
Abstract
Abstract
Background:
Laproscopic single-site surgery is the natural evolution of minimally invasive surgery.
Methods:
A 70-year-old male was planned for a resection of a gastric GIST (gastrointestinal stromal tumor). A Triport® trocar (Olympus, Aartselaar, Belgium) was placed through a 2-cm periumbilical incision. Besides the placement of a Nathanson liver retractor in the subxiphoidal position, no additional trocars had to be added. The partial gastrectomy was carried out by using clinical prototypes of double-bended intruments and of a “goose neck” videolaparoscope, all specially designed for single-port surgery.
Results:
Total operative time was 140 minutes, and estimated blood loss was 10 mL. No intra- or postoperative complications occurred. Hospital stay was 4 days. Final pathology revealed the complete resection of a GIST tumor of gastric origin.
Conclusions:
We have demonstrated the technical feasibility and described the detailed surgical technique of laparoendoscopic single-site surgery gastric wedge resection.
Introduction
Clinical Case
A 70-year-old man presented with several episodes of nausea, vague abdominal discomfort, and mild acid reflux. His past medical history only revealed hyperlipidemia, and the physical examination was unremarkable. During the workup, an esophagogastroduodenoscopy showed a 2-cm pedunculated mass along the posterior wall of the mid-body of the stomach. Ultrasonography showed that the origin of the tumor was in the submucosa. A computed tomographic (CT) scan of the abdomen visualized the mass in the stomach, but did not reveal additional lesions in the abdomen or pelvis (Fig. 1). In our department, the resection of small gastric GIST is routinely performed laparoscopically, with the use of four laparoscopic ports and the enlargement of one of the port sites for the extraction of the tumor. Given our experience with LESS in bariatric and colorectal disease, we proposed to resect the GIST by using this single-port approach. The patient was informed of the characteristics of the LESS procedure and other surgical options, including laparoscopic, as well as the possibility of requiring a conversion to an open procedure. The clinical application of this technique was reviewed by the local Ethical Committee, according to the declaration of Helsinki.
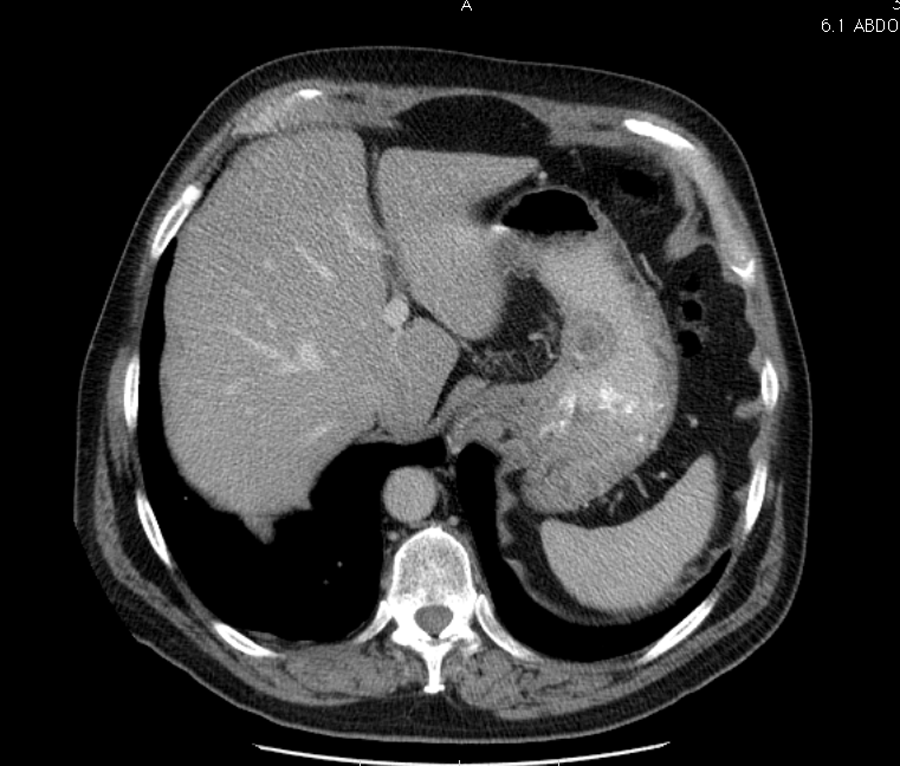
Transverse CT scan shows an endoluminal gastric stromal tumor.
