
Abstract
Abstract
Introduction:
Increasing literature has been published lately addressing the safety and efficacy of en bloc stapling of the renal hilum during laparoscopic nephrectomy and nephroureterectomy. The aim of this review was to analyze the available literature on en bloc stapling of the renal hilum and to complement it with technical issues that are required, according to our vast experience in en bloc and separate stapling, to safely control the hilum with this technique.
Materials and Methods:
A PubMed search using the terms “en bloc,” “nephrectomy,” and “laparoscopy” was conducted. We identified seven publications that have looked into hilar stapling technique.
Results:
Seven publications were found, which included a total of 434 patients who underwent en bloc stapling of the renal hilum. No complications specifically ascribable to this type of hilar control were encountered. No cases of postoperative arteriovenous fistula have been reported.
Conclusions:
En bloc stapling has become an established method to secure the renal hilum during laparoscopic nephrectomy and laparoscopic nephroureterectomy. Although no cases of postoperative arteriovenous fistula formation have been reported with the use of modern titanium staplers, longer follow-up is necessary to ascertain that it does not occur in the late postoperative period. We believe that well-trained laparoscopic surgeons should master this technique in both emergency and elective situations.
Introduction
The aim of this review was to analyze the current literature on en bloc stapling of the renal hilum and to complement it with technical issues that are required, according to our vast experience in en bloc and separate stapling, to safely control the hilum with this technique.
Materials and Methods
A PubMed search using the terms “en bloc,” “nephrectomy,” and “laparoscopy” was conducted. We identified seven publications that reported on en bloc stapling of the renal hilum during LN or laparoscopic nephroureterectomy (LNU) (Table 1).
AVF, arteriovenous fistula.
Results
The first report regarding en bloc hilar stapling was published by Rapp et al. 2 in 2004 and it included 433 LN and LNU. They performed emergency en bloc stapling in 26 patients with difficult hilar dissection or unexpected bleeding, in an attempt to maintain the laparoscopic approach and avoid conversion, thus realizing the feasibility of this approach. No perioperative complications were encountered and no cases of AVF were identified after a mean follow-up of 26 months. Despite these favorable results, they advocated that individual control should be the standard, with mass control used as a measure to prevent conversion to open surgery.
Kouba et al. 3 reported on 161 consecutive patients undergoing LN or LNU for tumoral conditions and nonfunctioning kidneys with at least 12 months of follow-up, comparing 90 patients with en bloc to 71 with individual stapling. The study included patients with pure laparoscopic and hand-assisted approaches, although their distribution was not detailed. Patients in the en bloc group had less intraoperative blood loss, although the difference did not reach statistical significance (173 versus 296 mL; P = 0.068). This trend was maintained when analyzing a subgroup with T2 tumors (225 versus 535 mL; P = 0.15). No cases of AVF were encountered after a mean follow-up of 34 months.
Buse et al. 4 prospectively enrolled 57 patients to assess the safety and feasibility of planned en bloc stapling during LN and LNU. Median blood loss and operative time were 100 mL and 145 minutes, respectively. Stapler malfunction was detected in 1 case (1.8%) (failure to open the stapler after firing) and resulted in conversion to open surgery. Three patients (5.2%) underwent open reoperation and the cause was found to be unrelated to the method of hilar control. After a mean follow-up of 12 months, no specific complications regarding en bloc stapling, including AVF, were found.
White et al. 5 specifically searched for AVF in 94 patients who underwent en bloc stapling during open (n = 43) and hand-assisted LN (n = 51). The patients were followed for a mean of 35.2 months with complete physical examination and CT imaging. No evidence of AVF formation was found. Stapling malfunction occurred in 2% of the cases, with no need for conversion. Estimated blood loss was 150 mL for open and 75 mL for hand-assisted laparoscopic surgery.
Ou et al. 6 reported on 23 patients with transitional cell carcinoma (TCC) who underwent retroperitoneal hand-assisted LNU with en bloc stapling of the renal hilum and found no cases of AVF after 24.5 months of follow-up.
Schatloff et al. 7 compared 65 patients who underwent en bloc stapling with 60 patients with individual vessel stapling during LN and LNU in the same time period for tumoral, inflammatory, and infectious conditions and did not find differences in operative outcomes or complications, with no cases of AVF encountered after a median follow-up of 25 months. Mean blood loss was 100 mL for en bloc versus 135 mL for separate stapling (P = 0.3). Stapler malfunction occurred in 1 patient during individual stapling of the renal vein.
Conradie et al. 8 reported on 90 patients who underwent en bloc stapling, including cases of inflammatory and tumoral conditions. Mean operative blood loss and operative time were 32 mL (range, 0–200) and 56 minutes (range, 22–130), respectively, and no cases of AVF were encountered after a mean follow-up of 28 months. No stapler failures were reported.
Discussion
A summary of the published studies on en bloc stapling of the renal hilum is detailed in Table 1. Initially described as a salvage maneuver to prevent open conversion, en bloc stapling has become the preferred method of hilar control in many centers. Although no randomized trials have yet been reported, it seems that en bloc stapling might shorten operative time, decrease blood loss, and reduce the rate of open conversion. With data of 434 patients being published up to now, including cases of inflammatory and infectious conditions, no cases of AVF have been encountered.
En bloc stapling of the hilum requires much less hilar dissection than separate hilar control. Our technique to prepare the hilum for en bloc stapling consists in dissecting from the lower pole upward along the psoas sheath. All fatty and flimsy tissue located posterior to the hilum is bluntly dissected. Pulsations of the renal artery are detected but no effort is made to dissect it or clearly identify it. No dissection is performed inside the hilum itself. After this, a path is created at the cranial border of the renal vein using the suction probe. The tip of the suction probe should be directed caudally and it is usually observed coming out posterior to the hilum (Fig. 1). So, we basically surround the hilum without getting into it. On the basis of our experience, we have found that almost any hilar configuration is amenable to be en bloc stapled with this technique, including wide or fibrotic hilums and those with early vascular divisions. A condition that would not allow for a single en bloc stapling would be an extrahilar artery coming out directly from the aorta. In these situations, this polar artery is first stapled individually and a second load is used for the hilum itself.

