
Abstract
Abstract
Background:
Laparoscopic surgery may affect peritoneal physiology. Short-term laparoscopic surgery does not affect peritoneal transforming growth factor beta (TGF-b1) expression. The current study was conducted to evaluate the hypothesis that prolonged laparoscopic surgery may affect peritoneal TGF-b1 expression.
Study Design:
In the first study, 24 patients scheduled for a right colonic resection were enrolled in the trial. Twelve underwent conventional surgery (CCR) and 12 were operated on laparoscopically (LCR). In the second study, 12 patients undergoing laparoscopic gastric bypass (LGB) surgery for morbid obesity were included. Biopsies of the parietal peritoneum were taken at standardized moments during the procedures. Tissue concentrations of active and total TGF-b1 were measured by using enzyme-linked immunosorbent assays.
Results:
During the LCR, there was a significant increase in peritoneal active TGF-b1 levels (P < 0.05). A similar, but not significant, trend was observed during the CCR. A similar pattern was seen in the total TGF-b1 concentrations during both procedures. The LGB procedure did not affect peritoneal active or total TGF-b1 concentrations. During the procedure, both the active and total TGF-b1 levels were significantly higher in the LCR, when compared to the LGB, group (P < 0.05).
Conclusions:
Prolonged laparoscopic surgery may affect peritoneal TGF-b1 expression, depending on the procedure performed. Considering the role of TGF-b1 in various biologic processes, including adhesiogenesis and oncology, these results may have clinical consequences.
Introduction
Activation of peritoneal inflammation and modulation of the immune response following laparoscopic surgery eventually regulates the peritoneal healing processes. Peritoneal mesothelial cells produce multiple cellular mediators, including transforming growth factor beta (TGF-b) that, in turn, regulates the response of other cells. 9 TGF-b stimulates fibroblasts to produce many proteins, including collagen, fibronectin, and integrins, and decreases the production of proteins whose function is to degrade the extracellular matrix, such as collagenase and heparinase. A variety of studies support the concept that TGF-b is crucial in peritoneal healing and subsequent adhesion formation. TGF-b increases the production of plasminogen activator inhibitor and stimulates extracellular matrix deposition, resulting in an accumulation of connective tissue.10–12 The relation between TGF-b and adhesion formation has been established by various studies demonstrating elevated levels of TGF-b in areas of adhesion formation in humans.13,14 Additionally, Freeman et al. have shown, in an experimental study, that peritoneal adhesions have increased levels of TGF-b1 and beta3 mRNA transcripts, compared with both uninjured and normally healed peritoneum. 15
In a previous study in patients undergoing a laparoscopic cholecystectomy, we have shown that short-term laparoscopy does not affect the peritoneal levels of TGF-b1. 16 In that study, however, the timing of the final biopsy might have been too short to detect any effect of laparoscopic surgery on the production of TGF-b1. The use of an ultrasonic scalpel, frequently used in laparoscopic surgery, decreased the levels of TGF-b1, compared to electrocautery, while the intensity of light used to illuminate the peritoneal cavity and the temperature of carbon dioxide (CO2) also affected local concentrations of TGF-b1.16,17 The current study was conducted to evaluate the hypothesis that prolonged laparoscopic surgery (i.e., over 1 hour) may affect peritoneal TGF-b1 expression and that the extent of surgical trauma might influence this response. Considering the involvement of TGF-b1 in oncologic and peritoneal repair processes, this could have clinical consequences.
Materials and Methods
The present study consisted of two clinical experimental studies. In study 1, 24 patients scheduled for a right colonic resection were enrolled. Half of these were operated on laparoscopically and the others through a laparotomy. The choice of operation was based upon the experience of the treating surgeon and the preference of the patient. In the second study, 12 consecutive patients undergoing laparoscopic gastric bypass surgery for morbid obesity were included. All procedures were performed by experienced gastrointestinal surgeons. Institutional review board approval was obtained and written informed consent was given before enrollment.
Surgical protocols
Study 1
The conventional procedure (i.e., the CCR group) was performed through a midline laparotomy. First, the lateral parietal peritoneum was incised and the right hemicolon was mobilized. Then, the terminal ileum and colon where divided, using a linear stapler (GIA™; Autosuture, Gosport, UK). After, the mesocolon was divided and the specimen was removed. The ileum was sutured to the colon in a side-to-side manner, using a resorbable monofilament suture (PDS; Johnson & Johnson Medical BV, St-Stevens-Woluwe, Belgium), and the mesocolon was closed. Then, the fascia and skin were closed. The occurrence of adhesions, time of surgery, and timing of biopsies were recorded.
