
Abstract
Abstract
LigaSure™ is a new bipolar vascular sealing system commonly used in various fields of surgery. However, no reports have been published about its use in plastic surgery, particularly for endoscopic flap harvesting. In this study, we present the use of LigaSure in endoscope-assisted latissimus dorsi (LD) flap harvesting for breast reconstruction. Between 2006 and 2008, 11 female patients with the mean age of 33.4 (range, 20–49 years) who had previously undergone mastectomy operations were included in the study. First stage of reconstruction was performed with the ipsilateral LD harvested by the help of LigaSure and a tissue expander placed beneath the LD and pectoralis major muscles. Secondary reconstruction was done by a definitive silicon gel–filled implant placed after an average of 6.6 months of expansion (range, 6–9 months). Data concerning the hospitalization and operation times, drainage amounts, complications, etc., were recorded. Mean follow-up was 13 months (range, 8–18 months). Mean flap harvesting time was recorded as 74.2 minutes (range, 50–125 minutes), which shortened as the surgeon got used to the procedure. Patients were hospitalized for 3–7 days, with a mean hospitalization period of 5.5 days. The total mean drainage amount postoperatively was found to be 950 mL (range, 725–975 mL), which is relatively lower than the previously reported values. LigaSure use in endoscope-assisted LD harvesting is easy, safe, and time sparing with almost no complications observed in this small initial series. Although more controlled studies with larger number of patients need to be done to verify its effectiveness in terms of hospitalization, drainage amounts, etc., it holds promise for a wide spectrum of operations in the field of plastic surgery.
Introduction
Although one of these pedicled flaps, the LD flap, is commonly used in breast reconstruction, this procedure has several disadvantages. One drawback is the relatively poor aesthetic and functional outcome of the donor site.1,2 In a study, 22% of patients rated their donor site scar unacceptable. 3 Endoscopy-assisted LD harvesting, which has been developed to overcome this problem, is the surgery of choice for many reconstructive surgeons.4–7
Electrothermal bipolar vessel sealer (EBVS; LigaSure; Vessel Sealing System) has been used in various surgical specialties, including general surgery, urology, obstetrics, and gynecology. Many studies have demonstrated the general safety and effectiveness of this hemostasis device.8,9 However, no reports have been published about the use of EBVS in plastic surgery, particularly for endoscopic flap harvesting.
In this study, we present our early experience with the EBVS system in reconstructive plastic surgery. We demonstrate the effectiveness of this new surgical tool in 11 breast cancer patients who, following mastectomy, had their breasts reconstructed using an endoscope-assisted LD flap with an expandable prosthesis.
Patients and Methods
Patient characteristics
Eleven female patients with a mean age of 37.9 years (range, 20–49 years) were enrolled in this study in the time period between 2006 and 2008. All patients had previously undergone surgery for breast carcinoma at ∼28 months (range, 23–36 months) prior to reconstruction. Only 2 had immediate reconstructions, whereas the others had a delayed procedure. One patient underwent a bilateral reconstruction following a bilateral mastectomy at different times. Primary reconstruction was performed using an ipsilateral LD flap with an integrated-valve breast expander (Mentor) placed beneath the pectoralis major (PM) and LD muscles. This initial reconstruction was endoscopically assisted. Second stage involved exchanging the expander with a silicone gel implant (Mentor) nearly 7 months later (range, 6–9 months). In addition to the previous procedures, further reconstruction of the nipple–areola complex was performed in 4 patients. Table 1 lists the patients' data, including tumor type, primary oncological surgery, and axillary lymph node status.
ChT, chemotherapy; IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma; MRM, modified radical mastectomy; RT, radiotherapy.
Equipment
A 30° angled 10-mm endoscope (Storz), fiberoptic lighted L-shaped retractor (Assi), and a U-shaped retractor with an endoscope hole (Snowden-Pencer) with routine endoscopic forceps and scissors were the main tools. LigaSure™ (Atlas, ValleyLab) was used as a hemostatic and muscle-sectioning device.
Preoperative markings
Drawings were done when the patient was in the upright position. The axillary crease was marked, as was the posterior axillary axis. A lazy S marking was drawn 6–8 cm below the crease on the posterior axillary axis. Additionally, another 1–1.5 cm marking was drawn nearly 15–18 cm below the upper marking, also on the posterior axillary axis. This marking was modified intraoperatively according to the progress of dissection. Finally, the other relevant markings on the breast were done, including the inframammarian sulcus, previous mastectomy scar, and the midline (Fig. 1).
