
Abstract
Abstract
Background:
The aims of this work were to introduce a two-port access (TPA) staging laparoscopy in gynecologic cancers and evaluate the feasibility and surgical outcomes of this operation.
Materials and Methods:
We performed 12 cases of TPA staging laparoscopy. The TPA system consisted of a single multichannel port at the umbilicus and an ancillary 5-mm port in the suprapubic area. Patient status was estimated in terms of operative morbidity and surgical outcomes.
Results:
All operations were completed laparoscopically, with no conversions to conventional laparoscopy or laparotomy. Procedures included endometrial cancer staging (n = 6), ovarian cancer staging (n = 3), 2 cases of type III radical hysterectomy, and 1 type II radical hysterectomy. Median patient age and body mass index were 48 years and 20.4 kg/m2, respectively. Median operation duration was 241 minutes (range, 188–360). Median estimated blood loss was 175 mL. Median number of lymph nodes obtained was 30 (range, 14–49). Median postoperative hospital stay was 8 days. There were no perioperative complications.
Conclusions:
TPA staging laparoscopy, using the single multichannel port system, could be a feasible procedure in selected gynecologic cancer patients, with only minimal skin incisions. Prospective, randomized trials will permit the evaluation of potential benefits of this minimally invasive surgical technique.
Introduction
Based on these considerations, we tried to perform appropriate cancer operations with minimal skin incisions by using a two-port access (TPA) system. This system consists of a single multichannel port system at the umbilicus, which had already been introduced by many surgeons, 8 and an ancillary 5-mm trocar in the suprapubic area. With the TPA system, we could minimize the number and size of skin incisions and perform proper surgical staging and optimal debulking for gynecologic cancers, including cervical, ovarian, and endometrial cancers, even if there were some technical problems. Although this study was preliminary, we expect the potential for improved surgical outcomes and better cosmetic results from these surgical techniques. The aim of this study was to introduce TPA staging laparoscopy, which was available for the gynecologic cancer operation, and to evaluate the feasibility of this operation.
Materials and Methods
This study was approved by the Institutional Review Board at Yonsei University College of Medicine (Seoul, Korea). We performed 12 cases of TPA staging laparoscopy for various gynecologic cancers, from May to October 2009, in our institute. Inclusion criteria were patients who had newly diagnosed untreated gynecologic cancers and needed lymph node dissection for surgical staging and treatment. All operations were performed by one surgical team.
Procedures included 6 cases of endometrial cancer staging, 3 cases of ovarian cancer staging, and 2 cases of type III radical hysterectomy, in 1 cervical cancer patient and 1 endometrial cancer patient with cervical extension, and 1 case of type II radical hysterectomy in metastatic cervical cancer from the stomach. All patients underwent pelvic lymph node dissection, and 11 of the 12 cases underwent para-aortic lymph node dissection. In endometrial cancer staging, the procedures included an extrafascial hysterectomy, a bilateral salpingo-oophorectomy, and a pelvic and para-aortic lymph node dissection. In ovarian cancer staging, an infracolic omentectomy was added to the procedures mentioned above. Two young patients with early ovarian germ-cell tumor underwent a unilateral salpingo-oophorectomy and surgical staging procedures for saving fertility, instead of a hysterectomy and bilateral salpingo-oophorectomy (Table 1).
BMI, body mass index; EBL, estimated blood loss; USO, unilateral salpingo-oophorectomy; PLD, pelvic lymph node dissection; PALD, para-aortic lymph node dissection; IO, infracolic omentectomy; NA, not available; EH, extrafascial hysterectomy; BSO, bilateral salpingo-oophorectomy; RH, radical hysterectomy.
Patient status was estimated in terms of body mass index (BMI), type and length of surgery, estimated blood loss, uterine weight, yield of lymph node, postoperative pain, postoperative length of hospital stay, and wound examinations after 6 weeks postoperatively. Operative times were defined as the interval from umbilical skin incision to completion of skin closure. Postoperative pain assessments were performed, in all patients, using a validated Visual Analog Pain (VAP) scale. The scale was presented as a score from 0 to 10, with verbal descriptors anchored with “no pain” and “agonizing pain.” Patients were asked to rate their pain intensity immediately after surgery in the recovery unit and at 6, 24, and 48 hours after surgery.
Surgical techniques
Patient preparation
Patients received prophylactic antibiotics 30 minutes before the operation. Patients were placed in the lithotomy position, and a general endotracheal tube with anesthesia was applied. A RUMI® uterine manipulator was placed with a KOH colpotomizer™ system (Cooper Surgical, Trumbull, CT) in 10 patients who underwent a hysterectomy. In the 2 cases, uterine manipulators were placed in the uterine cavity.
