
Abstract
Abstract
Background:
We had developed an innovative method of minimally invasive surgery using gasless laparoscopy in resection of the small bowel lesion. This study aimed at evaluating the feasibility and efficacy of this procedure by comparison with traditional open small bowel surgery.
Methods:
A wedge or segmental resection of the small bowel for removal of the lesion was performed in 25 patients at National Taiwan University Hospital from September 2006 to January 2009. Thirteen patients underwent gasless laparoscopy-assisted surgery (GLAS), and 12 patients underwent open surgery. The perioperative characteristics and clinical results between the two groups were compared.
Results:
The demographics, clinical data, lesion size, and operative time were comparable between the GLAS and open surgery groups, but the wound length and blood loss were significantly less in the GLAS group (P < 0.001 and P = 0.021, respectively). The time to first postoperative flatus and first oral intake were significantly less in the GLAS group (P = 0.007 and 0.036, respectively). No major complication occurred in either group. No tumor recurrence was found after a median follow-up period of 14 months (range = 1−30) in the GLAS group.
Conclusions:
GLAS for resection of the small bowel may be a feasible and safe procedure for the small bowel lesions. It has the advantages of better cosmetic outcome, less blood loss, and earlier recovery of bowel movement.
Introduction
We had developed an innovative method of minimally invasive surgery using gasless laparoscopy in radical subtotal gastrectomy for early gastric cancer. 4 It combines the benefits of gas-filling laparoscopy and open surgery (OS) and can perform subtotal gastrectomy with completely intracorporeal reconstruction safely and effectively. 5 We had used it for other abdominal surgery such as gastrojejunostomy 6 and hepatectomy. 7 This method may be a very useful training for major laparoscopic procedures, and we applied it to the resection of the small bowel lesion. This study aimed at evaluating the feasibility and efficacy of this procedure in small bowel surgery by comparison with traditional open small bowel surgery.
Materials and Methods
Patients
We first searched the surgical database of National Taiwan University Hospital for cases coded as intestinal neoplasms preoperatively. There, only 25 patients underwent wedge or segmental resection of the small bowel for removal of the lesion from September 2006 to January 2009. The medical records of all the patients were retrospectively reviewed. Small bowel tumor was preoperatively diagnosed in all of the patients. No patient was excluded. The surgical indications were symptomatic lesion or suspecting malignancy. The choice of laparoscopic or OS was based on the surgeon's habit. Informed consent was obtained from every patient, and the possibility of open conversion was explained to the patients who underwent gasless laparoscopy-assisted surgery (GLAS).
Thirteen patients underwent GLAS by an experienced laparoscopic surgeon, and 12 patients underwent traditional open small bowel surgery by three experienced abdominal surgeons. The operative objective was complete resection of all grossly evident disease with negative margin. Patient variables including age, gender, and comorbidities were recorded. Disease and treatment variables including presentation, image study, operative method, wound length (incisions for trocar and drain were included), operative time, blood loss, lesion size, pathologic result, perioperative complication, time to first postoperative flatus, time to first oral intake, and days of hospital stay were recorded. The patients were regularly followed up at the outpatient clinic, and the follow-up information was obtained.
Operative method: gasless laparoscopy-assisted small bowel surgery
Under general endotracheal anesthesia, the patient was placed in the supine position. A 3–5-cm minilaparotomy was made in the upper or lower midline of the abdomen according to the size and location of the lesion shown on the preoperative images. A wound protector was used to cover the minilaparotomy wound to facilitate retraction and to avoid contamination or tumor cell implantation. The abdominal wall was lifted by our designed self-retaining retractors and wall-lifting system (Fig. 1).
