
Abstract
Abstract
Background:
Laparoscopic distal pancreatectomy (LDP) has been shown to be an effective surgical option for benign lesions in the body and tail of the pancreas. However, its advantages and disadvantages have not been well characterized. In this study, we compared the outcomes of LDP and open pancreatectomy performed in our clinic.
Materials and Methods:
Peri- and postoperative outcomes were retrospectively compared between patients with benign pancreatic disorders who underwent open distal pancreatectomy (ODP) (n = 35) and those who underwent LDP (n = 40). The peri- and postoperative factors analyzed included operative time, blood loss, hospital stay, postoperative recovery, biochemical findings, and complications.
Results:
LDP was associated with significantly less operative blood loss (363 versus 606 mL; P = 0.001) and shorter hospital stay (22 versus 27 day; P = 0.009), but longer operative time (342 versus 250 min; P = 0.000), compared with ODP. There were no significant differences between the two groups in complication rates or postoperative recovery, except for the significantly shorter duration of postoperative pain-killer intake and earlier improvement of the biochemical analysis in LDP than in ODP.
Conclusions:
LDP appears to be a safe, desirable procedure for the management of benign pancreatic diseases, with outcomes similar to ODP.
Introduction
Materials and Methods
Patients and clinical variables
Between February 1998 and August 2009, a total of 156 patients with pancreatic lesions (including 76 malignant and 80 benign lesions) underwent distal pancreatectomy in the Department of Surgery 1 at Kyushu University Hospital (Fukuoka, Japan). One hundred and thirteen patients underwent open surgery (72%) and 43 (28%) underwent laparoscopic surgery. The open resections were performed earlier in our experience with pancreatic surgery, and the percentage of patients offered laparoscopic resection, rather than open resection, has increased over the time period of our study. Of the 76 patients with malignant pancreatic lesions, 73 were treated with ODP with lymph node dissection, and 3 were treated with LDP. To enable a comparison between the outcomes of ODP and LDP, only benign cases (80 cases) were selected for this study. We excluded 5 patients who had undergone major abdominal operations (i.e., gastrectomy, liver resection, and pancreaticojejunostomy), in addition to pancreatectomy, but included 5 patients who underwent additional cholecystectomy at the time of surgery. We, therefore, retrospectively compared 35 patients in the ODP group and 40 patients in the LDP group, with respect to the following clinical variables: operative time, operative blood loss, hospital stay, postoperative recovery, biochemical findings, and complications. Among the complications, pancreatic fistula was defined as any measurable volume of fluid on or after postoperative day 3 with an amylase level >3 times the serum amylase level, according to the definition of the International Study Group for Pancreatic Fistula (ISGPF). 6
Surgical procedures
ODP
ODP was performed via an upper midline incision or a left subcostal incision. The splenic artery was identified and ligated in advance of the transection of the pancreatic parenchyma to control intraoperative bleeding. The pancreatic parenchyma was transected sharply, using a scalpel, and the main pancreatic duct was ligated by using nonabsorbable sutures. The pancreatic stump was closed with fish-mouth sutures. A linear stapler (Echelon 60-4.5; Ethicon Endo-Surgery, Cincinnati, OH) was used to transect the pancreatic parenchyma in 8 patients (22%), and fibrin glue (Tisseal; Baxter Health Care, Deerfield, IL) was sprayed onto the pancreatic stump in an attempt to prevent pancreatic fistula formation.
LDP
LDP was performed, as described previously,7,8 with some minor modifications. Briefly, a subumbilical Hasson's trocar was inserted by the open technique, and four further trocars were then added (Fig. 1). Using ultrasonic coagulating shears (Harmonic scalpel; Ethicon Endo-Surgery) and/or a vessel-sealing system (LigaSure™, Tyco Healthcare Group, Boulder, CO), the greater omentum was divided between the stomach and transverse colon to reach the lesser sac. Intraoperative ultrasonography was used to localize the lesion (7.5 MHz, linear array probe; Aloka, Tokyo, Japan). The splenic artery was identified at the upper border of the pancreas and ligated at the proximal side of the resection line. The pancreatic parenchyma was transected proximal to the lesion, using a laparoscopic linear stapler (Echelon 60-4.5; Ethicon Endo-Surgery). In cases of splenic preservation, where it was difficult to preserve the splenic vessels, vessel ligation was performed, leaving the short gastric vessels to supply the spleen (i.e., the Warshaw technique). 9 The resected specimen was put into a surgical bag (Endo Catch™ II; US Surgical Corp, Norwalk, CT) and extracted after the widening of the left 10-mm port wound.