Two-port system using single multichannel port
After a 1.5-cm vertical intra-umbilical skin incision, a 1.5-cm rectus fasciotomy was performed to enter the peritoneal cavity. An Alexis® wound retractor (Applied Medical, Rancho Santa Margarita, CA) was inserted into the peritoneal cavity through the umbilicus. A 7½ surgical glove was fixed to the outer ring of the wound retractor. After making a small incision in one of the fingertip portions of the glove, a 5-mm trocar was inserted and moved into the abdominal cavity. The abdomen was insufflated with carbon-dioxide (CO2) gas of about 2 L, and a rigid, 30-degree, 5-mm laparoscope was inserted. After inspection of the pelvic cavity, we made two more holes at the fingers of the surgical glove for a 5-mm port and an 11-mm port for operating instruments. The 5-mm port for the laparoscope was used for insufflating CO2 gas. Another 5-mm trocar, in the suprapubic area, was used as the assistant port for the procedures and ventilating of CO2 gas (Fig. 1). Surgical instruments used were bipolar forceps, monopolar scissors, atraumatic forceps, a toothed grasper, a laparoscopic needle holder, a suction-irrigation system, an ultrasonic cutting and coagulating system (Harmonic Scalpel; Ethicon Endo-Surgery, Cincinnati, OH) and the LigaSure™ system (Valleylab, Boulder, CO).
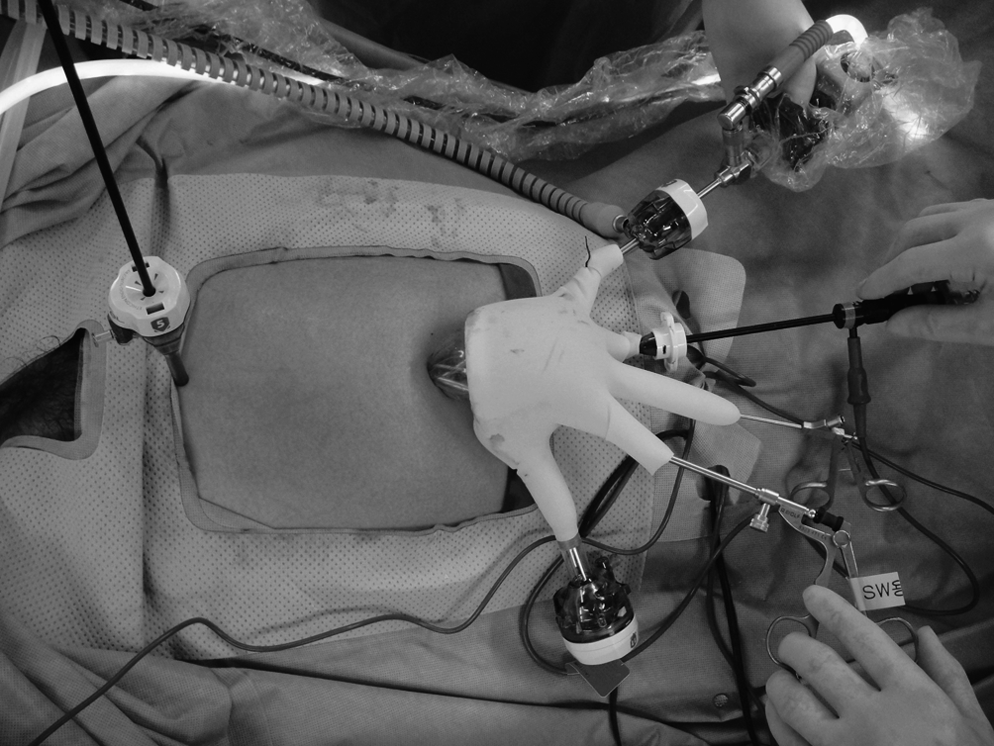
External view during a two-port access staging laparoscopy.
Staging laparoscopy procedure
Pelvic washings for the cytology examination were performed in all cases. For the pelvic lymph node dissection, the retroperitoneal space was developed by incising the peritoneum lateral to the infundibulopelvic ligament from the pelvic brim to the round ligament, using a monopolar hook. The paravesical and para-rectal spaces were identified. After the pelvic vessels and bilateral ureters were identified, pelvic lymph nodes were isolated and removed by incising tissue that was lateral and parallel to the external iliac artery, extending from the bifurcation of the common iliac artery to the point where the deep circumflex iliac vein crosses over the external iliac artery. Then, lymphatic tissues in the obturator fossa and on the internal iliac vessels were dissected (Fig. 2A).

