this promising new approach to the classical one (i.e., laparoscopic or open).
Footnotes
Disclosure Statement
No competing financial interests exist.