
Abstract
Abstract
The current report is a multicenter study of a series of infants who developed colonic strictures (CS) as a sequelae of necrotizing enterocolitis (NEC) and who were treated successfully with laparoscopic intestinal resection and primary anastomosis. During 2005–2008, 11 neonates (gestational ages, 32–38 weeks), with a mean birth weight of 1.7 kg (range, 0.96–2.2) and a mean weight at operation of 3.04 kg (range, 1.6–4.4 were approached laparoscopically, following the diagnosis of a post-NEC-CS. The two surgical techniques were: 1) laparoscopic mobilization with extracorporeal resection and anastomosis (LERA) in 4 (36%) and 2) laparoscopic mobilization with intracorporeal resection and anastomosis (LIRA) in 7 (64%) patients. Laparoscopy was effectively performed in all cases without conversion to open surgery. The median operative time was 93 minutes (range, 80–121). The anastomosis was colocolic in all patients, except in 1 case, in which it was colorectal. There were no operative complications. All babies recovered uneventfully and started oral feeding at a median time of 3.5 days (range, 1–11) postoperatively. Hospital discharge was at a median time of 9 days (range, 2–29) following operation. No recurrent strictures have developed.
Introduction
(
Materials and Methods
During 2005–2008, a retrospective review was performed to identify infants who developed an intestinal stricture following an episode of NEC that was managed medically at three participating hospitals. The following variables were recorded and analyzed by descriptive statistics: result of the contrast enema study; site of obstruction; type of CS; operative time; anastomotic technique; site of exteriorization of the resected bowel; complications; histologic findings; initiation of oral feeding; length of hospitalization; and length of follow-up.
Operative approach
The infants were placed in a dorsal decubitus position for laparoscopy. Three ports or stab incisions were used in all patients. A 3.5-mm angled (30- or 45-degree) telescope was introduced through the (4- or 5-mm) umbilical port. The other two working sites (3–5-mm cannulas or 2-mm stab incisions), used for introducing the instruments, were positioned, depending on the site of the CS. A 6–10 mm Hg carbon-dioxide (CO2) pneumoperitoneum was employed. Two surgical techniques were utilized, according to surgeon preference. These two approaches were: 1) laparoscopic mobilization with extracorporeal resection and anastomosis (LERA) (Fig. 2), in 36% of the patients, and 2) laparoscopic mobilization with intracorporeal resection and anastomosis (LIRA) (Fig. 3) in 64% of the patients. The anastomosis was hand-sewn in all cases. In 2 babies, an inner layer running 5-0 polyglyconate and an outer layer interrupted 4-0 silk were used. In 9 patients, interrupted 5-0 and 4-0 polyglactin stitches were utilized.

LERA. (

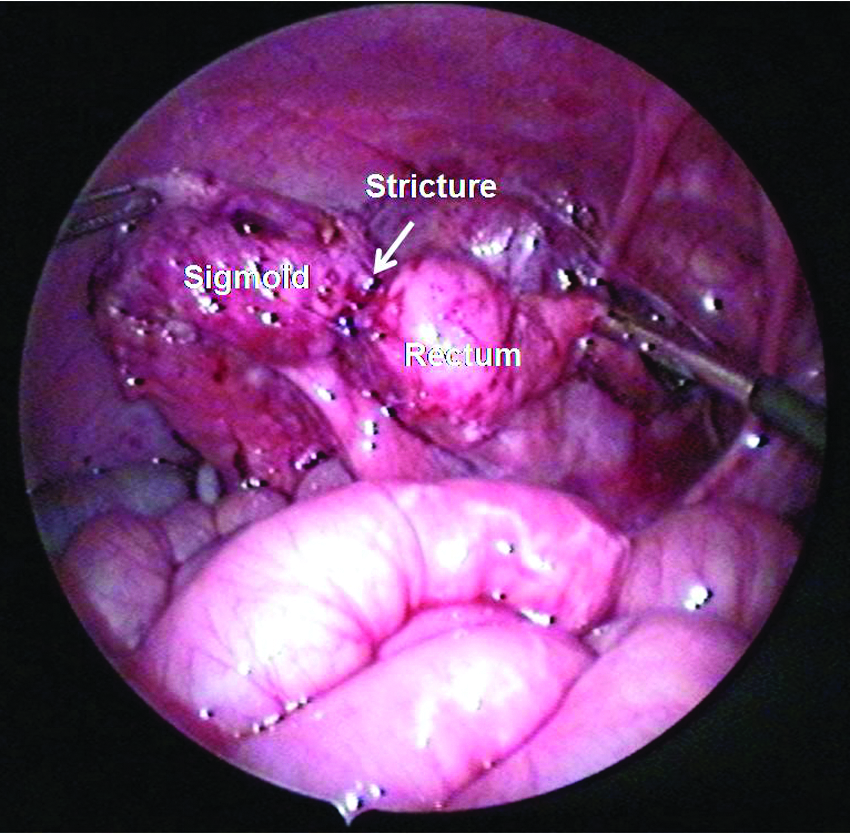
LIRA. Colorectal intracorporeal anastomosis (arrow). Same patient as in Figure 1. Note the interrupted 5-0 absorbable stitches. In this patient, the stenotic segment was retrieved through the anus.
