
Abstract
Abstract
When a patient with a ventriculoperitoneal shunt (VPS) undergoes laparoscopic surgery, there is the concern about possible problems with the shunt due to increased intra-abdominal pressure. We conducted a simplified reflux experiment on VPS valves to demonstrate safety. Each of five different VPS valves was connected via tubes to a glass vessel of our own making. Carbon-dioxide gas was consecutively insufflated into the vessel at 3–25 mm Hg pressure to determine whether reflux occurred when the valves and tubes were empty (opened test) and when filled with physiologic saline (closed test). Reflux occurred for two of five valves at an insufflation pressure of 5 mm Hg or more in the opened test, while not for any valves until 25 mm Hg in the closed test. In clinical settings, there would be no possibility of reflux under the pneumoperitoneum in VPS systems draining cerebrospinal fluid. Laparoscopic surgery in patients with VPS would be performed safely if characteristics of VPS valves are taken advantage of.
Introduction
Materials and Methods
The following five different programmable valves were used at the maximum setting.
Polaris® adjustable valve (product code SPV; Sophysa, Orsay cedex, France) BioGlide® Strata II® valve (product code 92866; Medtronic, Mineapolis, MN) BioGlide® Strata® NSTTM valve (product code 92365; Medtronic) Codman® HakimTM programmable valve (product code 82-3100; Codman & Shurtleff, Raynham, MA) Codman® HakimTM programmable valve (product code 82-3101; Codman & Shurtleff)
The shunt tubes to which each valve was connected were inserted into diluted indigo carmine solution in a sealed glass vessel of our own making (Fig. 1). CO2 gas was insufflated into the vessel, using pneumoperitoneal equipment (Omniflator 7640; Nortech, Elgin, IL), to increase the internal pressure. The set pressure in the vessel was increased consecutively to 3, 5, 7, 10, 15, 20, and 25 mm Hg at 30-second intervals to determine whether there was the reflux of diluted indigo carmine solution in the tubes at each set pressure (opened test). The shunt valves and tubes were then filled with saline solution, the vessel was refilled with oil, and the shunt tubes were inserted into oil in the vessel. As well as the opened test, the occurrence of reflux of oil in the vessel was investigated by increasing the internal pressure of the vessel (closed test).
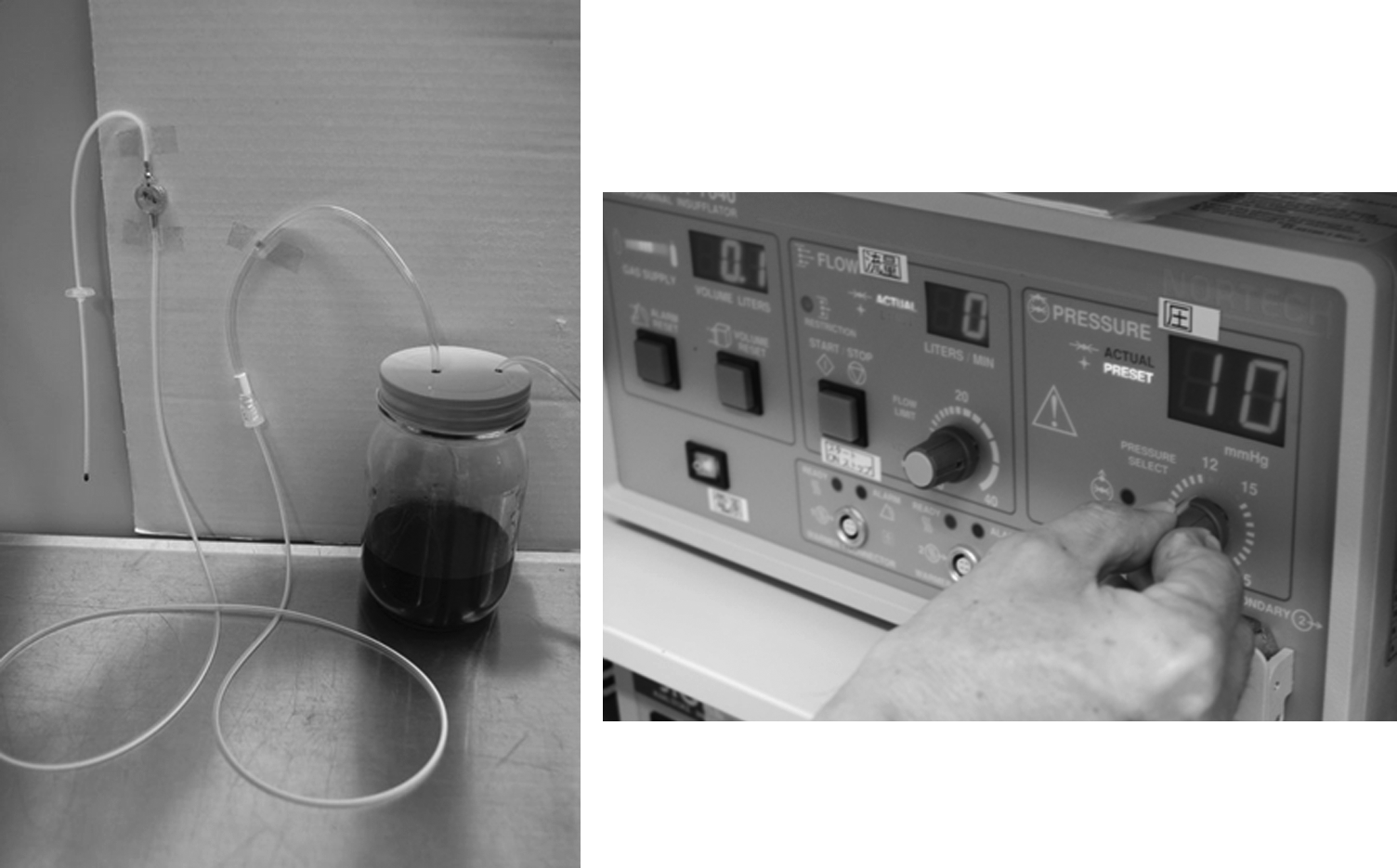
Simplified reflux experiment on VPS valves. Carbon-dioxide gas was insufflated into a glass vessel of our own making, in which tubes connected to shunt valves were placed.
