
Abstract
Abstract
Introduction:
Rectal strictures in patients with Crohn's colitis are common and options described for their treatment include direct steroid injection, injection of tumor necrosis factor (TNF) inhibitors, endoscopic balloon dilatation, use of Hegar dilators, stricturoplasty, and proctectomy. Adequate treatment is a challenge, especially with respect to the prevention of stricture recurrence. We present an option for the surgical treatment of these strictures using a transanal resection of the rectum with the addition of laparoscopy or laparotomy.
Methods:
Three patients who had medically refractory or chronic Crohn's colitis with rectal strictures were referred to us after failed medical management, rectal dilation, and balloon dilation of the strictures. In each case, we performed a transanal sphincter preserving dissection in the prone position and used the lithotomy position for intraabdominal mobilization, completion of the rectosigmoid resection, pull-through of the left colon, and coloanal anastomosis.
Results:
We resected the rectal strictures transanally in all three cases. One case provided the opportunity to perform a laparoscopy-assisted procedure, whereas the other 2 patients had laparotomy-assisted rectosigmoid resections. We did a coloanal anastomosis in 2 patients with healthy left colon. In the third case, the anal canal was preserved, but the patient was left with a stoma.
Conclusions:
Transanal resection is feasible in the surgical treatment of rectal strictures in patients with Crohn's colitis. It preserves the anal sphincteric mechanism and may help in avoiding a permanent stoma in a subgroup of patients. We found the prone position very helpful in performing the transanal rectal dissection.
Introduction
The transanal approach has been popularized in the management of Hirschsprung's disease in children.7,8 We have recently reported the use of a similar technique in rectosigmoid resections for intractable idiopathic constipation 9 and for redo Hirschsprung's pull-throughs. 10 This technique is less invasive and can be used to remove even an inflamed and scarred rectum, and the anal sphincteric mechanism can be preserved in selected patients. In this case series we present 3 patients with Crohn's disease and rectal strictures managed with a transanal resection and compare the results to available literature.
Methods