In the laparoscopic group (i.e., the LCR group), the procedure was started with an open introduction of the first trochar at the umbilicus. A pneumoperitoneum was established and three trochars were placed: two caudal from the umbilicus and one cranial. The colon was mobilized, and the mesocolon was divided. Subsequently, the colon was brought out through a 5–10-cm incision. Extra-abdominally, the terminal ileum and colon where divided by using a linear stapler. Then, a side-to-side anastomosis was performed in a similar way as during the CCR procedure. After, the bowel was brought inside the abdomen and the fascia and skin were closed. Again, the occurrence of adhesions, time of surgery, and timing of biopsies were recorded.
Biopsies of the parietal peritoneum were taken at three standardized moments during surgery. The first was taken immediately after access to the peritoneum. The second was taken after mobilization of the colon and division of the mesocolon. In the laparoscopic group, this implicated just before the minilaparotomy. The last was taken at the end of surgery. The biopsies were taken at a site remote from direct surgical trauma.
Study 2
Patient undergoing a laparoscopic gastric bypass (i.e., the LGB group) were positioned in the lithotomic position. After the establishment of a pneumoperitoneum, using a Veress needle in the left-upper quadrant of the abdomen, five trochars were placed. The stomach was sized into a small pouch, using a stapler device. The omentum was divided longitudinally to the level of the colon transversum. The jejunum was then anastomozed side to side approximately 20 cm after the ligament of Treitz to the pouch of the stomach. One hundred to 150 cm of length of the jejunum was measured distal to this anastomosis and stapled side to side to the proximal jejunum. After, the bowel was divided between the gastrojejunostomy and the enteroenterostomy. The gastrojejunostomy was tested for leakage by applying air through a nasogastric tube. The occurrence of adhesions and time of surgery were recorded. Immediately after creating the pneumoperitoneum, a biopsy was taken from the parietal peritoneum in the right-upper quadrant. During the procedure, each 45 minutes, an additional biopsy was taken from the parietal peritoneum. All biopsies were taken at a site remote from direct surgical trauma.
Tissue sampling and processing
The peritoneum was carefully dissected, taking care not to include the underlying muscle. The tissue specimens were snap-frozen in liquid nitrogen and stored at −70°C until further processing. Before homogenizing, a sample of thawing peritoneal tissue was cut off before being blotted and weighed. Each biopsy was rinsed with phosphate-buffered saline (PBS) with 0.5 M of sodium chloride (pH 7.4), cut into small pieces, and placed into ice-cold homogenization buffer (PBS with 0.01% Triton X-100; Sigma, St.Louis, MO) in a final concentration of 40 mg tissue/mL of buffer. The tissue was homogenized for 60 seconds on ice, using a Polytron homogenizer (Ultra Thurrax IKA T-25; Janke & Kunkel, Staufen, Germany), centrifuged at 10,000 × g for 4 minutes at 4°C, and the supernatant was stored at −70°C until further analysis. Tissue processing and assays were performed in batches.
Biochemical assays
Concentrations of active and total TGF-b1 were measured by using commercially available (R&D Systems, Abingdon, UK) enzyme-linked immunosorbent assays (ELISA). Both the active and total form of TGF-b1 were measured, since TGF-b is inactive when produced, and has to be activated to become an active cytokine. The active and total amounts of TGF-b1 were performed in separate steps: First, the active fraction of TGF-b1 were assayed directly in the ELISA plate, and, second, the total amount of TGF-b1 was assayed by acidifying the samples with 1 mol/L HCL to pH 3, followed by a 15-minutes incubation at 22°C, resulting in an activation of TGF-b1. To neutralize samples, 1 mol/L of NaOH were supplemented before addition to the ELISA plate, according to the instructions from the manufacturer. The lower detection limit for the TGF-b1 assay was 32 pg/mL. The intra-assay variation was 3.3–4.5% (CV%), and the interassay variation was 7.6–19.1%. Additionally, results were normalized to total protein content, using a commercial protein assay (Bio-RAD, Hercules, CA).
Statistics
Values are presented as mean and standard deviation. Analysis of differences between groups was performed from using the Friedman and the Mann-Whitney U tests. All tests were two-tailed. A P-value of less than 0.05 was considered to be significant.