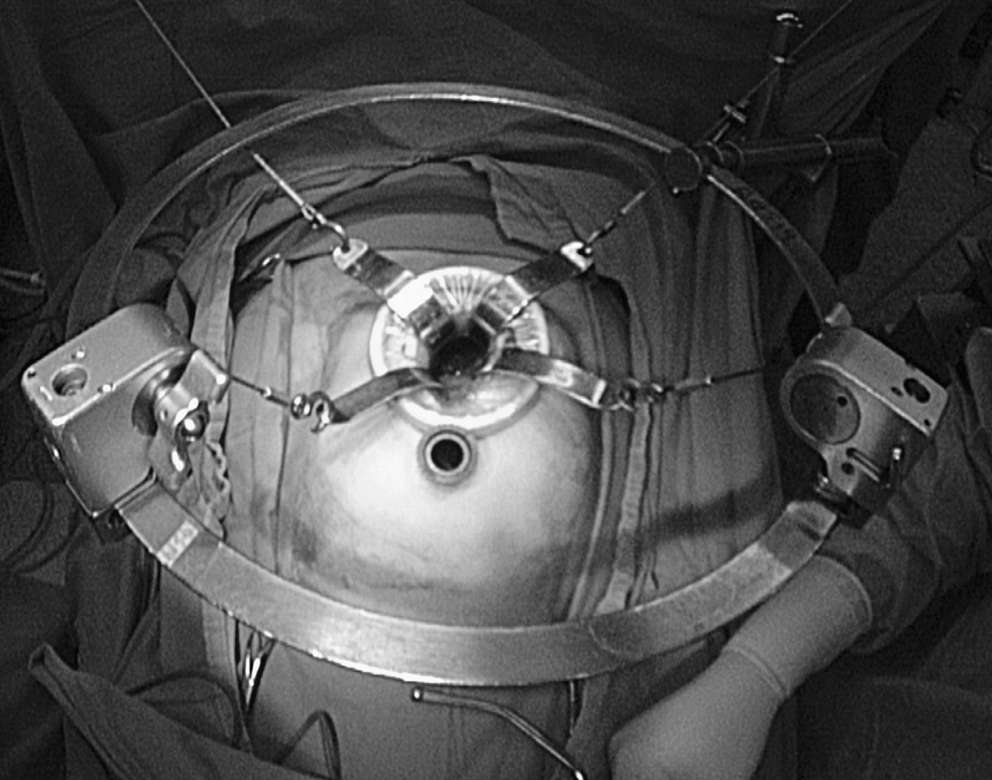
The abdominal wall was lifted by our designed self-retaining retractors and wall-lifting system.
A 10-mm, 30° telescope was inserted to inspect the peritoneal cavity and other abdominal organs. The small bowel bearing the lesion was exteriorized if the lesion was easily identified and the small bowel was fully mobile, then resection and anastomosis of the small bowel were performed on the body surface by linear staplers and handsewn closure. For duodenal or jejunoileal lesions that were not fully mobile or hard to be identified, two or three 10-mm trocars were inserted under laparoscopic vision in the bilateral abdominal and periumbilical areas, respectively. The laparoscope, traditional and laparoscopic instruments could be inserted through either the minilaparotomy wound or the trocar (Fig. 2). The lesion could be palpated by using one or two fingers through the minilaparotomy wound. Direct control of the bleeding was easily made by vigorous suction due to the gasless environment.
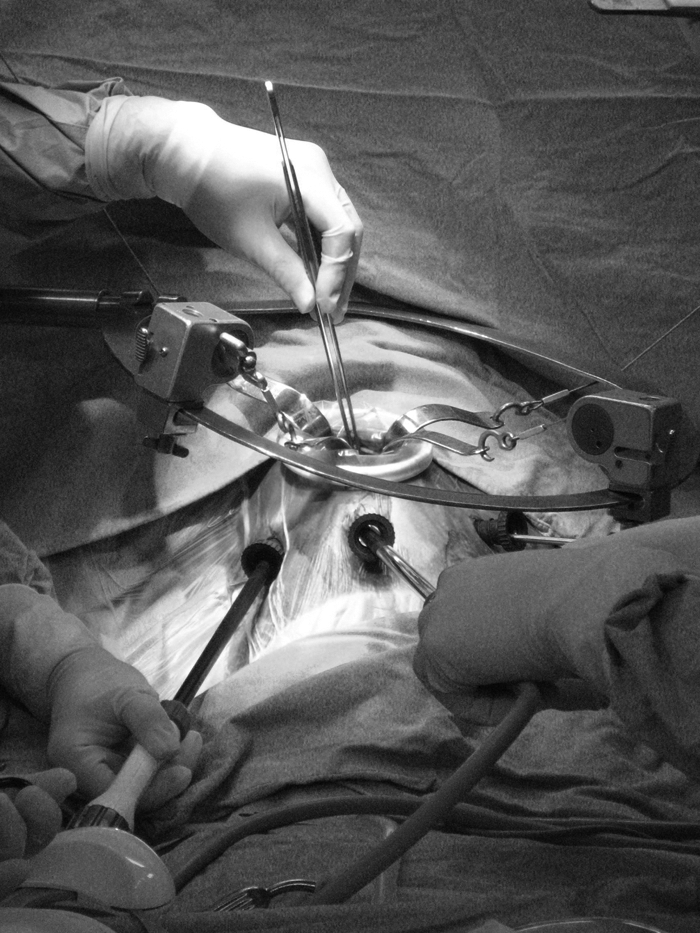
The laparoscope, traditional and laparoscopic instruments could be inserted through either the minilaparotomy wound or the trocars.