Three patients aged 17, 17, and 21 years who had been treated for medically refractory or chronic Crohn's colitis and rectal strictures were referred to our institution. They had failed medical management, rectal dilation, and balloon dilation of the strictures. All 3 had been diverted (ileostomy in 2, colostomy in 1). One had developed a rectovesical fistula despite diversion. In each case, we performed a transanal sphincter preserving dissection ∼1.5 cm above the dentate line, in the prone position, and then packed the perineum with sterile gauze. We then flipped the patient supine and placed them in lithotomy position for intraabdominal mobilization, completion of the rectosigmoid resection, pull-through of the left colon, and coloanal anastomosis.
Results
Case 1
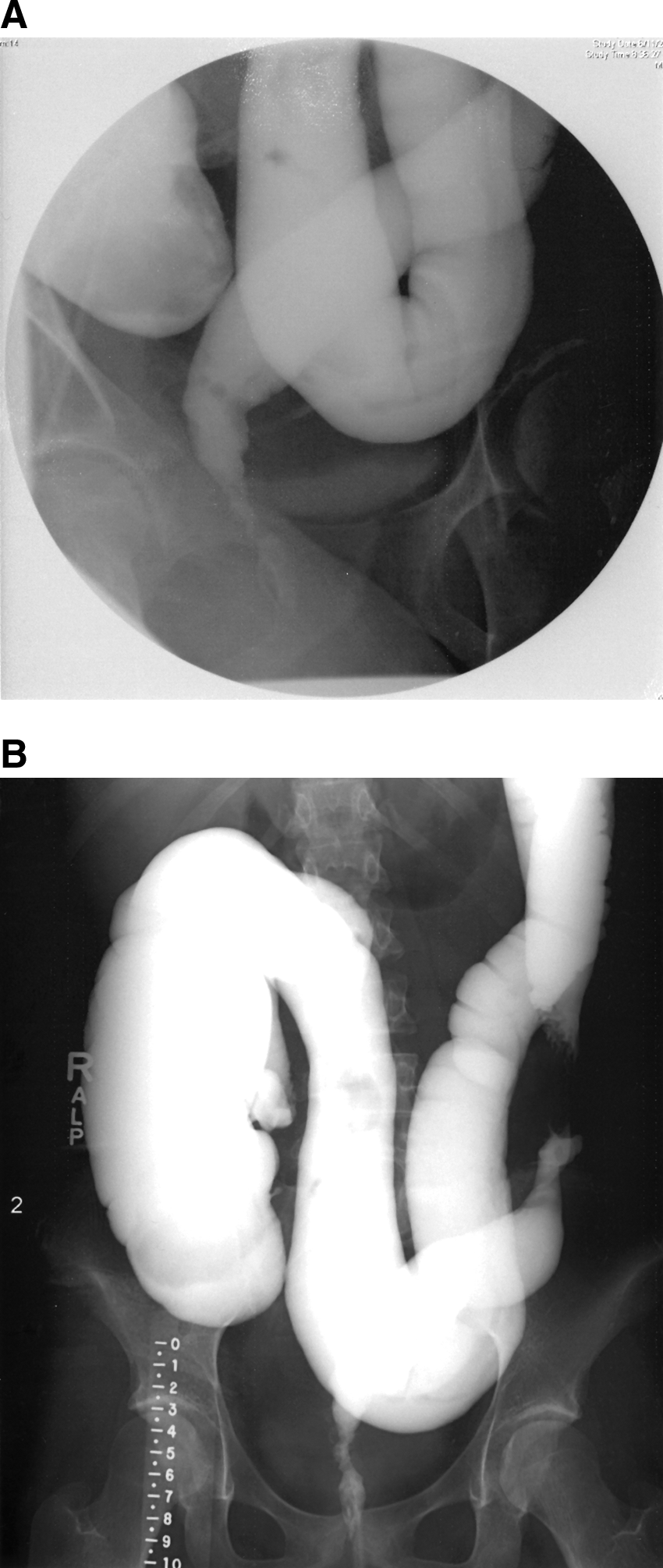
A 21-year-old woman was initially seen in our hospital and found to have Crohn's disease at the age of 11 years. She was managed on azathioprine and prednisone and followed for 10 years without significant active disease until 1 year prior to presentation when she developed chronic fever and weight loss. She was identified to have a rectal abscess associated with anal and rectal strictures. CT and MRI scans of the pelvis revealed fluid collections and inflammation around her upper rectum. Colonoscopy showed a strictured rectum and sigmoid at 4 and 20 cm from the anal verge, respectively, with prestenotic colonic dilatation. The strictures and rectal abscess persisted despite treatment with antibiotics and steroids, necessitating a laparoscopic diverting ileostomy. The pelvic fluid collection was noted to have resolved at the time of the laparoscopy. She responded well to the fecal diversion with weight gain but the strictures remained, as demonstrated on contrast enema (Fig. 1A, B).
(
A laparoscopic-assisted transanal resection of the rectum and sigmoid colon was done at 5 months after diversion. Laparoscopy confirmed a stricture at the mid-sigmoid colon. The descending colon, which was grossly normal, was mobilized up to the splenic flexure. Via a perineal, transanal dissection, a stricture 1 cm above the dentate line was found with a grossly diseased and friable rectum. The rectosigmoid was resected, pull-through of the descending colon was performed, and a coloanal anastomosis was done, preserving the anal canal and sphincter mechanism. The ileostomy was closed at 7 months postoperatively. She developed a recurrence of colitis in the pulled through segment at 6 months after ileostomy closure and was placed on anti-TNF therapy, in addition to metronidazole, to which she responded. She is now 13 months postileostomy reversal, is quiescent in terms of her Crohn's status, and has four formed stools daily, with no blood in the stool. She is gaining weight adequately.
