
Abstract
Abstract
Background:
Morbidity of small intestinal disease is rare and the associated lesion is hard to be detected due to lack of specific manifestations and effective diagnostic approaches. Hematochezia and melena are the most common symptoms in small intestinal diseases. Hence, small intestinal disease is an important differential diagnosis when hematochezia or melena occurs, especially when gastric and colonic diseases are excluded. As the small intestinal lesion is hard to be located preoperatively, laparotomy used to be performed without a preoperative location. This might lead to related postoperative complications. With the development of laparoscopic technique, laparoscopic operations are more frequently applied to surgical disease, despite their benign or malignant nature. Generally, almost all kinds of small intestinal disease can be treated with laparoscopic surgery.
Methods:
Clinical data of 77 patients with small intestinal bleeding undergoing laparoscopic or laparoscopy-assisted operations from April 2003 to December 2008 were included, and their clinical information were analyzed retrospectively.
Results:
No intraoperative complication or conversion was observed in all cases. The mean operative time, mean estimated blood loss, and mean size of incision were 78.3 ± 30.5 minutes, 17.5 ± 9.8 mL, and 3.3 ± 1.9 cm, respectively. Postoperative complications occurred in 4 patients, including 2 cases of adhesive ileus, 1 case of gastric retention, and 1 case of anastomotic bleeding. All of them were cured by nonoperative management. The mean flatus time was 2 days after operation and the mean postoperative hospital stay was 7 days. There was 1 case of gastrointestinal stromal tumor with local recurrence and hepatic metastasis. Four patients died from metastasis of malignant tumors during the follow-up from 2 to 70 months after operations. No trocar site or wound recurrences were noted.
Conclusions:
Laparoscopic treatment in small intestinal bleeding is feasible, safe, and minimally invasive. It may be widely used in the future for its good therapeutic outcomes and improved diagnostic chance in small intestinal bleeding diseases.
Introduction
Patients and Methods