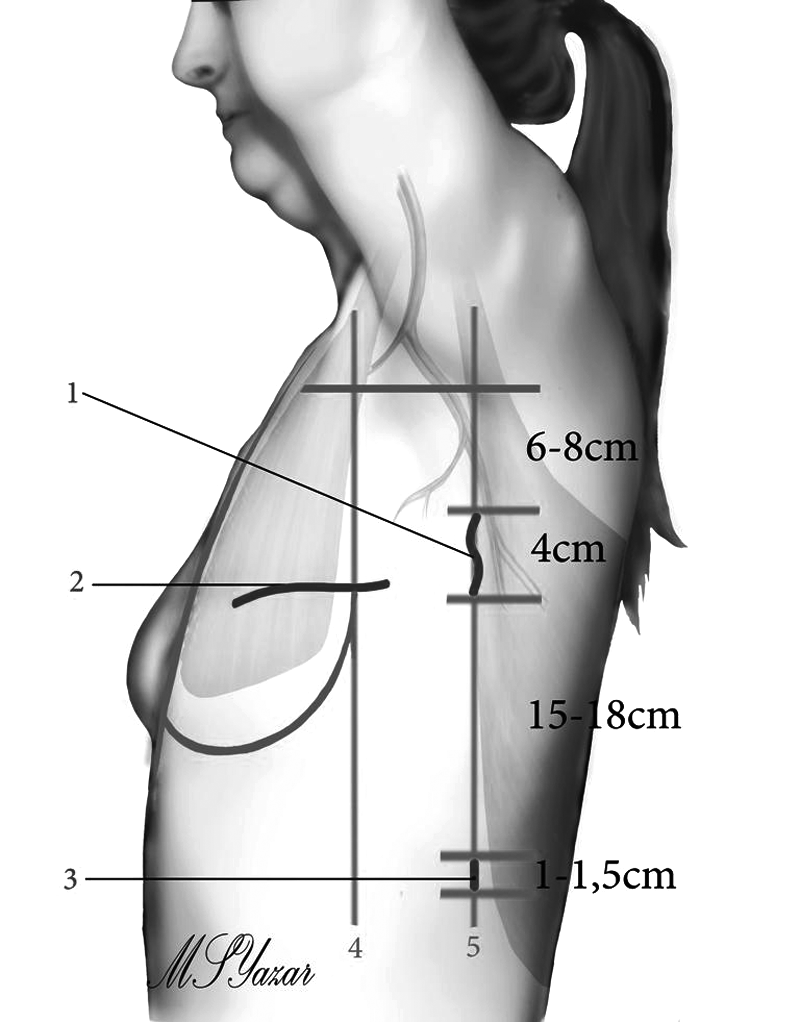
Preoperative markings. “1” indicates the primary 4-cm S-shaped incision, whereas “2” is the transverse incision made on the previous mastectomy scar. “3” is the lower 1–1.5-cm-long incision made, which can be modified intraoperatively.
Operative technique
The patient was placed on a lateral decubitus position on the table, and the trunk was draped. The relevant upper extremity was also draped and left mobile in the operative field. A tumescent solution of 1000 mL Lactated Ringer with 1 mg adrenaline and 75 mg of lidocaine was injected above the LD muscle into the subcutaneous tissue excluding the pedicle area. As the surgeon stood in front of the monitor, he made a superior incision and accessed the LD muscle. The muscle was dissected from the skin and subcutaneous tissues with the help of the L-shaped fiberoptic retractor under direct vision, if possible (Fig. 2).
