
Abstract
Abstract
Background:
Laproscopic surgery is widely used in treating gastrointestinal disease. This study investigated the clinical result, short-term outcomes, and cost analysis of the newly developed gasless laparoscopy-assisted distal gastrectomy (GLADG) and compared it with conventional open distal gastrectomy (ODG).
Methods:
Seventy-five patients underwent distal gastrectomy with radical lymph node dissection for early gastric cancer from December 2005 to January 2008. Thirty-one patients underwent GLADG and 44 underwent ODG. Postoperative pain, morphine use, disease-free and overall survival, and surgical and hospital costs were measured postoperatively and compared between the two groups.
Results:
Patients in the two groups were comparable by age, sex, body mass index, tumor size, tumor location, cancer staging, and operative time. The GLADG group had early start of oral intake and shorter postoperative hospital stay (P < .05). There was less morphine use from postoperative day 1 to 4 in the GLADG group than in the ODG group (P < .05), and body temperature from postoperative day 1 to 2 was lower in the GLADG than in the ODG group (P < .05). Cost analysis showed that operation cost (100,242 ± 5385 versus 36,455 ± 1419) and equipment cost (65,909 ± 5385 versus 2122 ± 1419) was higher in the GLADG group, but its total hospital cost (193,552 ± 12,715 versus 206,676 ± 41,920) was lower than in the ODG group (P < .05). The 2-year disease-free and overall survival rates were not different between the two groups.
Conclusions:
GLADG is feasible for early gastric cancer. It is advantageous because of less pain, less postoperative inflammatory response, less blood loss, and shorter total hospital stay while achieving the same oncologic results as ODG.
Introduction
However, gas-filling laparoscopy requires inflation of the abdominal cavity to provide space for visualizing the operative site. Positive abdominal pressure increases cardiac preload and after load, systemic vascular resistance, and cardiac index.7,8 D2 lymph node dissection is also difficult under laparoscopy and, as such, requires a longer period of learning time.9,20 Tactile sensation and manipulation are restricted in laparoscopic gastrectomy, thereby significantly prolonging operative time. Port-site recurrence due to pneumoperitonium after laparoscopic gastrectomy has also been reported recently.10,35,36
Our institute has recently developed a novel technique of gasless laparoscopic surgery with abdominal wall lifting, which combines the benefits of open procedure and laparoscopic surgery. This technique is now being used in gastrectomy, hepatectomy, and splenectomy in the hospital. The perioperative results of gasless laparoscopy-assisted distal gastrectomy (GLADG) for early gastric cancer have been reported with favorable outcomes. 11 This study investigated the postoperative outcomes of GLADG for early gastric cancer and compared it with traditional open distal gastrectomy (ODG).
Methods
Patients
From February 2006 to December 2007, 75 consecutive patients in the National Taiwan University Hospital with a preoperative diagnosis of early gastric cancer located in the middle and lower third of the stomach were enrolled in this study. The inclusion criteria were T1N0 and T1N1 early gastric cancer that was preoperatively diagnosed by endoscopy and computed tomography. All of the patients had abdominal computed tomography for cancer staging and none showed any evidence of para-aortic and level 2 lymph nodes lymphadenopathy or distant metastasis.
Thirty-one patients underwent GLADG and another 44 underwent ODG. According to the gastric cancer treatment guidelines in Japan, all of the patients received lymph node dissection with Groups 1, 3, 4d, 4sb, 5, 6, 7, 8a, 9, and 12a. 12
The patients' age, sex, and body mass index and American Society of Anesthesiology score were documented. Peri- and postoperative characteristics were obtained from the medical charts, including operating time, blood loss, number of lymph nodes dissected, peak body temperature, heart rate, day of first flatus, day of first eating, dosage of morphine use, postoperative pain using a visual analog scale, and postoperative hospital stay.
Cost analysis (surgical cost and hospital cost) were also analyzed and estimated, as well as disease recurrence, patient death, disease-free survival, and postoperative patient survival.
Surgical procedure: gasless laparoscopic subtotal gastrectomy
A single surgeon with extensive experience in upper gastrointestinal surgery performed all the operations, with the patients under general anesthesia in supine position. The operator stood on the right side of the patient while the assistant stood on the left side. Kent's clamp and a clamp bar were positioned so that the clamp bars stood at the level of the patient's nose. A minilaparotomy was made (5 cm, called a three-finger port) in the upper midline of the abdomen about 5 cm below the xyphoid process. A wound protector was placed over the minilaparotomy to avoid contamination or cancer cell implantation (Fig. 1). Specially designed retaining retractors elevated the abdominal wall while the tumor and clip location were palpated using one or two fingers through the minilaparotomy to ensure their position (Fig. 2).