Clinical data of 77 cases of small intestinal bleeding who underwent laparoscopic or laparoscopy-assisted operations from April 2003 to December 2008 were collected. There were 44 male and 33 female patients. Age ranged from 13 to 79 years, with a median of 51. The major clinical manifestation was gastrointestinal bleeding, including 71 with melena and 6 with hematochezia. Hemoglobin ranged from 36 to 140 g/L, with a mean of 78.2. Endoscopic examinations were performed preoperatively to exclude possible lesions in the stomach, colon, and rectum, and then, the small intestinal bleeding was taken into account after related examinations. Preoperative related examinations were as follows: double-ballon enteroscopy (DBE) (61/65 cases), capsule endoscopy (5/10 cases), abdominal computed tomography (CT) scan (22/42 cases), positron emission tomography (PET)/CT (5/12 cases), multislice spiral computerised tomography enteroclysis (MSCTE) (31/40 cases), and digital subtraction angiography (DSA) (3/5 cases) (Fig. 1). After the above examinations, the lesions were found in the small intestine in 76 cases. One showed false negative and was diagnosed as small intestinal tumor after a laparoscopic exploration. No metastasis was found by imaging analysis before the operation.
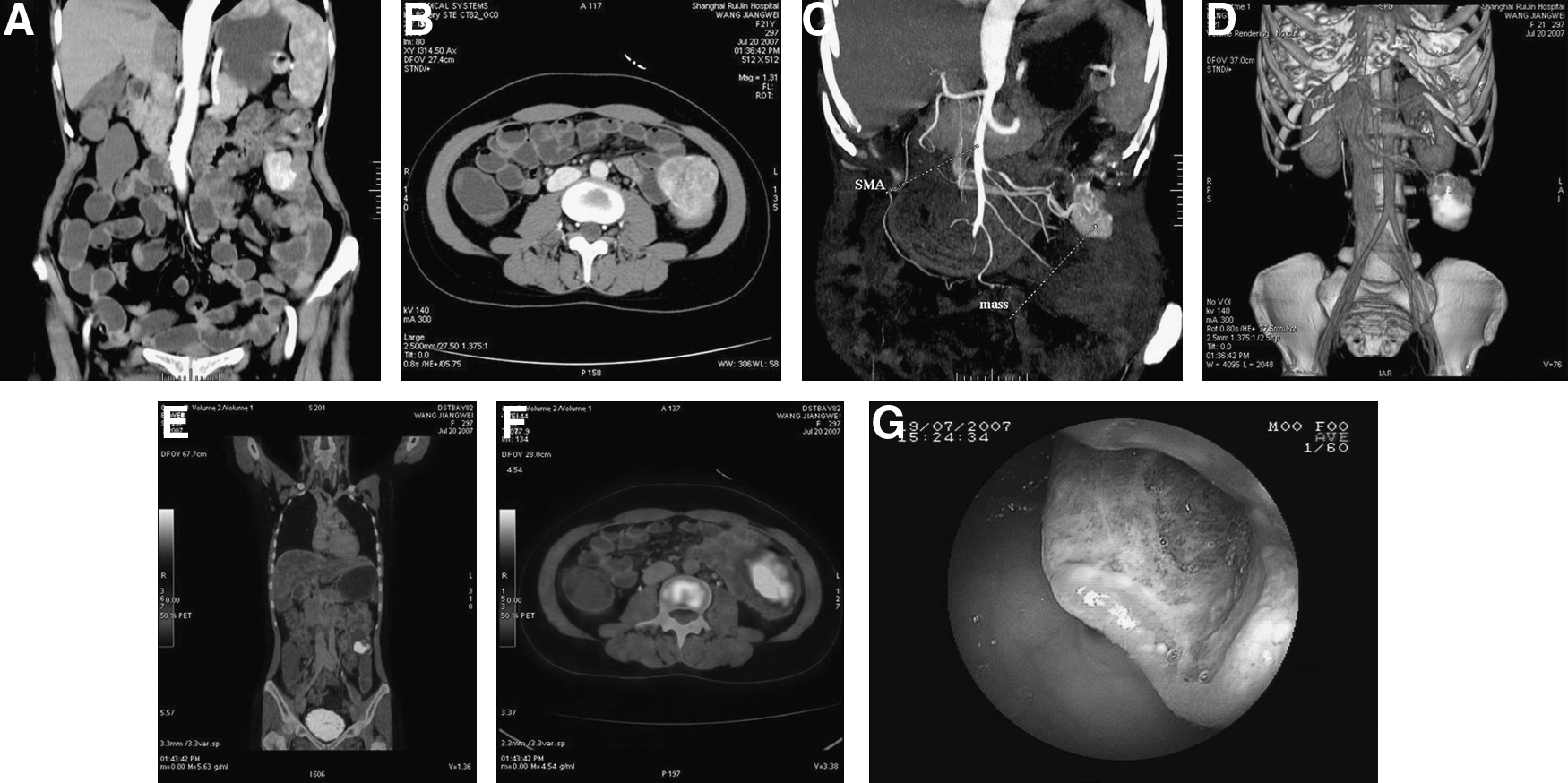
Preoperative diagnosis. (
All operations were performed under general anesthesia. A reverse Trendelenburg position was needed to create a spontaneous pendent of the abdominal organs. The operator stood on the patient's left and the assistant on the opposite. A carbon-dioxide pneumoperitoneum was established through the umbilicus with a Veress needle, and intraperitoneal pressure was maintained at 15 mm Hg. There were three trocars, including one 10-mm and two 5-mm trocars. Their positions were located at the umbilicus (10 mm, laparoscope), the midpoint from the xiphoid to the umbilicus, and the midclavicular line in the left-upper quadrant, respectively. An intestinal exploration began from the Treitz ligament to the ileocecal junction after an abdominal inspection, such as the liver, stomach, omentum, colon, pelvis, etc. The lesion was located by observing intestinal appearance, color, enterocinesia, and the mesentery. The dissection of the small intestine with the lesion was performed laparoscopically after the lesion was exactly located. Subsequently, a wedge resection, segmental resection, or right hemicolectomy was performed, according to the size, location, and nature of the lesion. Generally, the extraction of the lesion was performed through a mini-incision with a plastic protector for the abdominal incision. The small intestine was put back into the abdomen after an extra-abdominal anastomosis. The pneumoperitoneum was reestablished to inspect the anastomosis. If everything was normal, the operation was finished after the closure of the incision (Fig. 2).