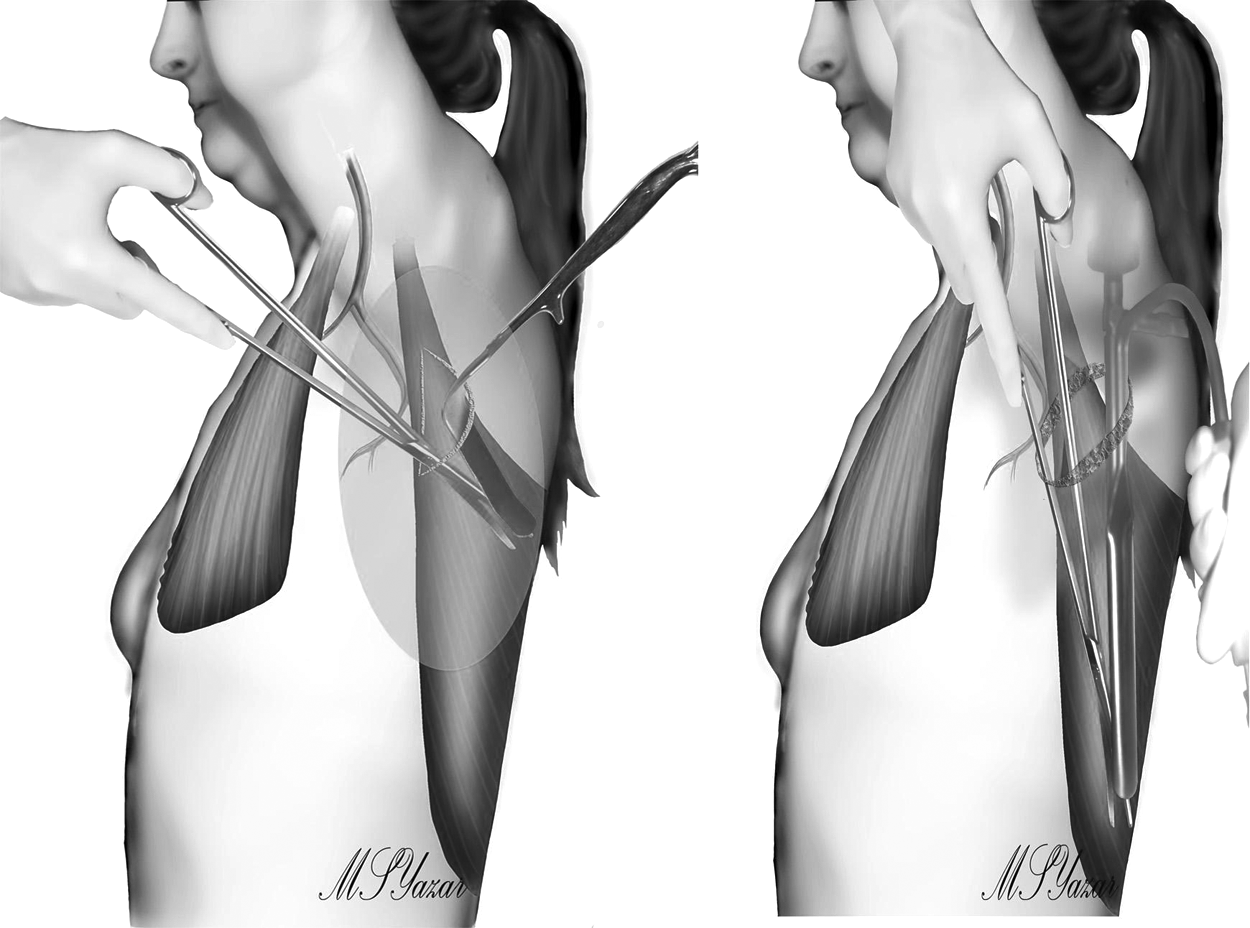
Separation of the latissimus dorsi (LD) from skin with the L-shaped fiberoptic retractor (left) and the U-shaped retractor (right).
After the initial dissection, the 10-mm 30° endoscope and U-shaped retractor were placed beneath the incision to dissect the remaining of LD from the skin. Later, the superolateral border of LD was visualized again and separated from the thoracic wall with endoscopic assistance (Fig. 3). At this time, the intercostal perforators were visualized clearly with the endoscope and easily sealed and divided with the EBVS (Fig. 4).

Dissection of LD using the 10-mm 30° endoscope and U-shaped retractor. Muscle-thoracic wall dissection (left) and anterior muscle border dissection (right) are demonstrated.