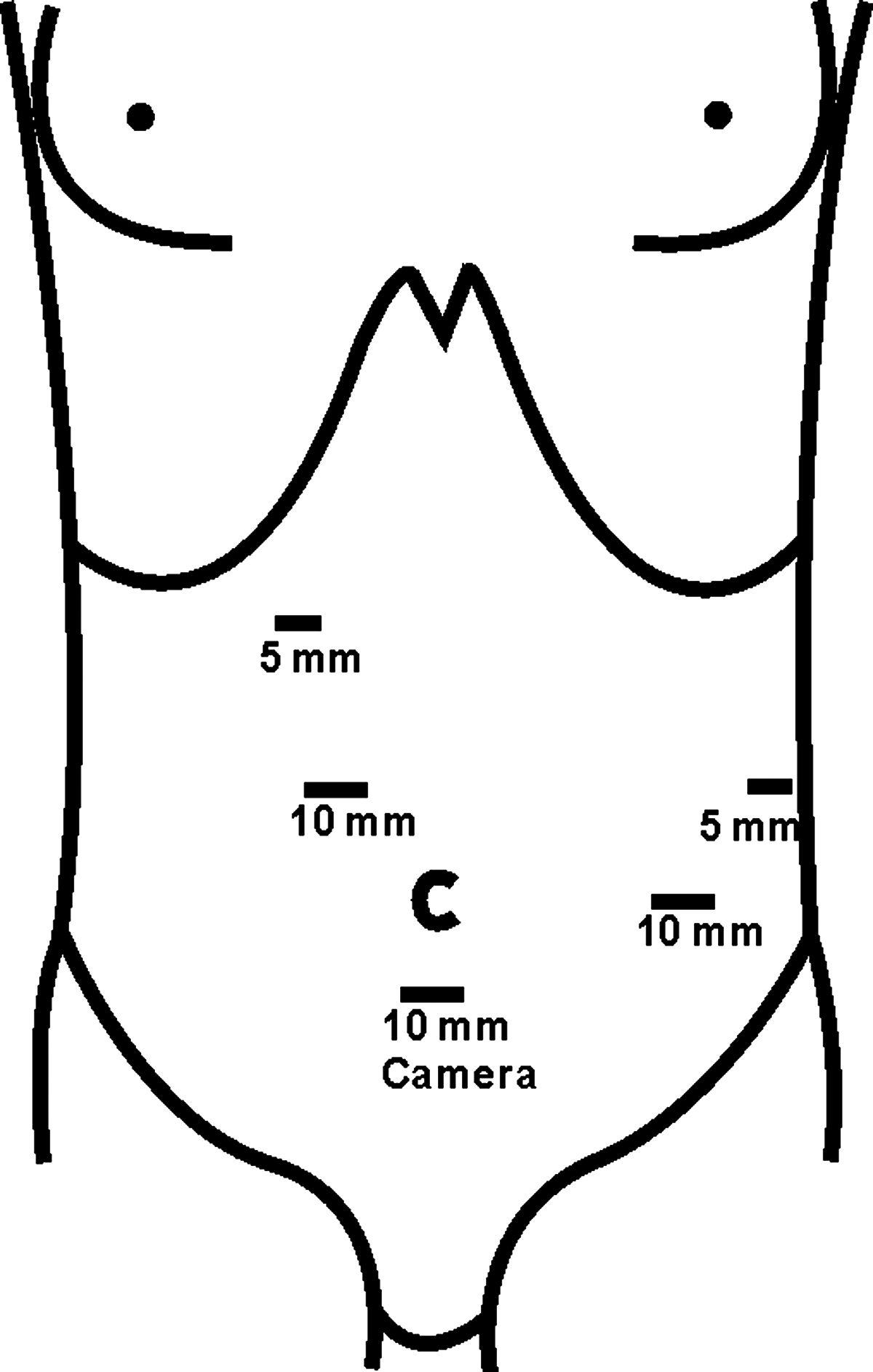
Placement of trocars for laparoscopic distal pancreatectomy. The 10-mm trocar below the umbilicus was for the camera. The two trocars on the right side were for the surgeon, and the two trocars on the left side were for the assistant.
