
Abstract
Abstract
A persistent gastrocutaneous fistula (pGCF) is an all-too-common complication following removal of a gastrostomy tube (GT) in a child and is associated with significant morbidity. The most common initial methods to manage pGCF include local would care and occlusion techniques. Failure of this approach is followed by surgical excision of the fistula tract and closure of the gastrostomy under general anesthesia. We report the first use of a tissue adhesive, 2-octylcyanoacrylate (2OC) (Dermabond; Ethicon, Sommerville, NJ) as a non-surgical method to close pGCF in children.
Methods:
The families of children presenting to the pediatric surgical division for management of a pGCF were offered the option of 2OC closure. Children not receiving or who failed to achieve closure with 2OC therapy underwent surgery for excision of the pGCF with primary closure of the stomach and soft tissues.
Results:
Seven children underwent 2OC therapy. 57% (4 of 7) of the children had complete closure of the pGCF with 2OC therapy. Three children underwent operative closure without complication.
Conclusions:
The tissue adhesive 2OC can successfully close a pGCF in children after GT removal. This therapy is cost-effective, non-invasive, does not require general anesthesia, and can be performed in an outpatient setting.
Introduction
In this article, we report a novel use of a tissue adhesive, 2-octylcyanoacrylate (2OC) (Dermabond; Ethicon, Sommerville, NJ), to achieve the closure of pGCF in children. Multiple studies have demonstrated that wound closure with 2OC is comparable with other standard wound-closure techniques. 2OC has also been used for rapid nail fixation after nail-bed repair, skin-graft fixation, temporary otoplasty, as a wound sealant, for treating oral aphthous ulcers, and in the treatment of corneal perforations.3–7 The use of 2OC is well-tolerated and associated with few complications.8–12
Materials and Methods
Following approval by the Institutional Review Board, the families of children presenting to the pediatric surgery division for the management of a pGCF were offered closure with the tissue adhesive, 2OC. Seven children underwent 2OC therapy, and the following data were retrospectively reviewed: 1) diagnostic indication for gastrostomy-tube placement, 2) age of child at time of 2OC therapy, 3) technique used to place the gastrostomy tube, 4) size of gastrostomy tube, 5) time of indwelling gastrostomy tube prior to removal, 6) success of 2OC therapy, and 7) length of follow-up after 2OC therapy.
Technique
Informed consent was obtained after a discussion with the families, which included the nature of tissue adhesive and the risks and benefits of 2OC therapy. The pGCF site was prepared with alcohol and adhesive remover to ensure that the orifice was clean, dry, and free of any foreign body. Any visible granulation tissue was completely cauterized with silver nitrate prior to the application of 2OC. The pGCF site borders were manually opposed with gentle traction, by hand, on the abdominal skin to avoid any 2OC extending between the wound edges, since this would impede healing. The 2OC was applied in three layers, as reported in the package description and previous reports.3,4 The area was allowed to dry and was then covered with a small dressing. The patients returned for follow-up weekly, and, if the 2OC therapy failed, the parents were given the option of repeat 2OC therapy or operative closure of the pGCF. If the pGCF did not respond to 3 applications of 2OC, it was considered a failure, and the child underwent operative closure.
Results
All 7 children who presented to the pediatric surgery clinic following removal of their GT had a pGCF of greater than 1 month in duration. Each of the 7 children underwent 2OC application in the clinic. The range of presentation with a pGCF was 4–7 weeks following appliance removal. The 2OC therapy was well tolerated, without complication, in all the cases (Fig. 1). Four children (57%) had complete 2OC closure, and 3 eventually required operative repair of the pGCF. Of the 4 children in whom the 2OC was successful, the indwelling GT had been in situ for an average of 17.3 versus 28.7 months in those children who failed therapy. The GT size was 12–14 Fr in those children who were successfully closed versus 2 of 3 children who failed closure had a GT size of 16 Fr. The diagnostic indication for GT placement, age of the child at the time of 2OC therapy, and GT placement technique did not appear to influence the effectiveness of 2OC therapy. The mean length of follow-up after 2OC was 16 months (Table 1).