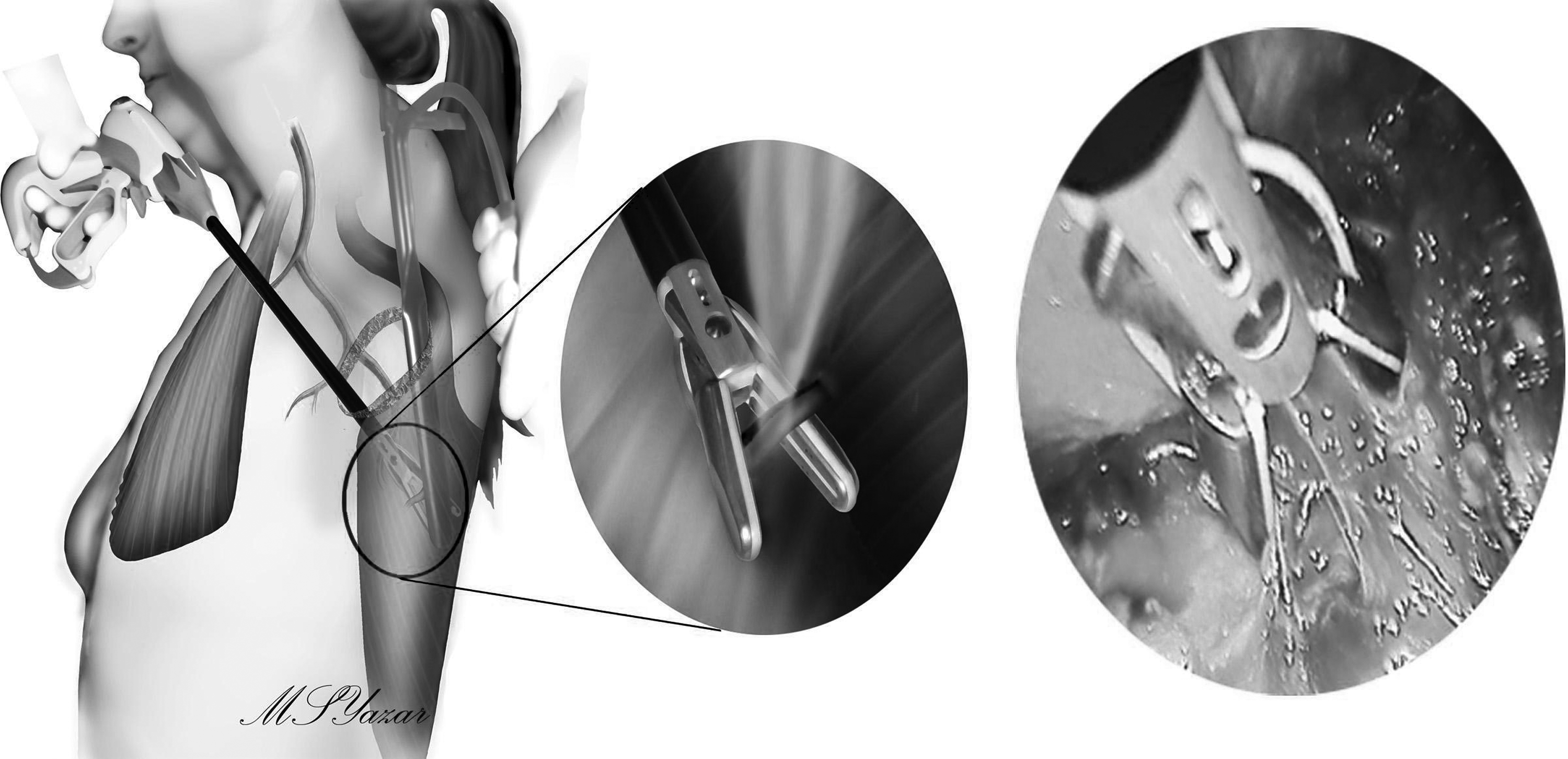
Schematic view of the LigaSure Atlas sealing the intercostal perforators.
At this point, the LD was still attached to the inferior iliac bone and superior humeral, and the medial parts of the muscle were still undissected and intact. To free the distal inferior border of the muscle, a second incision 15–18 cm below the initial incision was done, as demonstrated in Figure 1. The surgeon then inserted the endoscope and the U-shaped retractor into the upper incision. The LigaSure, inserted into the lower incision, was used to separate the inferior muscle attachments (Fig. 5).