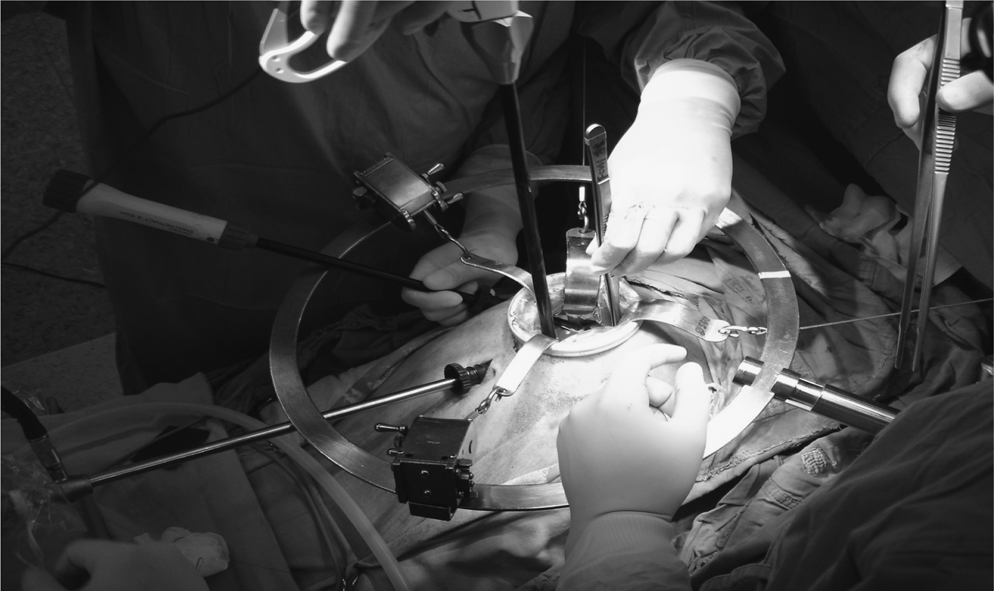
The minilaparotomy wound and the self-designed abdominal lifting system.
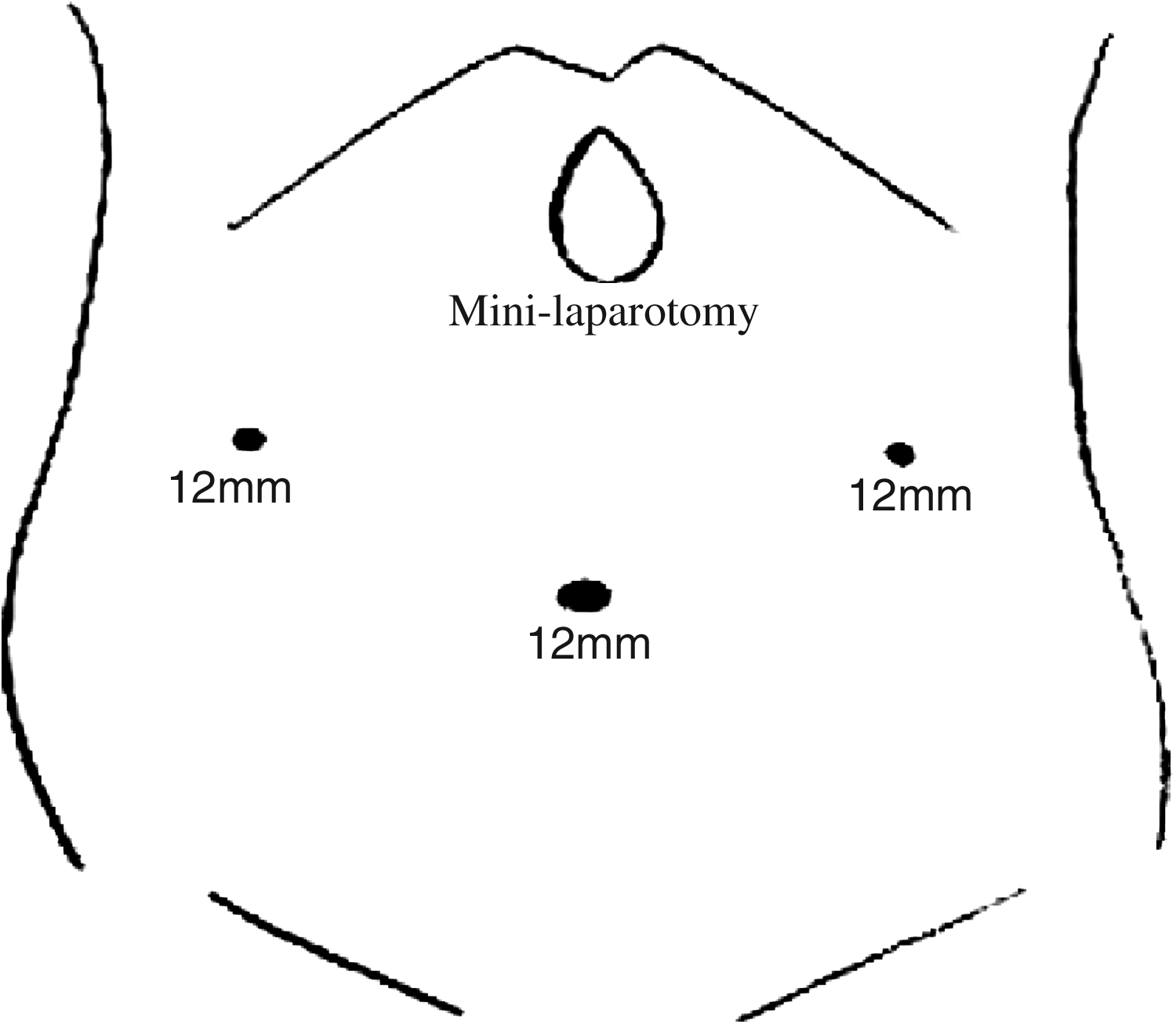
The incision and port sites used in gasless laparoscopic gastrectomy.
Three or four working ports were created at the bilateral subcostal region or periumbilicus, depending on the tumor location. The laparoscope was inserted either through the minilaparotomy or through any of the ports for examination of the entire peritoneal cavity, especially the Douglas pouch. A Harmonic scalpel (Ethicon, Cincinnati, OH), Ligasure (Tyco; Valleylab, Boulder, CO), or electrocauterizer divided the greater omentum through either the working ports or minilaparotomy. The left gastroepiploic vessels were exposed and divided by ligature, whereas the right gastroepiploic vessels were divided at their roots. After the right gastric artery was exposed and divided at its origin by ligature, the duodenum was transected 1 cm below the pylorus by endoscopic stapler (Endo GIA, Tyco; Valleylab). Groups 7, 8a, and 9 lymph nodes were then dissected and the left gastric artery was exposed and divided by suture ligation.
The specimen was removed through the minilaparotomy after transection from the remaining stomach by an endoscopic stapler inserted through either the minilaparotomy or ports. Dissection of lymph nodes located in the perigastric area and the celiac trunk, common hepatic artery, left gastric artery, and hepatoduodenal ligament was done mainly via the minilaparotomy by direct vision or via the working port by camera vision. Direct control of the bleeding was easily made through the minilaparotomy, and vigorous suction was accomplished through the ports or minilaparotomy.
B-II gastrojejunostomy was performed by intracorporeal anastomosis using an endoscopic stapler. The laparoscopic instruments were inserted more freely into the peritoneal cavity for anastomosis, depending on the level of the remnant stomach. The anastomosis was reinforced by hand suture by traditional instruments by either direct visualization or intracorporeal suture with laparoscopic instruments under laparoscopic inspection, or both.
Postoperative care
All patients were administered prophylactic antibiotics for 3 days. The nasogastric tube was removed after flatus, and patients were also given clear liquid diet after removal of the nasogastric tube. All patients were discharged after attaining good tolerance of soft diet.
Operation cost, equipment cost, and hospital cost
All citizens in Taiwan have national health insurance. The Bureau of National Health Insurance pays New Taiwan dollar (NTD) 34,333 (1USD = 32 NTD) for each distal gastrectomy in either open or laparoscopic distal gastrectomy, but not for any laparoscopic equipment in laparoscopic distal gastrectomy. Thus, patients need to pay additional laparoscopic equipment costs by themselves for laparoscopic distal gastrectomy. The operation cost is equal to 34,333 plus equipment cost, and the hospital cost is the total of all costs except operation cost.