Statistical analysis
Data are presented as the mean ± standard deviation. Statistical analysis was performed by using the Mann-Whitney U test for quantitative variables and chi-square test for qualitative variables, with statistical significance set at P < 0.05.
Results
Patient characteristics
Patient characteristics, including age, gender, BMI (basal metabolic index), size, location of the lesion, and pathologic diagnosis, are shown in Table 1. Ages, BMI, size, location of the lesion, and pathologic diagnosis were matched between the two groups, though the female-male ratio was significantly higher in the LDP group than in the ODP group.
LDP, laparoscopic distal pancreatectomy; ODP, open distal pancreatectomy; BMI, basal metabolic index.
Perioperative data
Perioperative outcomes are shown in Table 2. LDP was associated with significantly less intraoperative blood loss and shorter hospital stay, but longer operative time, than ODP. The operative time ranged from 160 to 753 and 124 to 699 minutes in LDP and ODP, respectively. The rates of spleen preservation and use of a stapling device were significantly higher in the LDP group than in the ODP group. Splenic vessels were more often preserved in the LDP group, but the difference was not significant. Four cases in the LDP group were converted to open surgery (uncontrollable bleeding in 3 and dense adhesions in 1). There were no significant differences between the two groups in postoperative recovery (in terms of day of first flatus, water intake, meal intake, and start of walking), but there was a significantly shorter duration of postoperative pain-killer intake in LDP than in ODP.
LDP, laparoscopic distal pancreatectomy; ODP, open distal pancreatectomy.
Postoperative biochemical findings
We compared postoperative biochemical findings between the two groups (Table 3). Serum levels of C-reactive protein (CRP) on postoperative day 1 (POD1), alanine aminotransferase (ALT) on POD3, and aspartate aminotransferase (AST) on the first and third PODs1 and 3 were significantly higher in the ODP group, compared with the LDP group.
LDP, laparoscopic distal pancreatectomy; ODP, open distal pancreatectomy; CRP, C-reactive protein; ALT, alanine aminotransferase; AST, aspartate aminotransferase; WBCs, white blood cells.
Complications
There was no significant difference in the rate of postoperative complications (including pancreatic fistula) between the two groups (Table 4).
Eight patients developed 9 complications.
Eleven patients developed 13 complications.
Grade B; grade A not included.
LDP, laparoscopic distal pancreatectomy; ODP, open distal pancreatectomy.
Multivariate analysis
Multiple logistic regression was done to determine how much the difference in perioperative outcomes was, indeed, due to the surgical approach. As illustrated in Table 5, operative time was significantly affected by the type of operation and blood loss and insignificantly affected by size of the lesion and patient gender. Table 6 shows that blood loss was significantly affected by the type of operation and operative time and insignificantly affected by size of the lesion and patient gender. Multivariate analysis of the hospital stay revealed that it was significantly affected by the rate of pancreatic fistula and insignificantly affected by other factors.
Discussion
There have been marked developments in laparoscopic surgery during the last two decades. Advanced laparoscopic surgery can be performed safely and effectively by experienced surgeons and in selected patients and can demonstrate several advantages over conventional open techniques. In the gastrectomy, laparoscopic surgery has shown comparable results to the open approach, in terms of decreased incidence of postoperative complications, decreased length of hospital stay, and decreased narcotic use. 2 In the colectomy, laparoscopic patients had lower median pain scores, earlier discharge, and faster resolution of ileus. 1 Laparoscopic splenectomy was associated with shorter hospital stay and fewer complications. 3
In the present study, we retrospectively compared the clinical and perioperative outcomes of LDP and ODP. LDP produced comparable results to ODP, in terms of complications and postoperative recovery, with less intraoperative blood loss, shorter hospital stay, and better cosmesis. These findings highlight the feasibility and safety of LDP and support its routine use in patients with benign distal pancreatic lesions. LDP was first reported by Gagner et al. in 1996, 10 and reports supporting its safety and feasibility have gradually increased in number since then. Velanovich 11 reported the first comparative study between LDP and ODP in 2006 and concluded that LDP produced surgical results equivalent to ODP, with shorter hospitalization time and faster return to normal activity. Several other studies comparing LDP and ODP have recently been published,11–19 and a review of these articles is presented in Table 7.
