
Abstract
Abstract
Sclerosing encapsulating peritonitis (SEP) is a rare cause of intestinal obstruction. It is difficult to make a definite preoperative diagnosis, and most cases are diagnosed at the time of laparotomy. It is usually of unknown origin, although, at times, it may be seen secondary to a variety of conditions. Spillage of bile and gallstones at laparoscopic cholecystectomy is an unusual cause of SEP and has not been reported in literature, to date. Contrast-enhanced computed tomography of the abdomen revealed small-bowel loops congregated to the center of the abdomen encased by a soft-tissue density mantle with loculated fluid in the interloop bowel location. Excision of the sac and adhesiolysis was done in our patient for recurrent episodes of intestinal obstruction, who recovered well in the postoperative period.
Introduction
Case Report
A 64-year-male presented with crampy abdominal pain that started in the periumbilical region and was nonradiating, aggravated by food intake, associated with bilious vomiting, and constipation. The patient had a history of similar episodes twice in the last 8 months and was managed conservatively. The patient had a history of laparoscopic cholecystectomy with spillage of bile and gallstones during the procedure 1 year earlier. There were no intra-abdominal adhesions at the time of laparoscopic cholecystectomy. The patient did not have a history of tuberculosis or any other drug intake, except tablets of glimepiride (generic) 1 mg daily for diabetes mellitus. On examination, the patient was dehydrated and afebrile, with a pulse rate of 92/minute and blood pressure of 100/70 mm Hg. Scars from a previous laparoscopic cholecystectomy were present. There was mild abdominal distension, no free fluid, bowel sounds were sluggish, and rectal examination was normal. Laboratory blood analyses were within normal limits. Plain abdominal X-ray showed few dilated small-bowel loops. An ultrasonography of the abdomen revealed an 11 × 6 cm fluid collection in the left iliac fossa with multiple septations. A contrast-enhanced computed tomography (CECT) scan revealed that the jejunal and ileal loops were clumped together in a thick, membrane-like sac, which was adherent anteriorly to the parietal peritoneum with evidence of loculated fluid in the interloop locations (Fig. 1). The CECT scan also showed an 11-mm hypodense lesion in the left iliac fossa that was suggestive of spilled gallstone (Fig. 1). An exploratory laparotomy was performed, as symptoms did not resolve with conservative treatment. On laparotomy, small bowel, large bowel, and omentum were encased in a fibrous sac (Fig. 2); on opening of this sac, the small bowel and left colon were encased in two different sacs, with dense interloop adhesions and loculated collection inside the sacs (Fig. 3). One 1.3 × 1 cm gallstone was recovered from the peritoneal cavity. The omentum was normal, and there was no malrotation of the gut. An excision of the sac and adhesiolysis was done without any bowel resection (Fig. 4). Sac fluid was negative for malignant cytology and acid fast bacilli (AFB). Histopathology of the peritoneal sac showed fibrocollagenous tissue with mixed inflammatory infiltrates, occasional well-formed granulomas with giant cells, and few dense areas of hyalization, but there was no evidence of malignancy, caseating epithelial cell granuloma, or AFB. The patient recovered well during the postoperative period and was discharged on day 10; he is doing well in the follow-up.

CECT scan of the lower abdomen shows clustered gas-containing small-bowel loops with thick, membrane-like sac (white arrows), fluid inside the sac (notched arrow), and spilled gallstone in the left iliac fossa (black arrow).