Statistical analysis
All values were expressed as the mean ± standard error of mean. Student's t-test was used to compare the two surgical groups, and the overall and disease-free survival was estimated by Kaplan–Meier analysis. Significance of differences between the two groups was calculated by log-rank test. P < .05 was considered statistically significant.
Results
Clinicopathological characteristics of the patients
The 75 patients had a median age of 60.1 years (range: 22–86 years). There were 38 men and 37 women, and all underwent ante-colic gastrojejunostomy. Pathologic examination showed 54 stage IA and 21 stage IB early gastric cancers. All of them were followed up until September 2008, with a mean follow-up time of 19.3 months. The demographic and pathology data showed no differences between the two groups (Table 1).
GLADG, gasless laparoscopy-assisted distal gastrectomy; ODG, open distal gastrectomy; ASA, American Society of Anesthesiology.
Postoperative and surgical outcomes
The operation time in GLADG was 165.8 ± 10.08 minutes, which was not significantly different to the ODG (206.11 ± 7.54 minutes). Mean blood loss was 60 mL in GLADG, which was significantly less than that of ODG (P < .01). There were no differences in lymph node dissection between the two groups. The first oral intake (4.06 ± 0.93 in GLADG versus 6.54 ± 1.04 in ODG) and discharge (10.1 ± 0.5 in GLADG versus 18.2 ± 3.6 in ODG) were all significantly less in the GLADG group (all P < .05).
Two patients in the GLADG group had postoperative complication: one had afferent loop syndrome and the other had ileus. In the ODG group, there were four complications: 2 patients had afferent loop syndrome, both of whom required a second operation, and 2 had intra-abdominal abscess (Table 2). All 4 were discharged uneventfully. The 30-month disease-free survival (0.92 in GLADG versus 0.92 in ODG, P = .76) and all survival (0.93 in GLADG versus 0.88 in ODG, P = .62) were not different between the GLADG and ODG groups (Figs. 3 and 4).
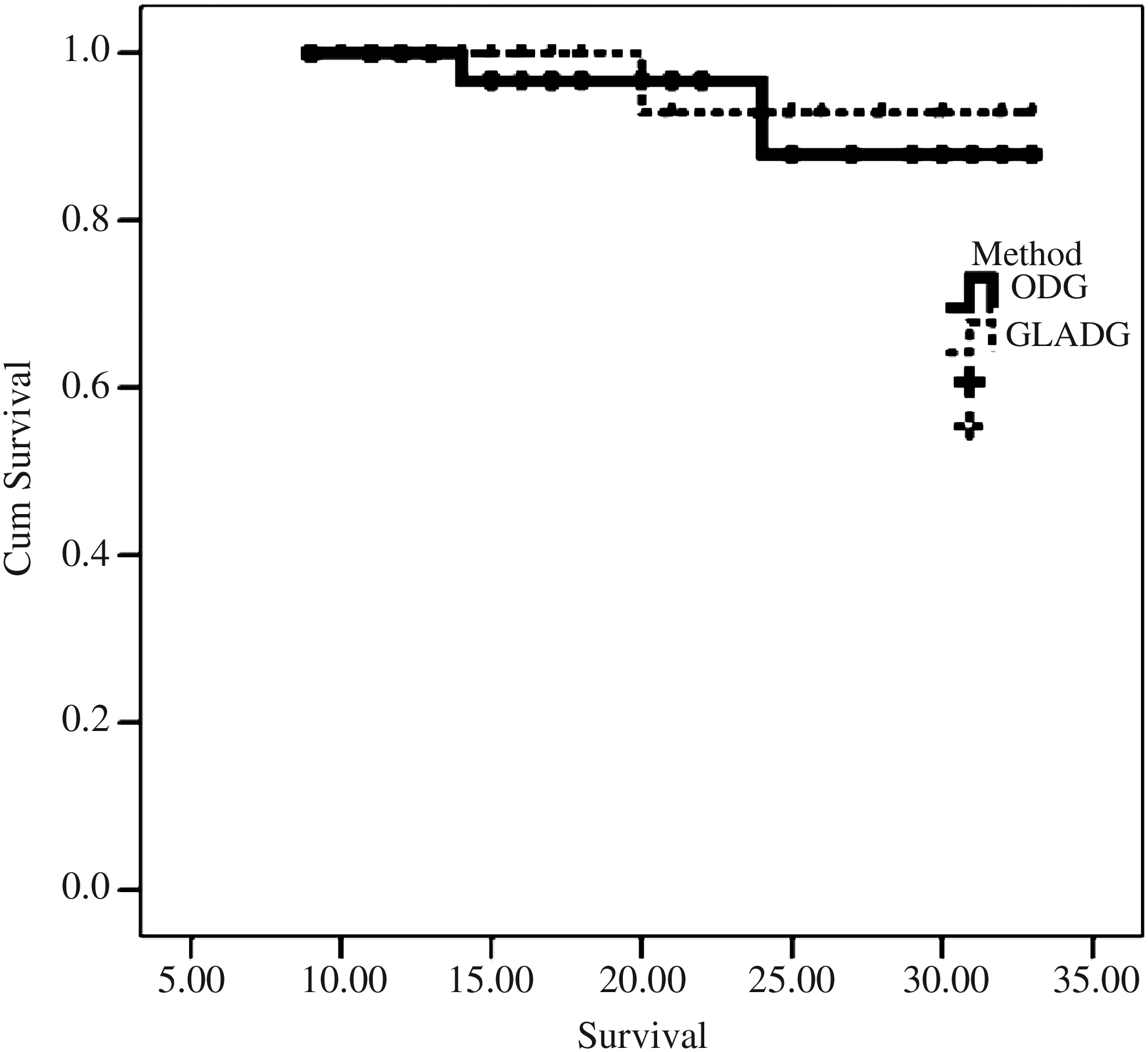
Overall survival between the gasless laparoscopy-assisted distal gastrectomy and ODG groups.

Disease-free survival between the gasless laparoscopy-assisted distal gastrectomy and ODG groups.
NTD, New Taiwan dollar.
The postoperative pain scale was not significantly different in both groups, although the GLADG group had less morphine use from postoperative day 1 to 4. Peak temperature was also less in the GLADG group from postoperative day 1 to 2 (Table 3).
Cost analysis