Results
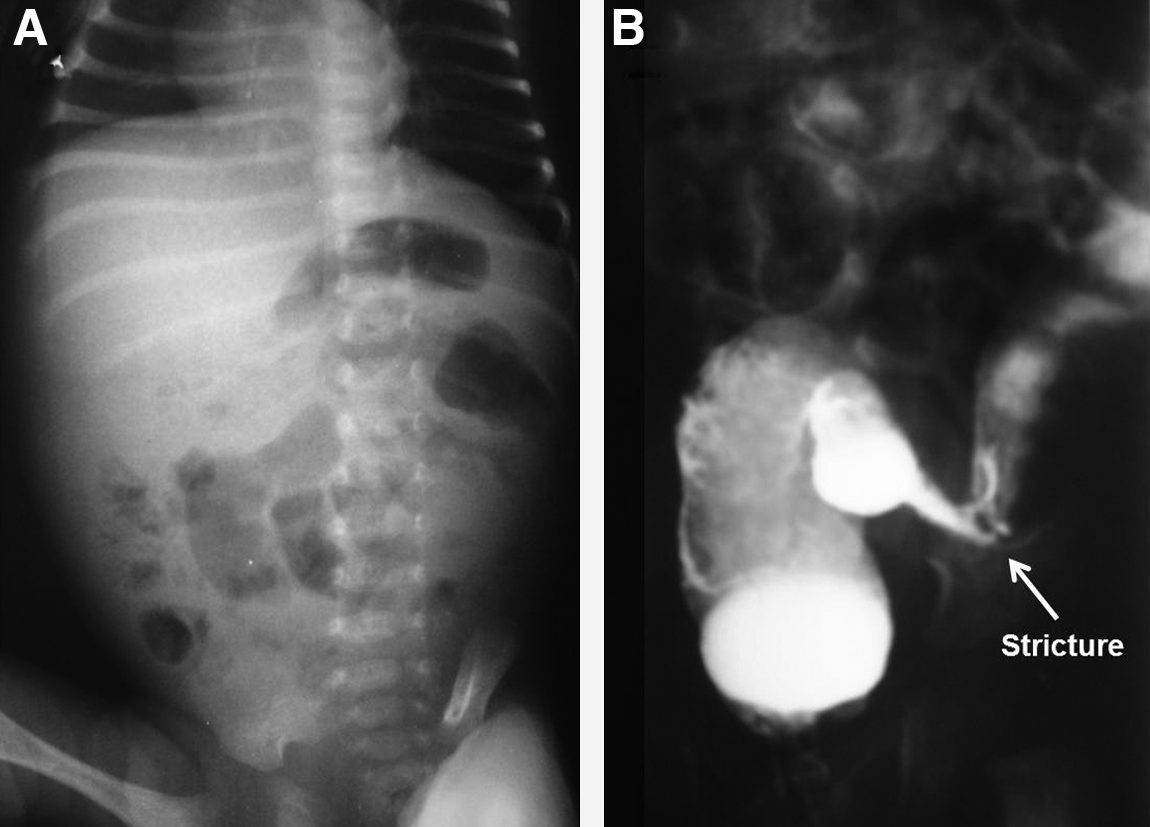
Eleven neonates (gestational age, 32–38 weeks), with a mean birth weight of 1.7 kg (range, 0.96–2.2) and a mean weight at operation of 3.04 kg (range, 1.6–4.4), were found to have a post-NEC-CS. There were no small-bowel strictures identified (Table 1). The NEC episode had been managed medically with parenteral nutrition, nasogastric suction for gastrointestinal decompression, and broad-spectrum intravenous antibiotics in all patients. The mean time between the identification of the CS and NEC was 7 weeks (range, 3–21). Most babies developed at least 2 of the following symptoms: abdominal distention, bilious vomiting, diarrhea, and low grade fever. Gastrointestinal bleeding was found in only 1 patient. The mean age at operation was 9 weeks (range, 4–21). A contrast enema study was employed to confirm the diagnosis of a CS in all cases. The sites of obstruction were ascending colon (1), hepatic flexure (1), transverse colon (1), splenic flexure (5), left colon (2), sigmoid colon (2), and rectum (1). One baby (case 8) had two areas of stenosis (Figs. 4 and 5).