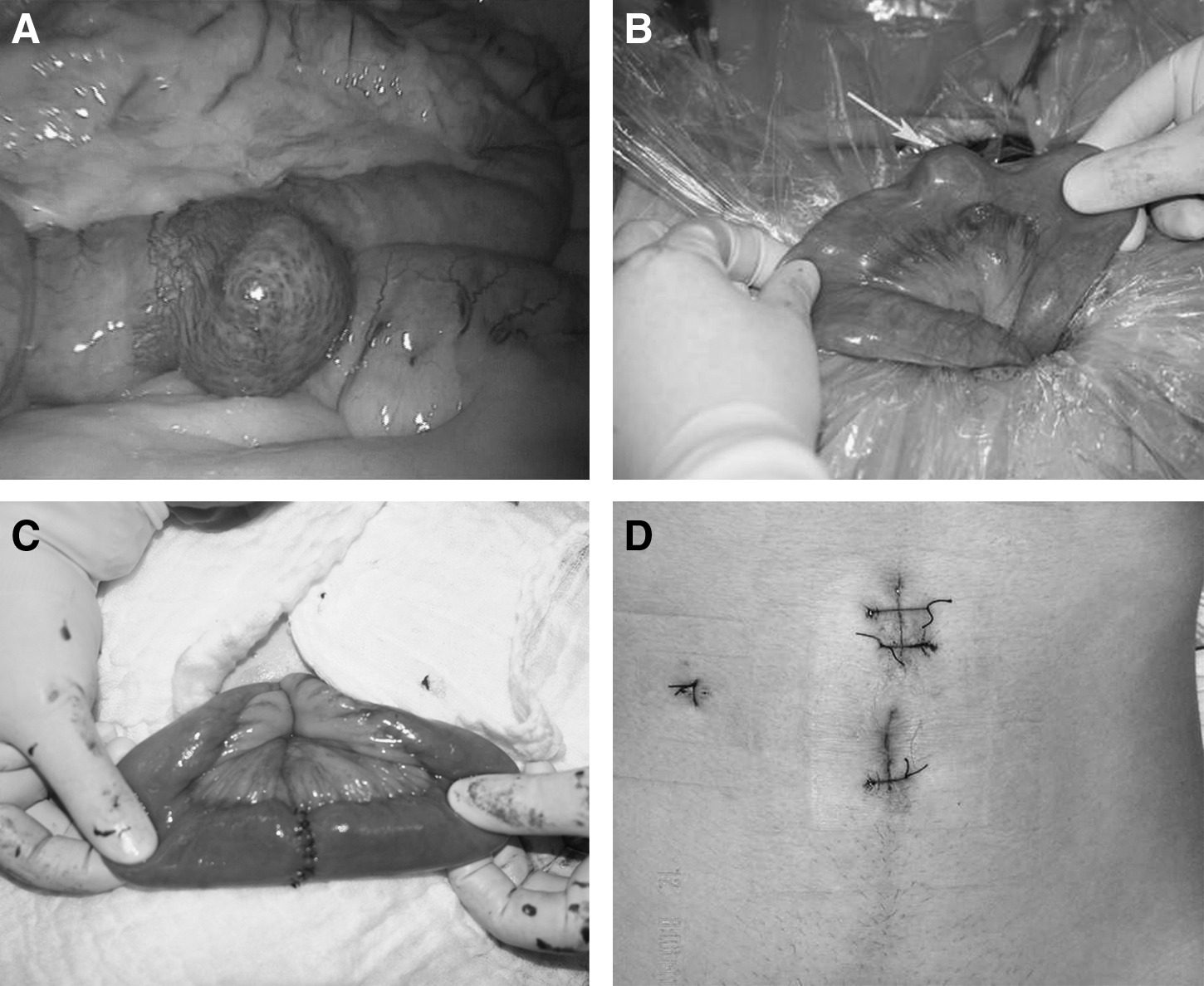
Intraoperative findings. (
Results
All cases were performed laparoscopically. No conversion or intraoperative complication occurred. There were 17 cases in the ileum, 45 cases in the jejunum, and 15 cases in the boundary of the ileum and jejunum, respectively. There were 17 cases performed by laparoscopic wedge resection, 59 by laparoscopy-assisted segmental resection, and 1 by laparoscopy-assisted right hemicolectomy. The operative and recovery data are listed in Table 1.
There were 4 postoperative complications, including 2 cases of adhesive ileus, 1 gastric retention, and 1 anastomotic bleeding. They were cured by nonoperative management. Pathologic results were as follows: gastrointestinal stromal tumors (GISTs; 48 cases), adenocarcinoma (2 cases), diverticulum (14 cases), xanthoma (1 case), hamartoma (1 case), polyp (4 cases), neuroendocrine carcinoma (1 case) tubulovillous adenoma (1 case), leiomyosarcoma (1 case), and vascular malformation (4 cases) (Fig. 3). The mean diameter of tumors was 3.5 ± 1.8 cm.