The Kocher maneuver was performed for the duodenal lesion, and the small bowel was sequentially examined from the ligament of Treitz to the ileocecal valve for the jejunoileal lesion. The lesion was identified by direct or laparoscopic vision and palpation. The decision about the resection procedure was based on the preoperative images and intraoperative findings. A wedge resection of the duodenum was made by an ultrasonically activated scalpel, and the intracorporeal repair was made by handsewn closure. A segmental resection of the small bowel was made by laparoscopic linear staplers, and the intracorporeal side-to-side anastomosis was made by a laparoscopic linear stapler and handsewn closure. The specimen was removed through the minilaparotomy wound. A drain was placed near the anastomosis site and taken out through the lateral trocar incision, and the wounds were closed. Postoperatively, the patient was started on a regular diet after flatus and discharged home after removal of the drain.
Statistical analysis
Depending on the type of data, descriptive statistics were calculated using frequencies, means, standard deviations, and medians. The two groups (GLAS versus OS) were compared with each other using independent Student's t-test or Mann-Whitney test for continuous variables and Likelihood Ratio χ2 test or Fisher's exact test for categorical variables. A value of P < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS for Windows v13.0 (SPSS, Inc., Chicago, IL).
Results
There were 7 male and 6 female patients with a mean age of 52 years (range = 16–81) in the GLAS group. There were 9 male and 3 female patients with a mean age of 59.2 years (range = 37–89) in the OS group. Half of the patients in the two groups presented with tarry-bloody stool. Most of the lesions were found using computed tomography scan or enteroscopy. The demographics and clinical data were given in Table 1, and there was no significant difference between the two groups.
GLAS, gasless laparoscopy-assisted surgery; OS, open surgery.
Among the 13 patients in the GLAS group, no patient was converted to OS, and 2 underwent resection of the small bowel on the body surface without other trocar insertions. The distribution of the lesion was similar in these two groups. There was no significant difference in the size of the lesions and in the operative time between the two groups, but the wound length and blood loss were significantly less in the GLAS group (P < 0.001 and P = 0.021, respectively) (Table 2). The pathologic results of the patients in the GLAS group were gastrointestinal stromal tumors (GISTs) in 5 patients, carcinoid tumor in 1 patient, diverticula in 3 patients, papillary adenoma in 1 patient, lipoma in 1 patient, cavernous hemangioma in 1 patient, and heterotopic gastric mucosa in 1 patient. The pathologic results of the patients in the OS group were GISTs in 7 patients, metastatic adenocarcinoma in 1 patient, metastatic pleomorphic carcinoma in 1 patient, lipoma in 1 patient, Brunner's gland adenoma in 1 patient, and tubular adenoma in 1 patient. The resection margin was free of tumor in all patients.
Statistically significant.
The time to first postoperative flatus and first oral intake were both significantly less in the GLAS group (P = 0.007 and 0.036, respectively). The hospital stay seemed to be less in the GLAS group but not significantly less (P = 0.132). Among the 13 patients in the GLAS group, 1 had glaucoma during hospitalization and underwent peripheral iridectomy, another one had reactivation tuberculosis after surgery. Among the 12 patients in the OS group, 1 had abdominal wound bleeding after surgery. No major complication occurred in either group. No tumor recurrence was noted after a median follow-up period of 14 months (range = 1–30) in the GLAS group. The patient with metastatic adenocarcinoma in the OS group had a recurrence 1 year after surgery. The patient with metastatic pleomorphic carcinoma in the OS group died of primary malignancy one and half months after surgery (Table 3).
Statistically significant.
Discussion
The small bowel tumors are relatively rare. GIST is the most common mesenchymal tumor of the small bowel. It usually grows out of the primary organ instead of diffusely infiltrating and rarely involves the lymph node, so it is appropriate for laparoscopic surgery in addition to benign tumors. In our study, half of the pathologic results were GISTs.
Laparoscopy had been used in small bowel resection for different tumors, including carcinoma,1,8 carcinoid tumor,2,9 leiomyoma,10,11 metastatic cancer,10,12 GIST,13–15 lipoma, 16 hemangioma, 17 and schwannoma. 18 Given the rare nature of these tumors, most published reports related to laparoscopic small bowel surgery are case-reports, and only two series exist at the time of writing this article.14,15 No comparative study was reported. Although different techniques were proposed, these laparoscopic methods initially used CO2 pneumoperitoneum.