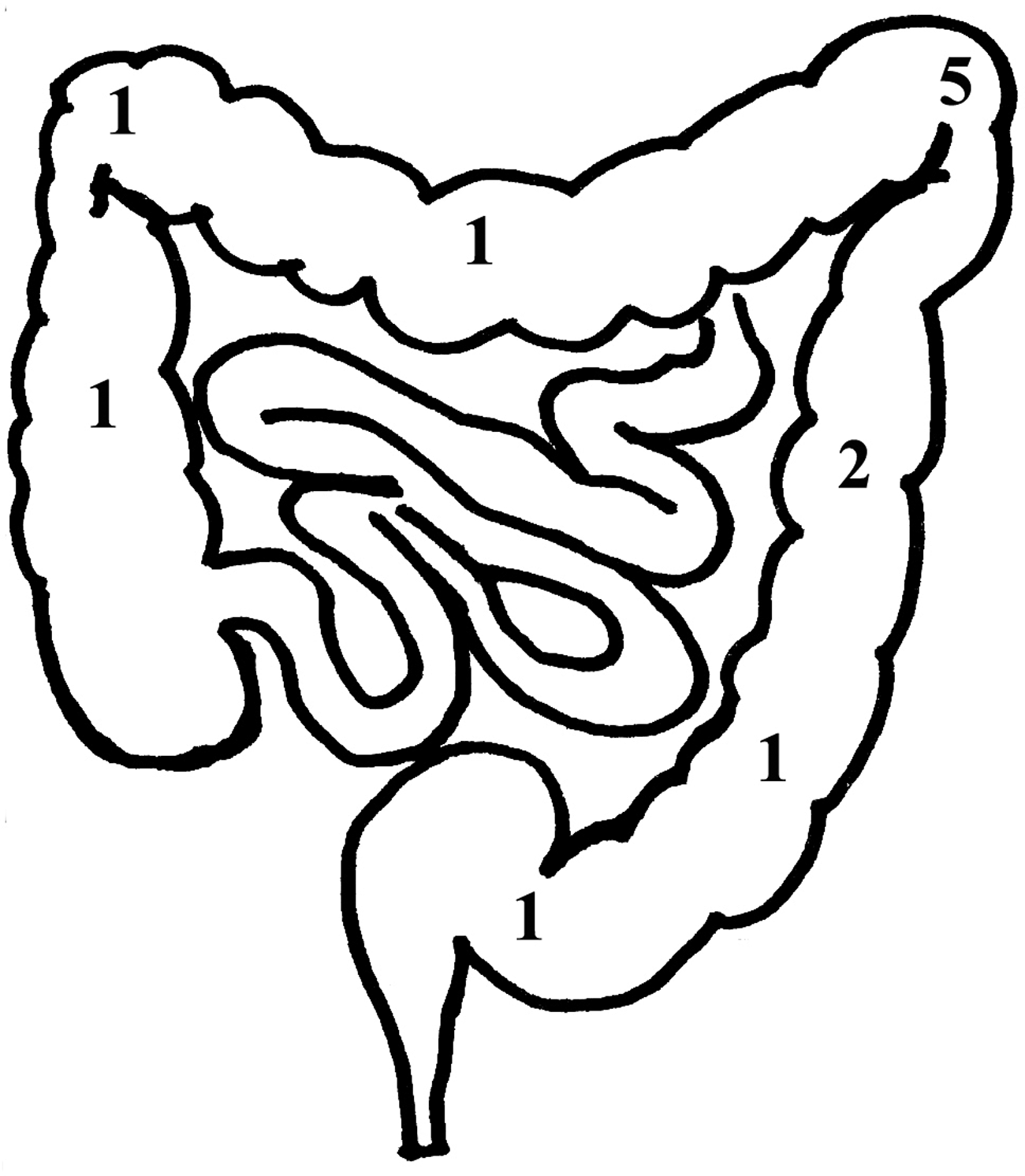
Graphic depicting the sites of colonic obstruction in these 11 patients.
Same patient (case 11) as in Figure 1. Note the severe rectosigmoid stricture (arrow) before laparoscopic intracorporeal resection and anastomosis.
LERA, laparoscopic extracorporeal resection and anastomosis; LIRA, laparoscopic intracorporeal resection and anastomosis.
Laparoscopy was effectively performed in all cases without the need of conversion to an open procedure. Median operative time was 93 minutes (range, 80–121). The anastomosis was colocolic in all patients, except for 1 baby, in which it was colorectal. The stenotic intestinal segments were exteriorized through the umbilical incision in all patients, except for one. In this infant, the diseased bowel was removed through the rectum. There were no operative complications. Postoperatively, 1 patient developed a small umbilical hernia, which was recognized at 3 weeks after operation and resolved over the next 1.5 years. Histologically, acute and chronic inflammation, ulcerations, and/or fibrosis were seen in all specimens.