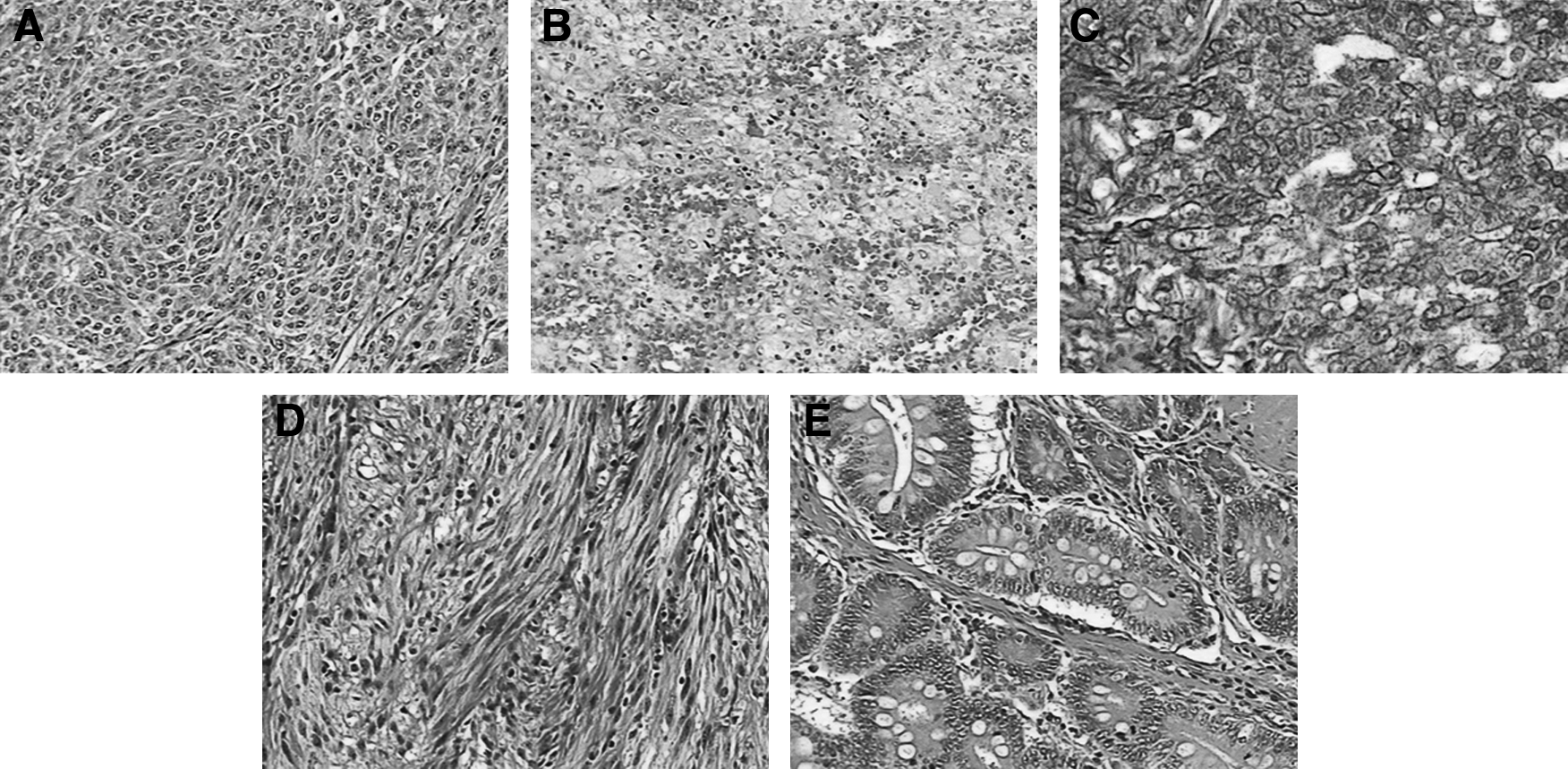
Pathologic results by H&E staining (original magnification, × 400). (
Follow-up time varied from 2 to 70 months, with a median of 36. No trocar site or wound recurrences were noted. There was 1 patient with GISTs found with hepatic metastasis by CT scan at the 26th month, and another patient with GISTs (the 7th month) died from hepatic metastasis. The tumor diameters were, respectively, 5 and 7 cm and could be classified as median- and high-risk degree. One patient with leiomyosarcoma (the 19th month) and 2 patients with adenocarcinoma (the 14th and 15th months) died from hepatic and/or pulmonary metastasis.