Results
In the opened test, there was no reflux up to an insufflation pressure of 10 mm Hg for the Polaris adjustable valve (product code SPV), the BioGlide Strata II valve (product code 92866), and the BioGlide Strata NST valve (product code 92365), but there was reflux of about 2 cm, with to-and-fro motion of the interface in the tubes, at an insufflation pressure of 15 mm Hg or more, followed by no further reflux. For the Codman Hakim programmable valve (product codes 82-3100 and 82-3101), reflux occurred in the tube during insufflation at an insufflation pressure of 5 mm Hg or more. Reflux stopped once the set pressure was attained, and this process was repeated. In the closed test, there was no reflux for any of the shunt valves at any of the set pressures (Table 1).
VPS, ventriculoperitoneal shunt; − , no reflux; + , go on refluxing to set pressure; *, reflux and stop at once.
Discussions
Laparoscopic surgery in patients with VPS tubes was previously contraindicated because of the possibility of a rapid increase in the intracranial pressure due to the pneumoperitoneum. Uzzo et al. 1 reported that intracranial pressure increased to a maximum of 25 mm Hg at a pneumoperitoneal pressure of 12 mm Hg. Most recent VPS systems use programmable valves. The valve is designed to prevent the refluxing of intra-abdominal or cerebrospinal fluids. Neale et al. 2 reported that there was no reflux for pressure increases to a maximum of 350 mm Hg in an in vitro experiment (PS Medical Flow-Control valve, Burr Hole). In reality, however, there are no basic data that show the effect of the pneumoperitoneum with CO2 on current VPS tube systems. Variable pressure, due to surgical maneuvers, is applied to the tubes in the abdomen. We, therefore, conducted a simplified reflux experiment by using pneumoperitoneal equipment clinically used for surgery to assure the safety of VPS systems.
There was no reflux for any of our tested shunt valves when filled with saline. This fact suggests that actually functioning shunt systems induce no reflux under laparoscopic surgery because cerebrospinal fluid is flowing. It is unlikely that a pneumocephalus will be produced by CO2 insufflation at pressures of less than 10 mm Hg during laparoscopic surgery. On the other hand, this experiment demonstrated that there could be reflux under normal pneumoperitoneal pressure, if the shunt system is empty. Because reflux-preventing valves of traditional VPS systems are weak, it is necessary to pay close attention to the possibility of reduced reflux-preventing function.
To the best of our knowledge, only two reports have described shunt-system troubles among reports of laparoscopic surgery in patients with VPS tubes3–12 (Table 2). One report involved the pneumoperitoneum in a patient in whom a VPS system had just been placed, resulting in intraoperative ventilatory impairment secondary to subcutaneous emphysema. 3 The other report described a shunt closure 5 days after placement of a VPS. 6 During the early days after the placement of a VPS system, it is necessary to conduct laparoscopic surgery carefully.
VPS, ventriculoperitoneal shunt; OP, operation; PP, pneumoperitoneum pressure; LPS, lumboperitoneal shunt; NA, not available.
Laparoscopic cholecystectomy was performed for a patient with VP shunt. Based on the result of the present reflux experiment, the pneumoperitoneal pressure was set at 8 mm Hg with tube clamping during operation. Although the necessity of shunt clamping was not apparent, shunt troubles might not always occur, even if laparoscopic surgery is performed without shunt clamping or manipulation, because of the function of reflux-preventing valves. It is also useful to decrease the set pressure of the pneumoperitoneum and desufflate intermittently to adjust the intra-abdominal pressure.
Conclusions
We conducted a simplified reflux experiment of CO2 gas on VPS valves to demonstrate safety. If detailed information about VPS systems is obtained and characteristics of its valves are taken advantage of, laparoscopic surgery can be performed safely.
Footnotes
Disclosure Statement
No competing financial interests exist.