All infants recovered uneventfully (Fig. 6). Oral feeding was initiated at a median time of 3.5 days following operation (range, 1–11). Hospital discharge occurred at a median time of 9 days (range, 2–29) following the laparoscopic resection. In 2 patients, a long postoperative hospitalization was due to staphylococcal sepsis for reasons unrelated to the operation (i.e., intrahospital infection). A summary of the results is detailed in Table 1. No new intestinal strictures have developed during the postoperative follow-up.
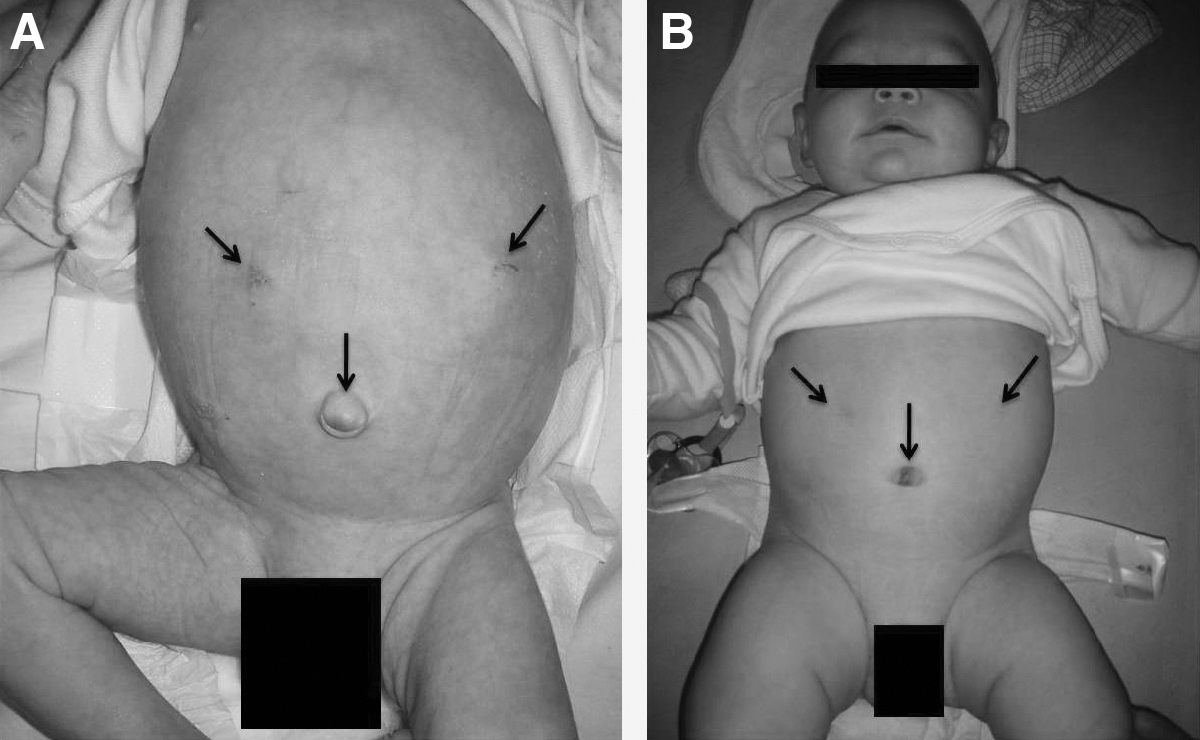
Postoperative cosmetic results at 15 days (
Discussion
NEC is the most common gastrointestinal emergency condition in the newborn, often affecting premature infants during the first 2 weeks of life. 9 Medical management includes bowel rest, gastric decompression, systemic antibiotics, and parenteral nutrition. 10 An intestinal stricture (with the colon being the most common site) can develop within 3 weeks to 3 months after both medical and surgical treatment for NEC and in both the functional and defunctionalized bowel. 11 In this study, a CS developed at a mean time of 21.8 days (range, 3–33) after medical NEC treatment. These neonates may not initially have had symptoms, hence pointing out the need for close clinical follow-up of such infants.
Symptomatic intestinal strictures usually require an operation, which, traditionally, has been via a laparotomy. 12 One of the coauthors (SSR) previously reported that an NEC CS could be successfully approached laparoscopically. 8 In our series, the two different approaches (LERA and LIRA) were feasible and well tolerated in these premature newborns. In addition, similar benefits found in other laparoscopic procedures were seen as well, including early initiation of oral feeding, reduced postoperative hospitalization, and better cosmetic result.
Conclusions
This series was an early attempt to evaluate the role of laparoscopy for the operative management for colonic strictures. All 11 patients in this series recovered well from the laparoscopic approach with either an intra- or extracorporeal resection and anastomosis.
Footnotes
Disclosure Statement
No competing financial interests exist.
This article was presented at the 19th Annual Congress for Endosurgery in Children in Waikoloa, Hawaii, June 8–12, 2010.