Results
Clinical results
In the right colonic resection study, there was no difference in gender between groups. The male; female ratio was 1:4. The mean age of patients was 55 ± 20 years in the laparoscopic and 72 ± 10 in the conventional group (P < 0.05). The indication for surgery was malignancy or dysplastic lesion in 17 patients and inflammatory bowel disease in 7 patients, without significant differences between groups. Further, there were no differences in the incidence of previous laparotomy or the occurrence of intraperitoneal adhesions during surgery. In the conventional group, the first biopsy was taken immediately after opening the abdomen. Mobilization of the colon and division of the mesocolon was completed after 26 ± 16 minutes of surgery. The last specimen was taken after 54 ± 16 minutes. In the laparoscopic group, the first biopsy was taken immediately after initiating the pneumoperitoneum, the second biopsy after 41 ± 13 minutes of surgery, and the last after 78 ± 12 minutes.
Patients included in the gastric bypass study had a mean age of 38 ± 9 years and an average body mass index of 49 ± 8 kg/m2. There was an equal distribution between men and women. Four patients had previously undergone a laparoscopic gastric banding, and 1 of them also underwent a laparoscopic cholecystectomy. Two others had a history of laparoscopic cholecystectomy, and 1 of them also underwent a laparoscopic appendectomy. The average operation time was 183 ± 35 minutes. In 1 patient, the procedure was converted to a laparotomy, after 135 minutes of laparoscopic surgery, due to extensive adhesion formation after a previous gastric banding.
Biochemical results
Study 1
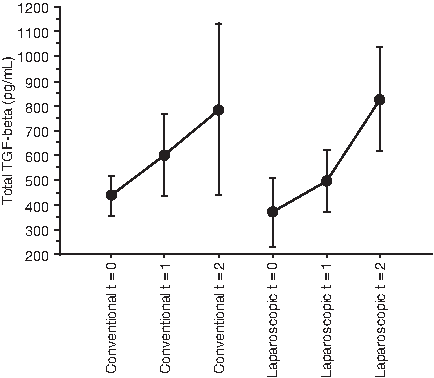
In the CCR group, the active TGF-b1 concentration in samples taken immediately after initiating the procedure was 102.2 ± 22.7 pg/mL (Fig. 1). During the procedure, levels increased by 46% to 149.7 ± 60.8 pg/mL at the end of the procedure. This trend did not reach statistical significance. In the LCR group, the initial peritoneal active TGF-b1 levels were 82.8 ± 41.4 pg/mL. During the laparoscopic procedure, a 60% increase was noted after the mobilization of the hemicolon (P = 0.01) and a 120% rise at the end of the procedure (P = 0.04). At none of the measured time points were there significant differences between the LCR and CCR groups with regard to active TGF-b1. When normalizing the values to the total protein content of the samples, the results where comparable with result per milligram of homogenized tissue, except for time point t1. At that time point, the active fraction of TGF-b1 was significantly higher in the laparoscopic, compared to the conventional, group (P = 0.01). After mobilization of the hemicolon and at the end of surgery, the levels were similar in both groups, again.

Active transforming growth factor beta 1 (TGF-b1) concentrations in peritoneal samples taken at the start of surgery (t = 0), after mobilization of the colon (t = 1), and at the end of surgery (t = 2) in patients operated on conventionally and laparoscopically. Data are presented as mean and standard error. *P < 0.05, compared to t0 values.
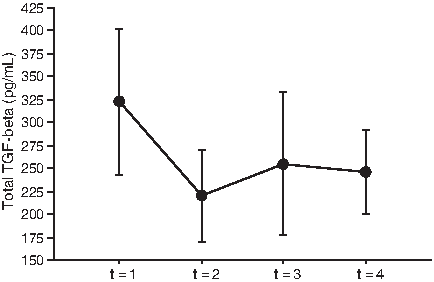
The total concentration of TGF-b1 was 370.6 ± 136.8 immediately after initiation of the procedure in the LCR group (Fig. 2). During the procedure, a 2-fold increase was observed, to 827.1 ± 212.5 (P = not significant). A similar pattern was observed in the conventionally operated group. At the end of the procedure, the levels of total TGF-b1 had increased by 1.8-fold, compared to the concentrations at the initiation of surgery. Again, there were no differences in any of the measured time points between the LCR and CCR groups. Similar results were obtained when the values had been normalized to the total protein content of the samples.