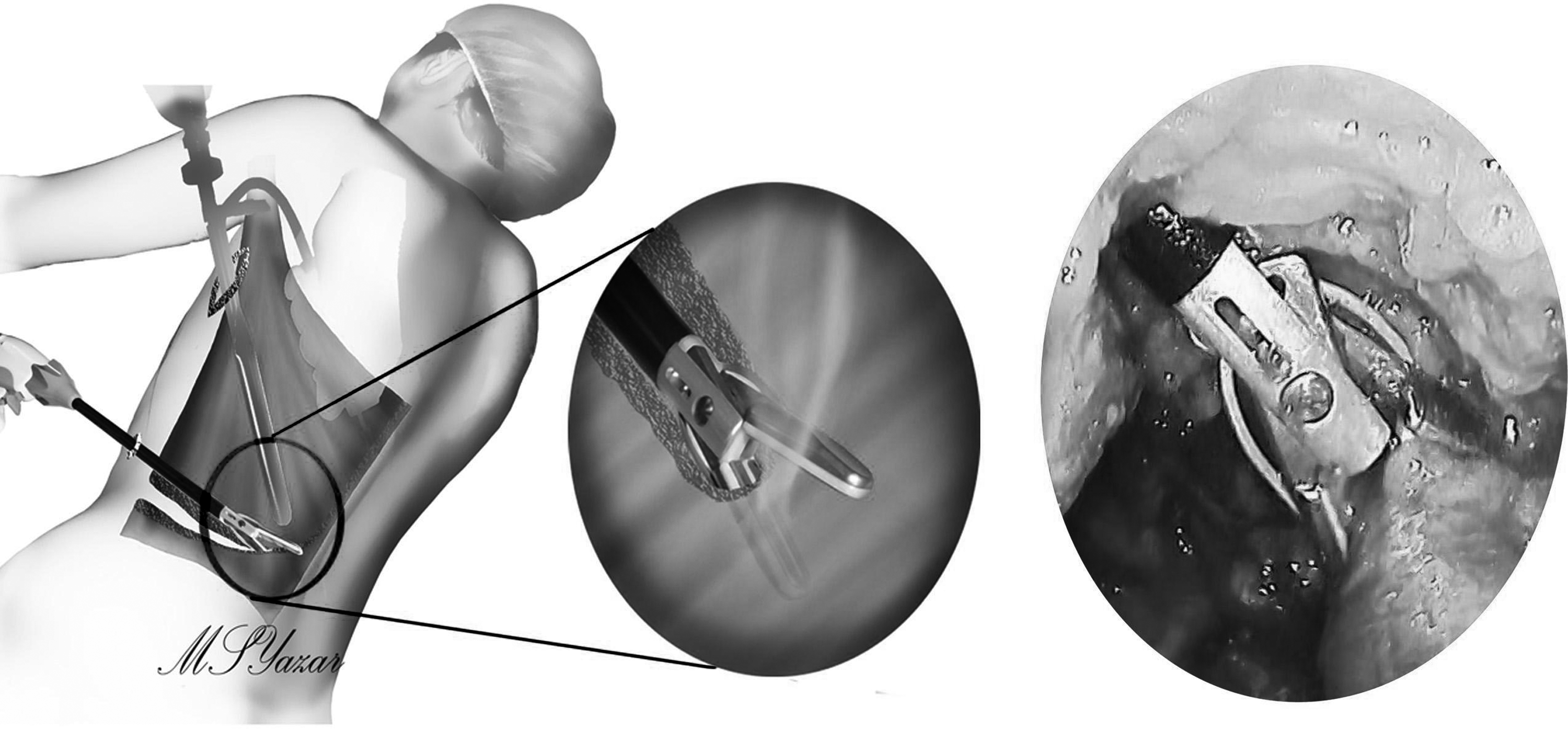
Separating the inferior attachments of the LD using the LigaSure Atlas inserted from the lower incision.
The midline region was then reached. The inferosuperior dissection started from the posterior midline to separate the muscle from vertebral attachments. Later, humeral attachment together with the thoracodorsal nerve was cut, which left the flap totally free in the surgeon's hand. Later, the previous mastectomy scar was excised without changing the patient position on the table. A subcutaneous tunnel was developed between the previous scar and the superior axillary incision regions to pass the LD anteriorly. The muscle was transferred, and the posterior incisions were closed under two suction drains.
The patients were then placed in supine position. The PM muscle was visualized, and its inferior and medial borders were separated from the thoracic wall. The LD was fixed to the medial sternal area with absorbable sutures. Then, to recreate the inframammarian fold, the LD was fixed to the predetermined sulcus-defining points by using the same absorbable suture materials. A suitable expander prosthesis was placed beneath the muscle. To cover the upper one-third of the implant, the previously freed PM was sutured to the LD inferomedially. With the prosthesis totally covered by muscle and a suction drain placed, the skin was closed in an intradermal fashion (Fig. 6).