Intraoperative view of a two-port access staging laparoscopy. (
For the hysterectomy, the round ligaments were ligated bilaterally, and bilateral infundibulopelvic ligaments were securely skeletonized and transected by using the LigaSure system after the identification of the ureters. The anterior and posterior leaves of the broad ligament were excised with a monopolar hook. The bladder and the attached peritoneal flap were developed by using a monopolar hook. Both uterosacral ligaments were excised with the monopolar hook, and the peritoneum on the posterior cervix was excised and divided from the cervix. The anterior and posterior colpotomy were performed, with the monopolar hook in the vagina delineated with the colpotomizer. Then, both uterine vessels were skeletonized and desiccated with the LigaSure system (Fig. 2B). Once the bladder was dissected below the colpotomy cup, a circumferential colpotomy was performed, using the monopolar hook.
We performed a type III radical hysterectomy in 2 patients. For the radical hysterectomy, the uterine vessels were dissected at their origins from the internal iliac vessels. The vesicocervical space was developed inferiorly and laterally. The medial edge of the divided uterine vessels was then pulled medially, and the ureter was completely freed from the retroperitoneal bed to the entry into the bladder by a complete dissection of the vesicouterine ligament. The cardinal ligament was transected at the medial wall of the internal iliac vessels. The anterior parametrium was transected near the bladder wall, and the posterior parametrium, including the uterosacral ligament, was divided midway from its origin of the uterus to the sacrum, until the bulge from the colpotomizer second lower ring in the vagina was reached. After completely detaching the uterus from the vagina, the uterus was extracted through the vagina. The pneumoperitoneum was maintained with a surgical glove filled with normal saline. A 40-mm, round-bodied needle was introduced through the 11-mm port, and we performed the closure of the vaginal cuff intracorporeally with a 1-0 Vicryl continuous running suture.
Para-aortic lymph node dissection was performed by using a monopolar hook and a Harmonic Scalpel. The peritoneal incision extended from the aortic bifurcation up to the transverse duodenum. After the inferior mesenteric artery and bilateral ureters were isolated, lymphatic tissues on the para-aortic, paracaval, and presacral spaces were carefully dissected (Fig. 2C). We performed an infracolic omentectomy in 3 patients with ovarian cancer. We divided the infracolic omentum along its superior border, just adjacent to the transverse colon, and provided hemostasis along the line of resection by using a Harmonic Scalpel (Fig. 2D). The resected omentum was extracted through the vagina with the uterus after the hysterectomy. In 1 patient, who did not undergo a hysterectomy, the omentum was extracted through an 11-mm port. The drainage bag was connected through the 5-mm port in the suprapubic area. After hemostasis, the single multichannel and ancillary ports were removed, and the umbilical fascia and subcutaneous tissue was approximated with 2-0 Vicryl sutures.
Results
Twelve TPA staging laparoscopic surgeries (6 endometrial cancer staging, 3 ovarian cancer staging, and 3 radical hysterectomy) were completed, with no conversions to conventional laparoscopy or laparotomy. Median patient age and BMI were 48 years (range, 16–62) and 20.4 kg/m2 (range, 17–27.3), respectively. Median operation time was 241 minutes (range, 188–360). Median estimated blood loss was 175 mL (range, 50–500). Two cases needed blood transfusions both intra- and postoperatively. Median uterus size was 144 g (range, 63–280). Median number of pelvic and para-aortic lymph nodes obtained was 30 (range, 14–49), and no patients had metastatic nodal disease (Table 1). Intravenous patient-controlled analgesia was given to 10 of the 12 patients. The median pain score, measured immediately after surgery in the recovery unit, was 3 (range, 2–5). The median postoperative pain scores, after 6, 24, and 48 hours, were 3 (range, 0–7), 3 (range, 0–4), and 2 (range, 1–4), respectively (Table 2). Median postoperative hospital stay was 8 days (range, 4–16). In 4 patients, who received postoperative adjuvant chemotherapy, postoperative hospital stay was calculated until the day before starting chemotherapy. There were no operative complications, such as bowel, urinary tract, and vessel injuries, and no port-site metastases were noted. Vaginal vault and abdominal wounds cleanly healed in all patients without any complications (Fig. 3A, B).

Postoperative photograph of abdominal skin incision. (
IV-PCA, intravenous patient-controlled analgesia.