Case 2
A 17-year-old girl had medically refractory Crohn's colitis and had received multiple courses of steroids, methotrexate, and infliximab. She presented at age 14 with a 1 year history of chronic fever, rectal pain, and pain with defecation. Examination under anesthesia revealed perianal abscesses and fistulae and a stricture 4 cm from the anal verge that could not admit a finger. She had a diverting sigmoid colostomy in healthy appearing colon (external appearance and endoscopic findings) to allow healing of the rectal disease. Repeat examination under anesthesia after 6 months showed resolution of the fistula and abscesses but the rectal stricture persisted. She had serial rectal dilations with Hegars and local injection of steroids. This was deemed to have provided adequate treatment as examination demonstrated that the stricture was soft, pliable, and accepted a No. 18 Hegar dilator. Subsequently, the colostomy was closed. After a transient improvement for 1 month, she developed recurrent perineal pain, difficulty with defecation, and abdominal pain necessitating creation of a new diverting sigmoid colostomy. Complications from the stoma ensued, including parastomal abscesses, mucus fistula retraction, and a wound dehiscence. She underwent drainage of the abscesses and the colostomy was revised. In view of the chronic problems related to the Crohn's colitis and the rectal stricture, she underwent a total abdominal colectomy with creation of an end ileostomy, leaving her with a Hartmann's pouch. She improved for 10 months but subsequently developed severe lower abdominal pain. An abdominal CT scan at that time showed a distended Hartmann's pouch and proctoscopy revealed a persistent stricture 4 cm from the anal verge and an inflamed rectum. The stricture was thought to be responsible for the accumulation of mucus in the Hartmann's pouch as well as the rectal inflammation, and a transanal resection of the rectum was planned. Operative findings included an extremely inflamed rectum densely adherent to the pelvis and a rectal stricture 2 cm from the anal verge. The initial approach was transanal; however, because of the dense adhesions to the pelvis, which disallowed full rectal mobilization, a laparotomy was performed for a completion proctectomy, leaving an intact anal canal. She had a wound infection in the early postoperative period but has done quite well afterward and is free of abdominal pain. She has been followed at this point for 15 months, and a future pull-through of the distal ileum remains an option.
Case 3
A 17-year-old boy with a history of Crohn's disease presented with intermittent crampy abdominal pain for 2 months, fever, and weight loss. Examination confirmed proctitis and a perirectal abscess. Examination under anesthesia revealed a rectal stricture 3 cm from the anal verge, and colonoscopy showed a stricture at 15 cm, beyond which the scope could not be passed. He was treated with steroids, antibiotics, and infliximab but there was no improvement, and he underwent a laparoscopic diverting ileostomy. The symptoms only improved mildly and his clinical condition was complicated by the development of a rectovesical fistula despite diversion. A transanal resection was performed. The distal stricture was contained within a large rectal inflammatory mass, which necessitated a combined laparotomy and transanal resection of the rectum and sigmoid colon with pull-through of the healthy proximal sigmoid colon. The operation was performed via a combined prone and then supine position (Figs. 2 and 3). For the transanal dissection a prone position was used, and for the colonic mobilization and coloanal anastomosis, the patient was in supine/lithotomy position. The rectovesical fistula was also repaired. He did well postoperatively, including significant weight gain and increase in linear growth. A recent contrast enema showed a normal caliber colon, examination under anesthesia demonstrated absence of a stricture, and ileoscopy as well as colonoscopy showed an absence of active disease. The anal canal and sphincters were preserved and demonstrated by his ability to hold contrast. He has been followed for 1 year and is scheduled for closure of the ileostomy.

The patient in the prone position used for transanal dissection.

Commencement of the transanal rectal dissection in the prone position with preservation of the anal canal.