Discussion
Due to the lack of specific clinical manifestations and the limitations of the present diagnostic approaches, early diagnosis of small intestinal bleeding is difficult. First, endoscopy should be first performed to exclude possible lesions in the stomach, colon, and rectum. Subsequently, small intestinal bleeding would be taken into account. The small intestine his 3–5 m in length, and its position in the abdominal cavity is overlapping and various. Therefore, it is a great challenge for surgeons, in clinical practice, to make a diagnosis of small intestinal bleeding and to locate the lesion accurately.1–4
Causes of small intestinal bleeding include diverticulum, neoplasm, vascular malformation, etc. In China, neoplasm is the most frequent cause of small intestinal bleeding, and Meckel's diverticulum and vascular malformation are the second and third ones. 5 In our series, the neoplasm accounted for 59 of 77 cases. Present diagnostic approaches of small intestinal bleeding include radiologic examinations (i.e., abdominal CT scan, MSCTE, DSA, and PET/CT), endoscopic examinations (i.e., DBE, capsule endoscopy), and surgical exploration. DBE is the most effective method for the diagnosis of small intestinal bleeding, and its diagnostic rate could reach 75–80%.6,7 In our series, the diagnostic rate of DBE was 92.4% (61/65 cases). In another 4 cases, there were 3 cases diagnosed by other approaches, such as CT scan, MSCTE, PET/CT, etc. Application of DBE is restricted to the longer operative time, lower extent of patient's tolerance, and higher expenses. Meanwhile, it is possible that DBE fails to inspect the whole small intestine both by the oral and anal route. It is also difficult to find the lesions that are small and growing outward. At that time, it must be diagnosed by means of exploratory laparotomy. Laparoscopic exploration has more advantages than open laparotomy, such as smaller incision, more complete exploration, and quicker recovery. Laparoscopic exploration can clearly, directly, conveniently, and thoroughly be used to inspect the whole intestinal serosa and mesentery.4,8–11 In our series, 1 case received laparoscopic exploration without preoperative positive findings. This case turned out to be a jejunal GIST (1.5 cm in diameter), opposite to the mesentery. Meanwhile, to avoid the omission of multiple synchronous lesions, it was necessary to explore the entire small intestine. We explored the small intestine with atraumatic forceps, inch by inch, from the Treitz ligament to the ileocecal junction, and located the lesion by directly observing the intestinal appearance, color, and enterocinesia. Therefore, laparoscopic exploration could be an assistant to the diagnosis of obscure gastrointestinal bleeding and compensate for the blind spot of DBE to improve the diagnostic rate of small intestinal bleeding.
In our 77 cases, there were 4 cases of vascular malformation, 14 of diverticulum, and 59 cases of neoplasm. Commonly, vascular malformation could not be located until congestion in the enteric cavity was found. It is a challenge for surgeons to distinguish it from normal tissue if the lesion of vascular malformation is small and less bleeding. Fortunately, the major cause of small intestinal bleeding is not vascular malformation in China. For small benign intestinal diseases, indications of the laparoscopic operation are the same as the open operation. As for malignant diseases, it is still under controversy. Now, there are increasing reports on laparoscopic operations in colorectal cancers that conclude laparoscopic operations are similar to open operations in the principle of radical resection.12–14 Therefore, laparoscopic operations in small intestinal tumors should strictly follow radical rules. However, abdominal spread could occur as the tumor ruptures when it is being scratched. If the tumor is too large to get out through a small incision, advantages of the minimal incision will lose. Hence, tumors smaller than 5 cm are considered to be indicated by laparoscopy. 15 Of course, tumors bigger than 5 cm also could be resected by laparoscopy.16,17 In our series, there were 9 cases where tumors were bigger than 5 cm, and the biggest one was 7 cm. The rupture of tumors did not occur during the operations. A laparoscopy-assisted operation, instead of a total laparoscopic operation, could be performed on tumors larger than 5 cm. Exploration and location were achieved by laparoscopy, while resection and anastomosis out of the abdominal cavity was through a small incision. Thus tumor could be completely removed by minimally invasive surgery.
Different approaches to the laparoscopic operation were performed, according to the size and nature of the lesions. Laparoscopic wedge resection was performed when the size of the benign tumor is smaller than 1 cm. Laparoscopy-assisted segmental resection of the small intestine was performed as though for the bigger or malignant lesions. Right hemicolectomy should be performed when the malignant tumor is located in the terminal ileum. After the tumor was accurately located, the tumor-related small intestine was dissected under laparoscopy and then pulled out through a small incision, with a plastic protector for the abdominal incision. The small intestinal was put back into the abdomen after an extra-abdominal anastomosis. This can save on operative time and expense without sacrificing the incision appearance. Therefore, it seems advantageous to make more widespread laparoscopic applications in small intestinal disease.
Conclusions
In conclusion, laparoscopy has minimal invasive therapeutic advantages and could improve the diagnostic rate in small intestinal bleeding. We believe that laparoscopy has a promising prospect in the diagnosis and treatment of small intestinal bleeding9,14,16 and should become a routine management of small intestinal bleeding.
Footnotes
Disclosure Statement
No competing financial interests exist.