Discussion
Laparoscopic operations have already been widely used for gynecologic diseases for decades, since a laparoscopic tubal ligation for contraception had been performed. 9 In the field of gynecologic oncology, applications of the laparoscopic surgical approach have increased, and surgical techniques of this operation have been improved gradually. Malur et al. described results about laparoscopically assisted radical vaginal versus radical abdominal hysterectomy type II in patients with cervical cancer. 6 Scribner et al. and Childers et al. demonstrated the feasibility of laparoscopic pelvic and para-aortic lymphadenectomy in gynecologic malignancies.4,5 In addition, Chi et al. showed a case control study of staging in early ovarian cancer, with 20 patients staged by laparoscopy, compared with 30 patients staged by laparotomy. 7 Recently, with the increased interest in MIS surgery and the innovation of technique and instrumentation for laparoscopy, an embryonic natural orifice transluminal endoscopic surgery, or a single-port access (SPA) laparoscopic surgery, has been developed. 10 Although it would take a long time for this surgical approach to be used popularly, due to technical difficulties, currently, a study of laparoendoscopic single-site surgery for the treatment of various cancerous and precancerous gynecologic conditions was demonstrated, 11 as well as SPA laparoscopy for benign gynecologic disease, such as SPA total laparoscopic hysterectomy or SPA adnexal surgery.8,12–14
Several laparoscopic surgeons have accumulated experiences and surgical skills for the SPA laparoscopic approach, and the approach of “better surgical outcomes with minimal incision” has been one of the principal objectives for laparoscopic operation. However, several main concerns have limited the widespread use of SPA laparoscopy in gynecologic cancers, due to their technical problems for performing specific procedures for cancers. SPA surgery has its systemic limitations, such as a crush between instruments and a limited amount of instruments, including the weaknesses of conventional laparoscopy, such as an unstable camera platform, the limited mobility of straight laparoscopic instruments, and two-dimensional imaging. These limitations, of course, negatively affect surgical performance in cancers, such as inadequate staging, spillage of cancer cells, including ovarian cyst rupture, and port-site metastases.
Robotic surgery, as one of the modalities for the cancer operation, is advantageous, because it overcomes the weaknesses of laparoscopy described above and has been gradually used for performing gynecologic cancer operations. A robotic-assisted radical hysterectomy and lymphadenectomy, in patients with cervical and endometrial cancer, was introduced and various studies using robotic systems have been published.15,16 Although it is not obvious that robotic surgery is superior to conventional laparoscopic surgery, in terms of surgical outcomes, these studies show the potential of robot-assisted laparoscopic surgery in the field of gynecologic cancers. However, robotic surgery still needs several skin incisions for robotic arms and assistants and, also, could have the same disadvantages of conventional laparoscopic surgery due to these incisions.
In the current study, we aimed to appropriately perform cancer operations with the minimally invasive approach and to surmount the technical problems of SPA, at the same time. So, we performed a TPA staging laparoscopy by employing a single multichannel port system with only minimal skin incisions. This TPA system enabled us to minimize skin incisions and complications from ancillary port placement. In our system, the ancillary 5-mm port, in the suprapubic area, was used not only by the assistant for traction, suction, and irrigation, but also by the operator for suturing and dissection. In particular, traction of the peritoneum and lymphatic tissues for pelvic and para-aortic lymph node dissection was performed through this ancillary port. Moreover, we perfectly performed an infracolic omentectomy with a Harmonic Scalpel and grasper through a single multichannel port at the umbilicus after the insertion of a 5-mm laparoscope through the ancillary port in the suprapubic area. Abdominal exploration also could be easily done in our system. Basically, an operator for this operation is needed to have surgical skills to perform procedures in the SPA system without technical difficulties. The median number of lymph nodes resected in our study was 30, and this number was sufficient, compared to the results of other studies with a conventional laparoscopic or robotic approach.4,17,18 Pelvic and para-aortic lymph node dissection was possible without any technical problems. In several patients, the upper para-arotic lymph node dissection, extended to the renal-vein level, was performed, although we had some troubles, due to difficulty in traction of the bowel and the limited angle of laparoscopic view. However, we could overcome this problem by using the 5-mm-sized laparoscopic articulating fan retractor (Tekno Medical, Tuttlingen, Germany). As a result, the use of our two-port system allowed us proper staging procedures, such as infracolic omentectomy, lymph node dissection, and abdominal exploration in reasonable operation times. Ultimately, better surgical outcomes, including decreased blood loss, decreased need for transfusion, and a shorter hospital stay are, potentially expected. Other advantages of our TPA system include enhanced cosmetic results from a hidden umbilical scar and minimal skin incisions, a decrease in morbidity related to bowel and vascular injury during trocar placement, and decreased postoperative wound infection and hernia formation. The median pain score, measured immediately after surgery in the recovery unit, and at 6, 24, and 48 hours after surgery, did not exceed 3 in the VAP scale. We could regard this score as a favorable result, in our experience. It is uncertain whether the TPA system is associated with a reduction in objective pain scores over conventional laparoscopy, as there have been no trials to compare with other surgical approaches.
Conclusions
The TPA staging laparoscopy, using single multichannel and 5-mm ancillary ports, could be a feasible procedure in selected gynecologic cancer patients, with only minimal skin incisions. Prospective, randomized trials will permit the evaluation of potential benefits of this MIS technique.
Footnotes
Disclosure Statement
No competing financial interests exist.