Discussion
Although mild cases of Crohn's strictures may respond to medical treatment, more aggressive treatment is necessary to treat recalcitrant strictures. 2 The use of endoscopic balloon dilation with or without steroid injection has been advocated in the treatment of these strictures. 11 However, this has not been demonstrated to be of repeated success and perforations may occur. The use of this technique in long rectal strictures often does not succeed. 11 In a review of 29 upper and lower gastrointestinal tract strictures dilated through a scope balloon, a perforation rate of 10% with a long-term success rate of 76.5% was reported. 11 Another technique is the use of rectal dilators, typically Hegar dilators of varying sizes, which also has variable success. In a group of 33 patients with anorectal strictures in Crohn's disease managed by dilation, 13 did not respond to dilations and had to undergo proctocolectomy. 12 In another review of 9 patients with Crohn's disease and anorectal strictures managed with rectal dilation, 7 remained dependent on regular dilation every 2–6 months, 24–48 months after commencement of this modality of treatment. 13 Repeated dilation on its own is not risk free with potential morbidities including sphincter damage, perforation, and local sepsis. 13
Infliximab is another technique utilized in the treatment of strictures associated with Crohn's colitis. The anti-inflammatory properties of TNF inhibitors have been demonstrated to alleviate the symptoms associated with strictures.6,14 The results tend to be unsatisfactory in patients who have fibrotic strictures, which are likely to be dense, long standing, and unrelated to previous anastomosis 5 as in the patients presented in this review. Local injection of infliximab is a more recent attempt at reducing the side effects of systemic infusion as well as providing a more effective alternative. Although the efficacy has been demonstrated in a small series involving short segmental strictures in patients with obstructive symptoms, 2 it may not be helpful in patients with multiple or long segmental strictures, such as in two of the cases we have presented.
Strictureplasty has been used successfully for the treatment of small and large bowel strictures in Crohn's disease.4,15 This method of course is not technically feasible in rectal strictures.
Surgery has a major role to play in the management of rectal strictures complicating Crohn's disease, especially when there is proctocolitis. 12 This may be in the form of temporary diversion or definitive resectional treatment. Fecal diversion may be necessary to allow the inflammatory process in the colon and rectum to subside but may not be helpful for more than a temporary period of time. And despite diversion, local irritation can continue and lead to problems. Some have also reported cases illustrating that diversion in this group of patients may result in worsening of their symptoms. 16
Transanal pull-through has been popularized for the treatment of Hirschsprung's disease.7,8 A key component of the procedure involves preservation of the anorectal sphincter mechanism. We contemplated that for those patients with a Crohn's rectal stricture, a successful transanal resection can allow for a pull-through and preclude the need for a permanent stoma. We have noted that the approach has been useful for rectosigmoid resection in other conditions such as idiopathic constipation refractory to medical management 9 and redo pull-throughs for Hirschsprung disease, which often have a scarred rectum or a distal pull-through segment that needs to be removed. 10 When the mobilization cannot be completed from below, laparoscopy or laparotomy can be done to achieve a complete resection of the rectum with or without adjacent colon. A common fear is fecal incontinence, but because the anal canal and sphincter mechanisms are preserved intact, the ability of the patient to maintain continence is maintained.7–10
One of the most feared consequences of complicated Crohn's disease is the need for a permanent diversion. This is particularly so in patients with anorectal strictures in the setting of Crohn's colitis and proctitis.1,17,18 In one review, only 34% of a group of patients with anal canal stricture and Crohn's disease avoided a permanent diversion. 19 Two of our patients were able to avoid permanent ostomy largely because the healthy segment of bowel utilized in the pull-through was anastomosed to an intact anal canal with preserved sphincter mechanisms and therefore preserved function. The first patient did well in terms of bowel function but had a flare of colitis necessitating more aggressive treatment with TNF inhibitors. We take a very aggressive postoperative strategy using both immunomodulating agents, such as methotrexate or 6-mercaptopurine, as well as anti-TNF agents to try and limit or delay postoperative recurrence.20,21 We do not know yet whether the third patient can one day be pulled through and undiverted.
In view of the psychological and social effects of long-term stomas in children and adolescents, 22 procedures that will preserve anal canal functions and improve quality of life after a proctocolectomy for rectal strictures are worth considering in selected cases.
Conclusion
Transanal resection is a feasible approach to the surgical resection of the rectum affected by a stricture in the setting of Crohn's disease.
Disclosure Statement
No competing financial interests exist.