Surgical procedure
The patient was administered general anesthesia and positioned in the French position. Antibiotic prophylaxis was given intravenously (second-generation cephalosporine) during induction. Preemptive analgesia was applied on a periumbilical field of 5 × 5 cm, using ropivacain (7.5%). A 2-cm semicircular incision was made at the superior edge of the umbilicus. The three-channel Triport® (Olympus, Aartselaar, Belgium) trocar was inserted and fixed before connecting it with the insufflator (Fig. 2). This flexible trocar was specifically designed for single-site surgery and consisted of a flexible inner ring, contained by a double-layered flexible tube with a diameter of 5 cm. The top and outer part of the trocar counted two 5- and one 12-mm gelports. The top was detachable and allowed the insertion and extraction of tissues or devices without contamination of the wound edges. The insufflator was connected to one of the two insufflation channels, and, under a working pressure of 15 mm Hg, the “goose neck” 5-mm 30-degree videolaparoscope was inserted in one of the 5-mm gelport channels. The “goose neck” is a prototype for clinical use and was provided by Olympus (Hamburg, Germany). The name refers to the long, bendable connection between the optic and the camerahead and makes it possible to prevent the collision of the camera with the instruments (Fig. 3). For the actual handling of the organs, we used clinical prototypes of instruments constructed with a double bend. One bend was made at the level of the intraperitoneal part and one at about 10 cm before the instruments' end up in the handle. The opposite bending of the right- and left-handed instruments maked it possible to perform manipulations in a very intuitive way, with minimal conflict between the instruments passing through the single hole. The Nathanson liver retractor was placed in the subxyphoidal position through a 5 mm incision. The visualisation of the tumor was possible after the opening of the lesser sac trough the gastrocolic ligament. The tumor was localized in the posterior wall of the body of the stomach. A anterior longitudinal gastrotomy was made with the 5 mm Sonosurg (Olympus, Belgium) harmonic dissector. The tumor was pedunculated and could easily be lifted out of the stomach. It was then resected with two fiings of a flexible endo-GIA™ 45-mm blue-cartridge linear stapler (Covidien, Mecheln, Belgium). The specimen was removed through the central opening of the Triport with careful protection of the wound edges by this device. Hemostasis was confirmed. The longitudinal gastrotomy was then closed in one layer with a Monocryl 2/0 running suture. The quality of the suture was tested with the instillation of methylene blue through the nasogastric tube. The hole in the fascia was closed with an interrupted Vicryl 1 suture and the skin with an intradermal Monocryl 2/0 suture.
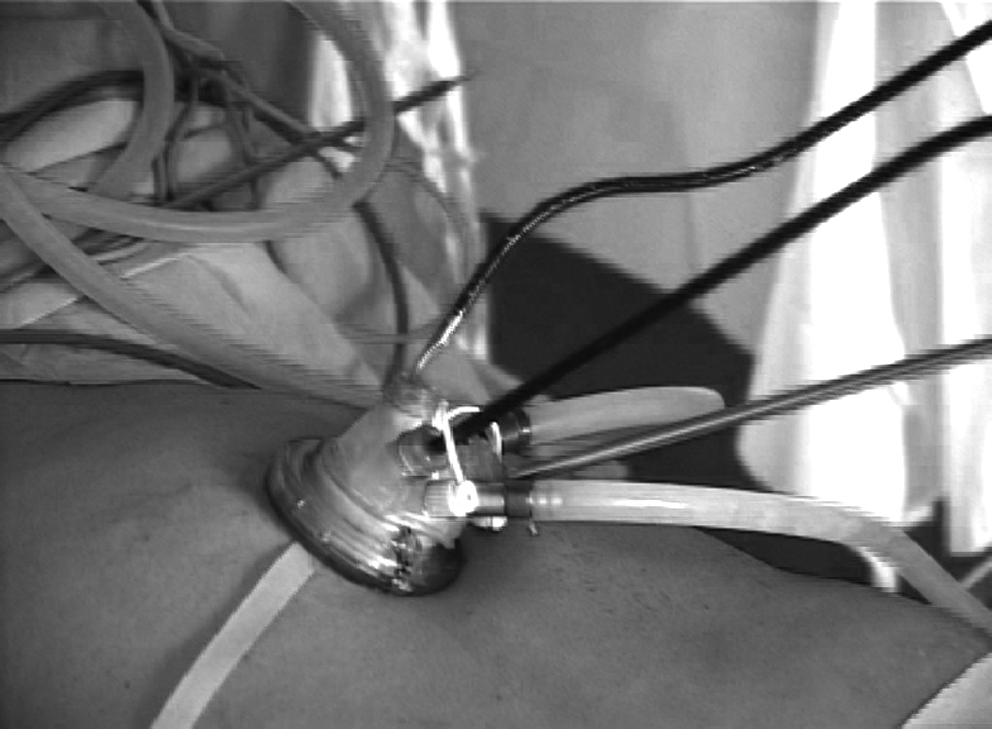
The Triport® (Olympus, Aartselaar, Belgium) inserted through a 3-cm periumbilical incision. The flexible ports make it possible to insert the double-bended instruments.