Total transforming growth factor beta 1 (TGF-b1) concentrations in peritoneal samples taken at the start of surgery (t = 0), after mobilization of the colon (t = 1), and at the end of surgery (t = 2) in patients operated on conventionally and laparoscopically. Data are presented as mean and standard error.
Study 2
In patients undergoing an LGB, another pattern was observed. The active peritoneal TGF-b1 concentration immediately after insufflation was 65.5 ± 20.8 pg/mL (Fig. 3). During the 135 minutes of laparoscopic surgery, there were no significant changes in active TGF-b1 expression. The total TGF-b1 concentrations also remained at the same level during the entire surgical procedure (Fig. 4). Additionally, when normalized to the total protein content of the sample, the concentrations of both active and total TGF-b1 did not change during the entire surgical procedure. There were no significant differences in both active and total TGF beta-1 between patients with and without adhesions and patients with or without inflammatory bowel disease.

Active transforming growth factor beta 1 (TGF-b1) concentrations in peritoneal samples measured immediately after initiation of the procedure and every 45 minutes during a laparoscopic gastric bypass. Data are presented as mean and standard error.
Total transforming growth factor beta 1 (TGF-b1) concentrations in peritoneal samples measured immediately after initiation of the procedure and every 45 minutes during a laparoscopic gastric bypass. Data are presented as mean and standard error.
Study 1 versus 2
When comparing both studies, the initial levels of both the active fraction and the total amount of TGF-b1 were within the same range. When comparing the active TGF-b1 levels in samples taken after 45 minutes in the LGB group with, respectively, the 41- and 78-minute samples of the LCR group, significantly higher concentrations were observed in the latter (P = 0.02 and 0.02, respectively) (Fig. 5). The same was true for the total concentrations of TGF-b1: Significantly higher levels were observed in samples taken at either 41 or 78 minutes of surgery in the LCR group, when compared to the 45-minute samples in the LGB group (P = 0.02 and 0.01, respectively) (Fig. 6).
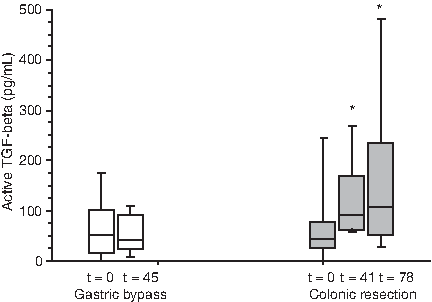
Active transforming growth factor beta 1 (TGF-b1) concentrations in peritoneal samples taken at the start of surgery and after 45 minutes during a LGB procedure (open boxes) and at start of surgery and after, respectively, 41 and 78 minutes of surgery during an LCR procedure (grey boxes). Values are median (horizontal line), interquartile range (boxes), and 10th and 90th percentiles (error bars). *P < 0.05 LGB versus LCR procedure.
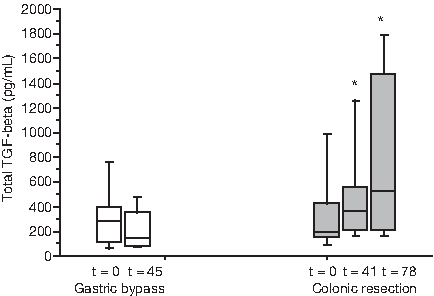
Total transforming growth factor beta 1 (TGF-b1) concentrations in peritoneal samples taken at the start of surgery and after 45 minutes during an LGB procedure (open boxes) and at start of surgery and after, respectively, 41 and 78 minutes of surgery during an LCR procedure (grey boxes). Values are median (horizontal line), interquartile range (boxes), and 10th and 90th percentiles (error bars). *P < 0.05 LGB versus LCR procedure.