Cost analysis showed that hospital cost (in NTD) in the GLADG group was less than that in the ODG group (NTD 97,084 ± 10,810 versus 151,968 ± 31,510). Surgical cost (NTD 100,242 ± 5385 versus 36,455 ± 1419) and total hospital cost (NTD 193,552 ± 2715 versus 190,767 ± 31,474) in the GLADG group were higher than those in the ODG group (Table 2).
Discussion
Recently, there have been various kinds of minimal invasive surgery for early gastric cancer. Among these, gas-filling laparoscopic gastrectomy has become the main treatment for early gastric cancer. Most of reports show results of fast recovery, less postoperative pain, and shorter hospital stay despite problems such as long operation time, high operation fee, port-site recurrence, cardiovascular restriction from increased intra-abdominal pressure, and loss of tactile sensation due to pneumoperitonium.13–15 Although GLADG is not a popular treatment for early gastric cancer, it combines the advantages of both traditional open surgery and minimal invasive surgery. For this reason, GLADG can compensate for the shortcomings of gas-filling laparoscopic surgery without losing the advantage of short-term recovery of minimal invasive surgery.16,17
In early gastric cancer, the incidence of lymph node metastasis is 2%–4% in tumor invasion to the mucosa and 18%–20% in tumor invasion to the submucosa. Over 95% of metastatic lymph nodes are restricted to the N1 level, whereas other metastatic lymph nodes are mainly in groups 7, 8, and 9.18,19 For this reason, in the Japanese treatment guidelines for gastric cancer, gastrectomy with D1 and groups 7, 8, 9, 11, and 12a lymph node dissection is sufficient for early gastric cancer treatment. 12
Following the rules of treatment for gastric cancer, this study shows no significant differences in numbers of harvested lymph nodes between the GLADG and ODG groups. Moreover, disease-free survival and overall survival are not significantly different between the two groups. Hence, GLADG is acceptable from the point of view in oncologic therapy.
According to the learning curve study from Kim in 2005, gas-filling laparoscopic gastrectomy is more technically difficult than laparoscopic cholecystectomy and laparoscopic colectomy. The operative time of laparoscopic distal gastrectomy significantly decreases after the first 50 operations. 2 In GLADG, a minilaparotomy wound is used at the beginning of the operation and the surgeon obtains good operating field visualization from either the minilaparotomy or laparoscopy. Further, both traditional and laparoscopic instruments can be used via minilaparotomy to perform ligation, suture, tissue manipulation, and bleeding control as in open operation.