In our GLAS, gas is not needed to inflate the peritoneum; and the contraindications or side effects related to pneumoperitoneum can be excluded. Vigorous suction can also be used for bleeding control without collapse of the space. 5 Our minilaparotomy wound was created first in the procedure to help get direct vision and dissect, in addition to helping exteriorize the small bowel or remove the specimen. This method provides a bridge for less-experienced surgeons from OS to advanced laparoscopic surgery, including totally laparoscopic approach for tumors in the duodenum, proximal jejunum, or terminal ileum.
In our GLAS group, the mean body mass index (BMI) was 23.1 kg/m2. The gasless technique may be much more difficult to use in obese patients with BMI over 30 kg/m2 and very difficult in patients with BMI over 50 kg/m2, because the operative field was limited due to thick abdominal wall and omentum. The maximum BMI in our GLAS group was 33.8 kg/m2, and it took longer time (205 minutes) to complete the wedge resection of the duodenal tumor in this patient.
The mean length of the wound was 6.5 cm in the GLAS group, which was significantly less than that in the OS group. It was similar to that of gas-filling laparoscopic surgery reported1,10,11 and had the same cosmetic effect. Moreover, with simultaneous use of traditional and laparoscopic instruments, the dissection, repair, and anastomosis could be easily performed and the learning curve could be speeded up. The tactile sensation could also be preserved by palpating the lesion using one or two fingers through the minilaparotomy wound. The median operative time in our GLAS group was 139.4 minutes (range = 35–295), which was similar to that in the OS group (143.8 minutes, range = 75–275) and that in previous reports of laparoscopic resection of small bowel tumors (9 patients, 129.7 minutes, range = 60–300).1,3,8,10,18
The intracorporeal bowel anastomosis could be easily made by a laparoscopic linear stapler in our GLAS, and the stapled entero-enterostomy did not increase the complication rate. 19 Intracorporeal repair or anastomosis for duodenum and segments of small bowel that could not be exteriorized, such as the jejunum near the ligament of Treitz and the ileum near the ileocecal valve, could avoid excessive dissection and manipulation of the small bowel and could decrease the inflammatory response. 20 Our study demonstrated that the patients who underwent GLAS had less blood loss, time to flatus, and oral intake than those in the OS group. The less blood loss may be related to less dissection, and the earlier return of bowel function may be related to less bowel manipulation. One patient with a jejunal GIST 8 cm in size who underwent open segmental resection of the proximal jejunum had a blood loss of 600 mL because of injury to mesenteric artery during manipulation, and the difference of blood loss was still statistically significant after excluding this patient (11.54 versus 116.36 mL, P = 0.048). The hospital stay was less in the GLAS group than that in the OS group, but the difference was not statistically significant (7.4 versus 8.3 days, P = 0.132). It might be related to the sample size of our study or the timing of removing the drain tube. All the patients were discharged home after removal of the drain.
We placed drains after small bowel surgery, because we think that placement of drains after small bowel anastomosis can detect anastomotic leak and bleeding earlier. However, neither anastomotic leakage nor postoperative internal bleeding occurred in both groups. Not to drain may be considered to let patients get discharged earlier.
In previous reports,1–3,8–18 no major complication occurred after laparoscopic resection of the small bowel except 1 with anastomotic bleeding in the jejunum. 14 In our study, no technique-related complication occurred in both groups. According to our previous study focusing on the small-intestine GISTs, recurrence was noted within a median time of 12 months after surgery. 21 However, no recurrence was noted after a median follow-up period of 14 months (range = 1–30) in the 5 patients with GIST in the GLAS group. There was also no recurrence in the patient with carcinoid tumor in the GLAS group.
At the time of writing this article, our study is the first series to compare gasless laparoscopy-assisted small bowel surgery as a minimally invasive surgery with the traditional open small bowel surgery. It has proved that the GLAS has better cosmetic outcome, less blood loss, and earlier recovery of bowel movement. It also proves the feasibility and safety of this technique due to the similar operative time and no tumor recurrence. However, the sample size is not large due to the rare nature of the small bowel tumors. The long-term oncologic outcome is also unknown. Application to more patients and longer follow-up period are needed to evaluate the recurrence rate and long-term survival.
To sum up, we developed an innovative method of minimally invasive surgery using gasless laparoscopy in resection of the small bowel lesion. We collected the data of 25 patients with the small bowel lesions undergoing the gasless laparoscopy-assisted resection or the open resection of the small bowel, and we compared the perioperative characteristics and clinical results between the two groups. The gasless laparoscopy-assisted resection of the small bowel may be a feasible and safe procedure for small bowel lesions. It has the advantages of better cosmetic outcome, less blood loss, and earlier recovery of bowel movement. This innovative procedure is a very useful training for major laparoscopic procedures and may be suggested.
Footnotes
Disclosure Statement
No competing financial interests exist.