The hilum is isolated during a right nephrectomy. A thin path is created with the suction probe at the cranial border or the renal vein to allow subsequent placement of one of the stapler jaws.
Stapling is one of the safest forms of vascular control. Device malfunctioning occurs in ∼1%–2% of cases, being mostly ascribed to preventable reasons. When improper stapling technique was excluded from the analysis, failures were <0.5%. 9 There is no demonstrated association between en bloc stapling and increased risk for stapler failure. Indeed, the majority of cases of stapler failure have occurred during isolated stapling of the vein and not during en bloc stapling.
A proper stapling technique should include the following technical considerations. Before firing the device, the surgeon must verify that both jaws are aligned and touching one another. Bulky tissue or solid structures (e.g., clips) between the jaws should be removed or dissected, as they will make the cutting to proceed over noncorrectly aligned stapled borders. As a measure of safety, the stapler jaws should be observed and checked along their entire length before proceeding to fire (Fig. 2). Provided no blind stapling is performed, en bloc stapling is an excellent technical resource to prevent conversion to open surgery should unexpected bleeding or difficult hilar dissection be encountered. After identifying the surrounding anatomical landmarks (e.g., vena cava, aorta, psoas muscle), bleeding is controlled by lifting the kidney and stapling the hilum.
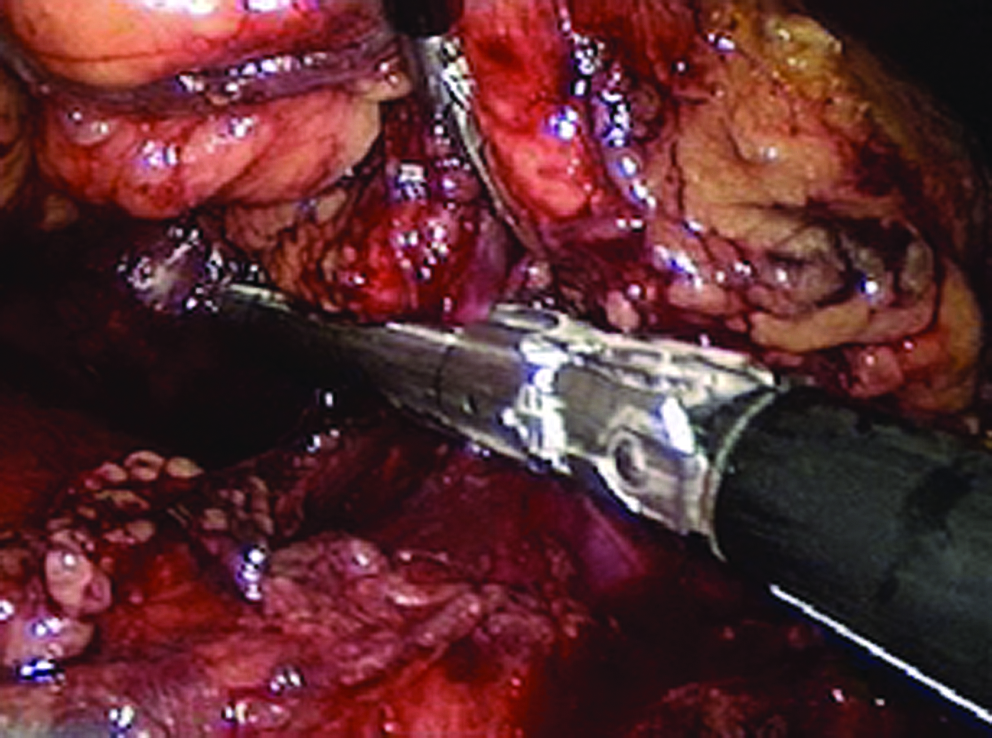
Correct stapling technique. The case is the same as that shown in Figure 1. Notice that the stapler jaws are perfectly aligned and visible through all their length.
One of the greatest fears during the stapling process is the risk of device failure and acute bleeding. We regularly use the EndoGia Universal (Autosuture) with 2.5-mm clips and have not had any inconvenience. However, it is worth to comment that sometime ago we tried with a stapler from a different company and happened in two cases that the stapler got locked during the firing process, meaning that only a part of the target was stapled and cut. In this condition, opening the stapler jaws would lead to uncontrolled bleeding. As a general safety issue, we recommend to close over the distal half of the hilum, meaning closer to the kidney. This safety maneuver allowed us in these specific cases to obtain proximal hilar control by placing a second stapler underneath. Other possible ways to deal with a trapped stapler include proximal placement of separate clips in the artery and vein and laparoscopic intracorporeal freehand knot tying. However, if there is not enough renal vein length, the artery can be clipped proximal to the stapler and the inferior vena cava temporally closed with a laparoscopic Satinsky or bulldog clamps. The hilum is cut and the inferior vena cava (IVC) can be repaired laparoscopically if necessary. If none of this is possible, the procedure should be converted to open surgery.
Conclusions
En bloc stapling has become an established method to secure the renal hilum during LN and LNU. Although no cases of postoperative AVF formation have been reported with the use of modern titanium staplers, longer follow-up is necessary to ascertain that it does not occur in the late postoperative period. We believe that well-trained laparoscopic surgeons should master this technique in both emergency and elective situations.
Footnotes
Disclosure Statement
No competing financial interests exist.