Intraoperative photograph showing abdominal cocoon (black arrow).
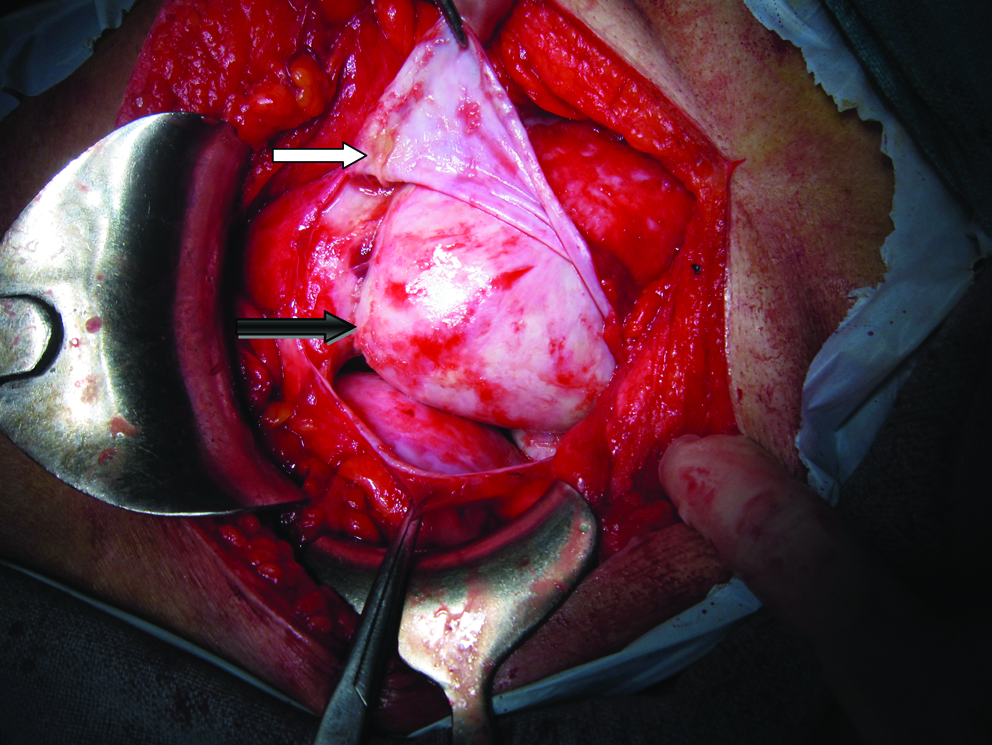
Intraoperative photograph showing layers of sac forming a cocoon, the outer layer of the sac (white arrow), and the internal layer (black arrow).

Intraoperative photograph showing bowel loops after excision of the sac and adhesiolysis.
Discussion
SEP is a rare cause of intestinal obstruction, which is characterized by the encasement of the small bowel by a fibrocollagenic cocoon-like sac.1,5 It can be idiopathic, which is called abdominal cocoon, or secondary to chronic ambulatory peritoneal dialysis, treatment with practolol, tuberculosis, or other rare causes, such as peritoneovenous shunt, ventriculoperitoneal shunts, and orthoptic liver transplantation.2,3,4,6 None among the above-mentioned causes was present in our case, but there was the spillage of bile and gallstones during the laparoscopic cholecystectomy, and there were no intra-abdominal adhesions at the time of surgery 1 year previously. So, bile and gallstone spillage during a laparoscopic cholecystectomy may also be added to the list of causes of SEP. Bile and gallstones, being irritants, may lead to an inflammatory reaction, which causes fibrosis, adhesions, and sac formation. It is strongly recommended to take all the preventive steps to avoid bile and gallstone spillage during a laparoscopic cholecystectomy to avoid this problem. It is difficult to establish a definite preoperative diagnosis, and most cases are diagnosed incidentally at laparotomy. A better awareness of this entity and the modern imaging techniques may facilitate the diagnosis preoperatively. 7 No surgical treatment is required in asymptomatic SEP patients. 8 There is a consensus among most researchers that symptomatic patients require surgical treatment. At surgery, in addition to careful dissection and excision of the covering membrane, dense interbowel adhesions also need to be freed for complete recovery. 9 In order to avoid complications of postoperative intestinal leakage and short-bowel syndrome, resection of the bowel is indicated, only if it is nonviable.
Conclusions
In conclusion, spillage of bile and gallstone during a laparoscopic cholecystectomy may be added to the causative list of SEP, and it is imperative for laparoscopic surgeons to be very careful to avoid gallblaber perforation and spillage during a laparoscopic cholecystectomy to avoid these serious consequences.
Footnotes
Disclosure Statement
No competing financial interests exist.