Significant difference.
L/O, laparoscopic/open; NA, not available.
The major operative differences noted in this series were a significantly longer operative time and reduced blood loss in the laparoscopic group. Other studies of LDP have reported operative times in the range of 154–308 minutes.4,17,20 The longer duration of surgery required for LDP can be partly attributed to the learning curve and decreases with increased experience. Even when the surgeon has adequate experience, operative time can be negatively affected by a change in surgical-room staffs and assistants. This effect can be minimized by adopting a team approach, allowing the consolidation of skills and expertise. Kim et al. 16 reported a median operative time of 195 minutes after performing 93 cases of LDP. They noted that operative time decreased as the experience of the operator increased (4.0 hours in the first quarter of the study, falling to 2.7 hours in the final quarter), thus emphasizing the demanding technical aspects of this procedure and the importance of the learning curve. In addition, our experience revealed that longer operative times were needed for pancreatic body lesions close to the superior mesenteric vein and in cases where splenic vessels were preserved.
Longer operative times did not translate into increased perioperative complications. We reported total complication rates of 20 and 31% in the LDP and ODP groups, respectively, which are comparable with those of previous studies (0–53 versus 0–57%).12,13,17,18,21 Pancreatic fistula is considered to be the most important complication following pancreatic surgery.7,22–24 The incidence of pancreatic fistula in our study was 12 and 17% in LDP and ODP, respectively (grade B; grade A not included). The reported incidences of pancreatic fistula in the literature show wide variability, ranging from 0 to 50%.7,12,14,17,19,21,25,26 This variation is mostly due to differences in the definition used for pancreatic fistula. All but one fistula in our study resolved after conservative management. One patient who underwent LDP also underwent percutaneous drainage of the intra-abdominal abscess, performed under radiologic guidance. An automatic stapling device was used in 95% of patients of LDP group in our study and in most other LDP studies previously reported.4,7,11,12,14–22,25,27–34 Automatic stapling and severance are simple, time-saving techniques and provide good results, but were used in only 22% of open cases in our series. Recognition of the superiority of these techniques is leading to increased use of the same techniques in ODP as well.
Regarding preservation of the spleen, we aimed to preserve the spleen as much as possible, unless the tumor was close to the splenic hilum or if ischemia was noticed after ligation of the splenic vessels, in cases of the Warshaw procedure. In the current study, splenic preservation was achieved more often in the LDP group (P = 0.01). Our results for spleen preservation in LDP (32%) were within the range reported in previously published articles (24–76%).8,13,19,21,27–30 Among the cases of splenic preservation in LDP (13 patients), we preserved the splenic vessels in 6 (46%), but used the Warshaw procedure in 7 (54%), 2 of whom developed postoperative splenic ischemia, which was responsive to conservative treatment. 8 Melotti et al., 21 however, reported a higher rate of splenic vessel preservation of up to 84%.
Postoperative recovery, represented by day of first flatus, day of first water intake, day of first meal intake, and day of start of walking, was similar in both groups in our study. This result is similar to that reported in some previous studies, 35 but different from others,12,14,16,17,36,37 and is strongly related to the personal preference of surgeons in charge in deciding the time to start of water and food intake. We detected a significantly shorter duration of postoperative pain-killer intake and earlier recovery of postoperative inflammatory response in the LDP group, indicated by serum levels of CRP, ALT, and AST, with no significant difference in white blood cell count. These parameters were not reported in some previous studies,11–13,15–19 while others reported no significant differences.14,38 Lee et al. 39 reported a significantly lower CRP on POD5 in patients undergoing laparoscopic distal gastrectomy, compared with those undergoing open gastrectomy. Like several previous studies,11,13,14–19 the results of the current study showed a significantly shorter hospital stay in the LDP than in the ODP patients (22 versus 27 days; P = 0.009). The longer hospital stay reported in LDP in our study (22 days) than that reported in Western studies is attributed to the health insurance system in Japan, which allows the patient to be hospitalized for a long time until the patient becomes pain free without a significant increase in cost.
Conclusions
In conclusion, the results of this retrospective study support the safety and usefulness of LDP for benign distal pancreatic lesions.
Footnotes
Disclosure Statement
No competing financial interests exist.