Discussion
In the present study, we have demonstrated that peritoneal TGF-b1 expression may be influenced by prolonged laparoscopic surgery, depending on the type of procedure performed. During a laparoscopic right hemicolectomy, a significant increase in active TGF-b1 was observed, while during laparoscopic gastric bypass, levels remained unaltered. The difference observed between the LGB and LCR procedure may be explained by different factors. First, the extent of surgical trauma to the peritoneum may have contributed. During an LCR, the right hemicolon is mobilized, creating a large peritoneal defect. During a LGB procedure, the extent of peritoneal trauma is conceivably lower. The extent of surgical trauma may be crucial, since it initiates an inflammatory reaction, leading to fibrin deposits on the peritoneal surface and activating several cell types that modulate peritoneal healing.4,5 A second explanation may be the patient population included in both studies. It may be debatable whether the results obtained from morbidly obese patients reflect general surgical practice. The same may be true, however, for studies in patients suffering from an inflammatory bowel disease or malignancy, making generalizations difficult. In the present study, the number of treated patients was too small to draw any conclusions on the possible effect of underlying pathology. It is known that morbid obesity is characterized by alterations in immune and inflammatory functions. O'Rourke et al. showed elevated levels of cytokines in peripheral blood samples and altered blood lymphocyte function.18,19 This modulated inflammatory state is important in the pathogenesis of much obesity-related comorbidity. To our knowledge, a variation in peritoneal wound healing between an obese and a healthy population has never been described. The same is true for adhesion formation; obesity has never been proposed as a risk factor for peritoneal adhesion formation. Further studies elucidating this subject appear indicated.
In the present study, we observed a significant increase in active TGF-b1 during the LCR procedure. During the CCR procedure, a similar pattern was seen. At the end of the procedure, the levels of active TGF-b1 were 50% higher, compared to the initial levels. This trend, however, did not reach statistical significance, possibly due to the relatively small sample sizes and wide standard errors. The same may be true for the total TGF-b1 concentrations during both LCR and CCR procedures: A trend toward increased levels was observed. Surprisingly, the increase in active TGF-b1 in the CCR group appeared to be lower, compared to the 120% increase in the LCR group. Surgical trauma to the peritoneum is believed to be larger in conventional than in laparoscopic surgery. The role of laparoscopy in peritoneal healing has been emphasized by Ordoñez et al., who found that duration of laparoscopic surgery significantly influenced pneumoperitoneum-related adhesion formation in an animal model. 7 A combination of surgical and pneumoperitoneum-related trauma, might have caused an altered immune response, creating a higher increase in the LCR group. Further studies focusing on the combination of various types of peritoneal trauma are indicated. Patients described in the colonic resection study were clinically identical, except for age of patients, which was significantly higher in the CCR group. This difference, however, is unlikely to have affected the biochemical results, since an age-related change in peritoneal TGF-b1 expression has never been described, to our knowledge.
Various studies have indicated the peritoneal plasmin system to be a key factor in peritoneal healing processes.4,5 Plasminogen activation is hampered by plasminogen-activating inhibitor types 1 and 2 (PAI-1 and 2). PAI-1 is the main inhibitor of tPA and uPA and is produced by a variety of cells, which also may produce plasminogen activators, including mesothelial cells. In free form, plasminogen activators are rapidly inactivated by PAI-1 by forming inactive one-to-one complexes. Increased PAI-1 levels have been associated with disturbed peritoneal healing and subsequent adhesion formation.20,21 In a previous study, we have observed that during an LGB procedure, the peritoneal levels of PAI-1 do not change, which is in accord with the present findings. 22 Results of the LCR study, however, are seemingly in contrast with previous observations on PAI-1 levels, wherein no significant changes were observed. However, when reanalyzing these data, a trend toward increased PAI-1 levels was seen in the LCR group, which is in accord with the present observations, since TGF-b1 is a main stimulator of PAI-1 production.
The increased TGF-b1 levels during the LCR procedure might have clinical consequences. Besides its role in peritoneal healing and subsequent adhesion formation, TGF-b1 is important in various biological processes, including oncologic processes, by regulating chemotaxis, mitogenesis, and angiogenesis.23–25 Malignancies are a main indication for various laparoscopic procedures, including colonic resection, nefrectomy, and hysterectomy. Experiments have suggested that laparoscopy may be correlated with decreased intraperitoneal tumor growth, compared to open surgery.26,27 Insufflation with CO2, however, has been described to promote peritoneal tumor growth, when compared to gasless laparoscopy. In another experimental study, however, no deleterious effects of CO2 insufflation on ovarian tumor growth were observed, when compared to gasless laparoscopy or midline laparotomy, in a rat model. 28 It is still unclear whether these experimental concerns may be translated into clinical problems. Taking into consideration the role of TGF-b1 in various oncologic processes, our results warrant further studies.
Conclusions
In conclusion, we have shown that prolonged laparoscopic surgery may affect peritoneal TGF-b1 expression, depending on the procedure performed. Considering the role of TGF-b1 in various biologic processes, including adhesiogenesis and oncology, these results may have clinical consequences.
Footnotes
Disclosure Statement
No competing financial interests exist.