Control of bleeding is very important in laparoscopic surgery as it is the most frequent cause of conversion to open surgery.21,22 Bleeding can be controlled more easily by traditional instruments from the minilaparotomy. The use of vigorous suction can also make the operative field clean without space collapse because of decreased intra-abdominal pressure. All of these enable the performance of GLADG in less time with less blood loss. Because of the characteristics of open surgery, the learning curve is fast, requiring only a few cases for surgeons to become familiar with the operative environment. This device and technique can also provide a bridge for young or less-experienced surgeons to become familiar with advanced laparoscopic surgery from open surgery.
Many studies have evaluated the cost analysis of laparoscopic surgery. The operation cost for laparoscopic surgery is higher than that for conventional surgery because of the use of disposable instruments. Nevertheless, the patients who undergo laparoscopic surgery have shorter hospital stay and faster recovery, whereas postoperative costs are higher in open surgery.23–25 In the study patients, many disposable instruments have been used to divide the gastrointestinal tract and for anastomosis. Thus, the costs of the surgical equipment and the surgery itself are much higher in the GLADG group. The average hospital stay of the ODG group is 8 days more than in the GLADG group. Thus, postoperative hospital cost is much higher in the ODG group. In the patients who undergo gastrectomy, the extra costs of the disposable and stapler instruments is fully compensated by the lower charges for ward use and nursing care associated with the GLADG.
Postoperative morphine use in the GLADG group also responds to this result from postoperative day 1 to 4. Undoubtedly, a small incision wound is one of the major advantages of laparoscopic surgery, which causes less postoperative pain.26–28 Postoperative pulmonary function, such as forced vital capacity and FEV1, are suppressed in the patients with large and long incisions in the upper abdomen after conventional upper gastrointestinal surgery. 13 In addition, bowel manipulation in conventional open surgery is more severe than in laparoscopic surgery, resulting in longer time of recovery of bowel peristalsis after operation.
In a study by Schippers et al., the postoperative first myoelectrical activity in the patients who underwent laparoscopic cholecystectomy was earlier by an average of 40 hours than in the patients who underwent open cholecystectomy. 29 There is a dose-related effect of morphine on the restriction of colonic peristalsis at postoperation day 3, and all doses of morphine inhibit the migrating spike bursts associated with propulsation and defecation. 30 As such, there is a relationship between the length of incision, wound pain, morphine use, and bowel recovery. In the recovering patients who underwent ODG, oral intake and bowel flatus resume at 1 or 2 days later than in the GLADG group, and the total hospital stay is 8 days more than in the GLADG group.
Pulmonary atelectasis is more prominent in open surgery and it makes the difference in postoperation body temperature.37,38 Moreover, laparoscopic surgery uses small incisions and less manipulation, but the effects of systemic stress response as well as the response of stress hormones and cytokine concentrations in serum after laparoscopic surgery remain controversial.31,32 This study has investigated and analyzed the body temperature of patients at postoperation days 1–5 and it shows that body temperature is significantly lower in the GLADG group. Although serum concentrations of stress hormones, such as interleukin 6, insulin, and CRP, have not been checked after the operation, inflammation seems slightly lower in the patients who have undergone GLADG.
There were 6 patients with operation-induced complications, but there were no significant differences in complications between the two groups. All patients who have undergone distal gastrectomy have reconstruction with Billorth-II gastrojejunostomy and the occurrence of afferent loop syndrome is higher than in other series. Both Billorth-II gastrojejunostomy and Roux-en-Y reconstruction can induce afferent loop syndrome, but which reconstruction has higher incidence of complications remains unclear. 33 Nonetheless, Roux-en-Y reconstruction in the patients who undergo distal gastrectomy can decrease gastroesophageal reflux and bile reflux. 34 For this reason, more Roux-en-Y reconstruction are performed.
Conclusions
In this short-term study, the patients who undergo GLADG have less pain, less analgesics use, rapid recovery of gastrointestinal function, and shorter hospital stay while achieving the same oncologic treatment results as the conventional open surgery. It is a feasible procedure for the patients with early gastric cancer. Because the mean postoperative follow-up is <2 years, more investigations on the long-term results after GLADG are warranted.
Disclosure Statement
No competing financial interests exist.