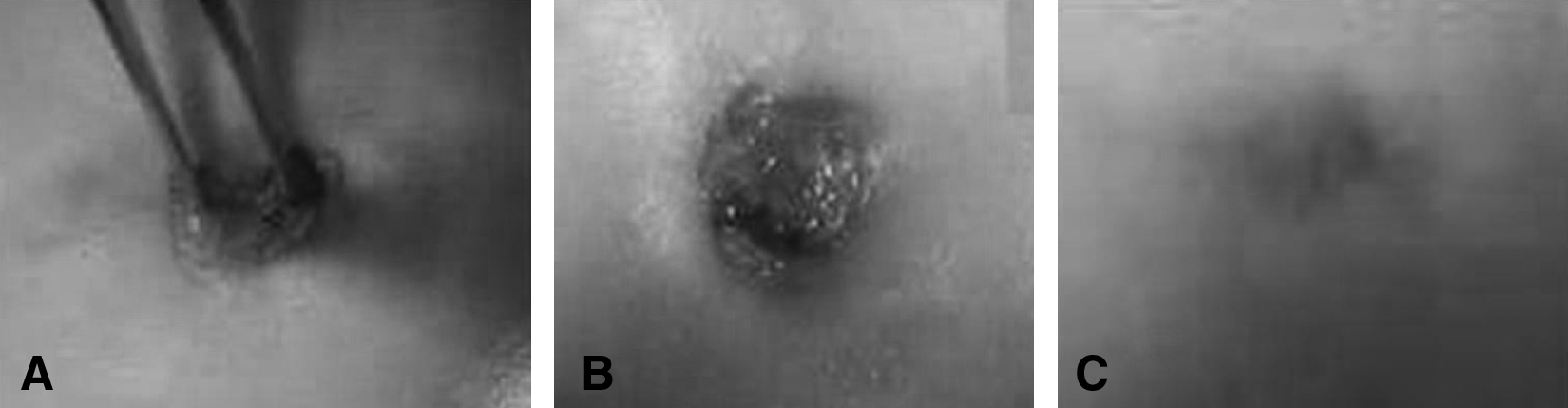
The GF site is cleaned with alcohol and adhesive remover to ensure that the orifice is clean, dry, and free of any foreign body. If granulation tissue is present, silver nitrate is applied prior to the application of 2OC. (
Diagnosis = diagnostic indication for gastrostomy tube placement; Age = age of child at first attempt of 2OC therapy; Type = type of procedure used to place gastrostomy tube; Size = size of gastrostomy tube; Time = number of months of indwelling gastrostomy tube before removal; Success = success of 2OC therapy; Follow-up = number of months for follow-up after last 2OC therapy.
Discussion
A gastrocutaneous fistula that fails to close spontaneously after GT removal is defined as persistent.1,8 A pGCF is associated with a number of situations, especially the length of time the GT is indwelling, with 45% of patients with a GT for greater than 6 months developing a pGCF. 8 The management of pGCF is often resource intensive, requiring a period of local wound care, followed by operative repair under general anesthesia. Cyanoacrylate tissue adhesives were first described in 1949 by Airdis, but those short-chain compounds caused local inflammation and had poor degradation properties. 3 The eight-carbon alkyl derivative, 2-octylcyanoacrylate (2OC), was designed as an alternative to correct some of these deficiencies.4–6 2OC has a breaking strength similar to that of a 5-0 monofilament suture, with improved cosmetic results, and it can be applied in an out-patient-setting clinic without local anesthesia. 4 The use of 2OC is very safe and efficacious, with rare reported adverse effects, including wound dehiscence, infection, and allergic skin reactions.4–6
The aim of this study was to analyze our recent experience in using 2OC tissue adhesive in the management of children with pGCF. We found that 2OC can successfully close pGCF in these patients. Four of the 7 children did not require operative intervention. None of the children suffered an adverse reaction to 2OC therapy. It does appear that, in this small study, 2OC therapy is more successful in children with smaller GT (less than or equal to 12–14 Fr) and a shorter indwelling time period (mean, 17.2 months). A larger study may be able to further differentiate other factors that may influence the efficacy of this technique.
Conclusions
This is the first study evaluating the utilization of 2OC as an occlusion technique for closure of children with pGCF. This technique was safe and effective in a majority of these patients. The 2OC technique is cost effective, can obviate the need for general anesthesia and can be performed in an outpatient setting. Additionally, the use of 2OC did not complicate subsequent surgical management of non-responsive pGCF. It should be considered as part of the initial management of this condition.
Footnotes
Disclosure Statement
No competing financial interests exist.