The specially designed “goose neck” 5-mm 30-degree videolaparoscope (Olympus, Hamburg, Germany), together with the exterior bend of the instruments, avoids instrument collision during surgery.
Results
Operation time from skin to skin was 140 minutes. There were no per- or postoperative complications. The patient started eating on the first postoperative day, but hospital stay lasted 4 days, mainly for social reasons. Pathology confirmed the histology of a gastrointestinal stromal tumor of 2 cm, with a mitotic activity less than 5 mitoses per high-power field and positivity for CD117. The resection margins were tumor free. Based on the pathology and size of the tumor, our patient was considered to be at low risk for recurrence, and no adjuvant therapy was planned. One month after surgery, the patient had healed completely with a minor periumbilical scar.
Discussion
Laparoscopic surgery has allowed for the performance of several major digestive operations through small incisions. The advantages of laparoscopically performed operations have led to an increasing interest in developing less-invasive procedures.1–12 Unlike natural orifice translumenal endoscopic surgery (NOTES), which faces obvious hurdles in safety and reproducibility, single-incision transumbilical laparoscopy is ready for widespread implementation. We have described a technique with specially designed instruments, which were kindly placed at our disposal by Olympus (Germany). These instruments have two permanent bends in their shafts, allowing relatively comfortable, intuitive manipulations. Even though the bends are rigid, the insertion through the flexible Triport poses no problem. A technical tip is to make a small incision in each gelport with a pointed blade to avoid tearing the gel. Also, the lubrification of the ports provides more easy manipulating. Each instrument is easily detachable from the handle and can, therefore, be used in a right- or left-handed way. The tip of the instruments can be rotated, which is of utmost importance in precise manipulations. On the outside, the extraperitoneal bend avoids contact between surgeons' hands. The specially designed “goose neck” camera makes it possible for the first assistant to have the camerahead and his or her hands out of the way of the handles of the instruments, thereby avoiding collision with each other. We have found it most easy to put the 12-mm port in the 2 O'clock position for the right-handed instruments and the endo-GIA stapler. One 5-mm gelport was put at the 6 O'clock position for the 5-mm videolaparoscope, and the other 5-mm port was positioned at the 10 O'clock level. The advantages of single-site surgery over conventional techniques are still to be proven. Our preliminary experience with LESS partial gastrectomy demonstrated at least the feasibility of the procedure. Larger or full-thickness tumors in close proximity to the pylorus or those tumors causing gastric outlet obstruction often require a more formal resection (i.e., antrectomy and gastrojejunostomy), due to the high probability that a wedge resection will result in narrowing of the distal stomach, causing iatrogenic gastric outlet obstruction. Masses in the proximity of the gastroesophageal junction can be managed similarly to tumors near the pylorus. The goals remain, if possible, to achieve an adequate surgical margin while maintaining the normal function of the lower esophageal sphincter mechanism. It needs to be said that the resection of a tumor at these anatomic sites would be more difficult by laparoscopic single-site surgery. At this time, we would consider a conventional laparoscopy or even open resection in these cases.
Conclusions
The idea of performing complex surgery through one single entry is fascinating and holds enormous potential. Further clinical investigation, in comparison to the established open and laparoscopic gastrectomy, should be conducted in order to evaluate the outcome of LESS partial gastrectomy.
Footnotes
Acknowledgments
Endogent, which is the cadaverlab of the Department of Anatomy of the University of Ghent and the Department of Surgery of the University Hospital of Ghent, receives logistic support from Olympus and financial support from Johnson & Johnson (New Brunswick, NJ).
Disclosure Statement
No competing financial interests exist.