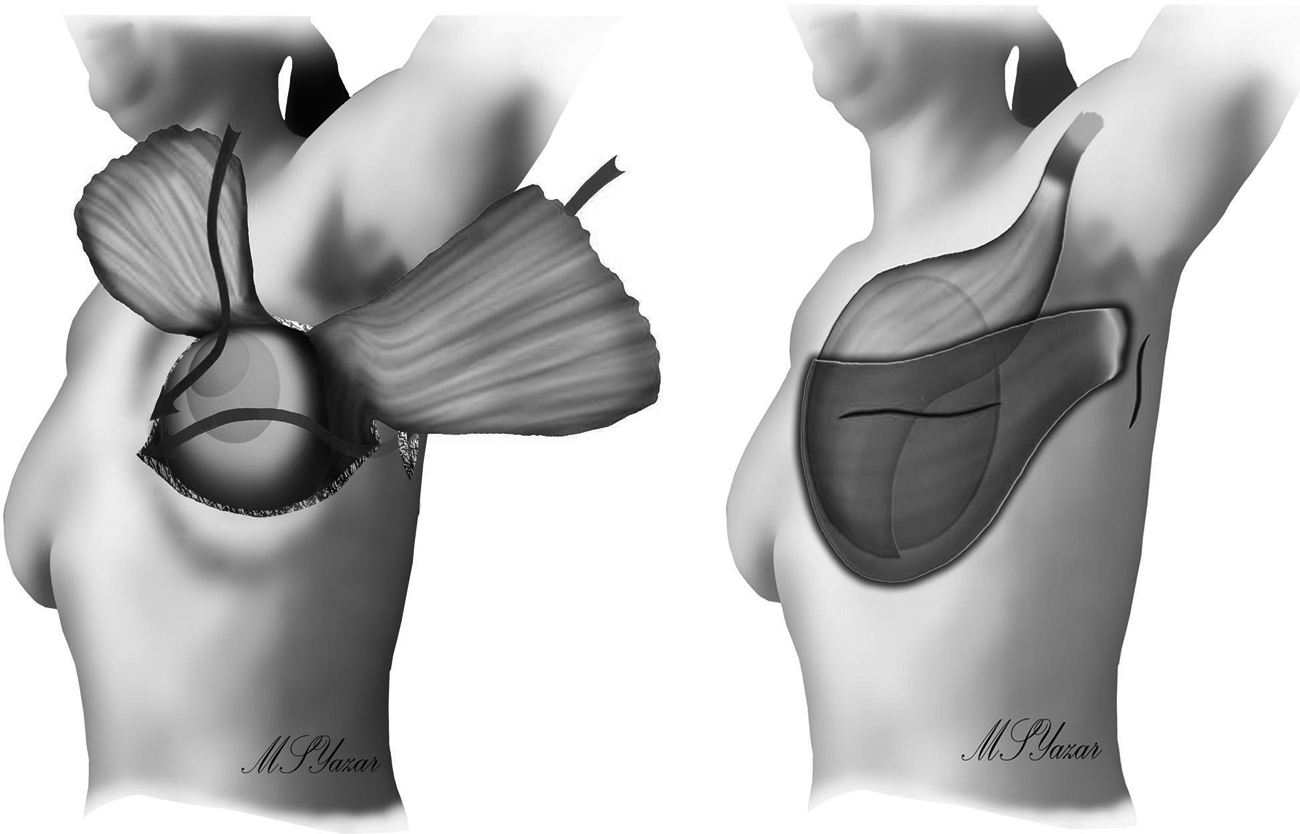
Placement of an expandable prosthesis and coverage by the LD and pectoralis major muscles. Note that the pectoralis major forms the upper medial borders, whereas the LD forms the inferomedial borders of the pocket (left). Total coverage of the expander with muscles after closure of the skin (right).
Results
In the 2-year period between 2006 and 2008, 11 female patients (median age, 37.9 years; range, 20–49 years) had postmastectomy breast reconstruction with endoscopic LD flap harvesting using the LIG system (Fig. 7). The harvesting time was shortened as the surgeon became more experienced with the procedure, and the mean harvesting time was 74.2 minutes (range, 50–125 minutes). Patients were hospitalized from 3 to 7 days, with a mean hospitalization period of 4.5 days. Patients with a hemoglobin level <7 g/L were transfused, but only 2 patients required 1–2 units of autogenous blood. Total amount of drainage postoperatively averaged 950 mL (range, 785–1075 mL), which is markedly less than those reported by previous standard LD-harvesting surgeries. 6 Daily drainage of <25 cc was the criterion for drain removal, and the donor region suction drain remained for an average of 11.6 days (range, 10–15 days). Table 2 lists the detailed data about each procedure.
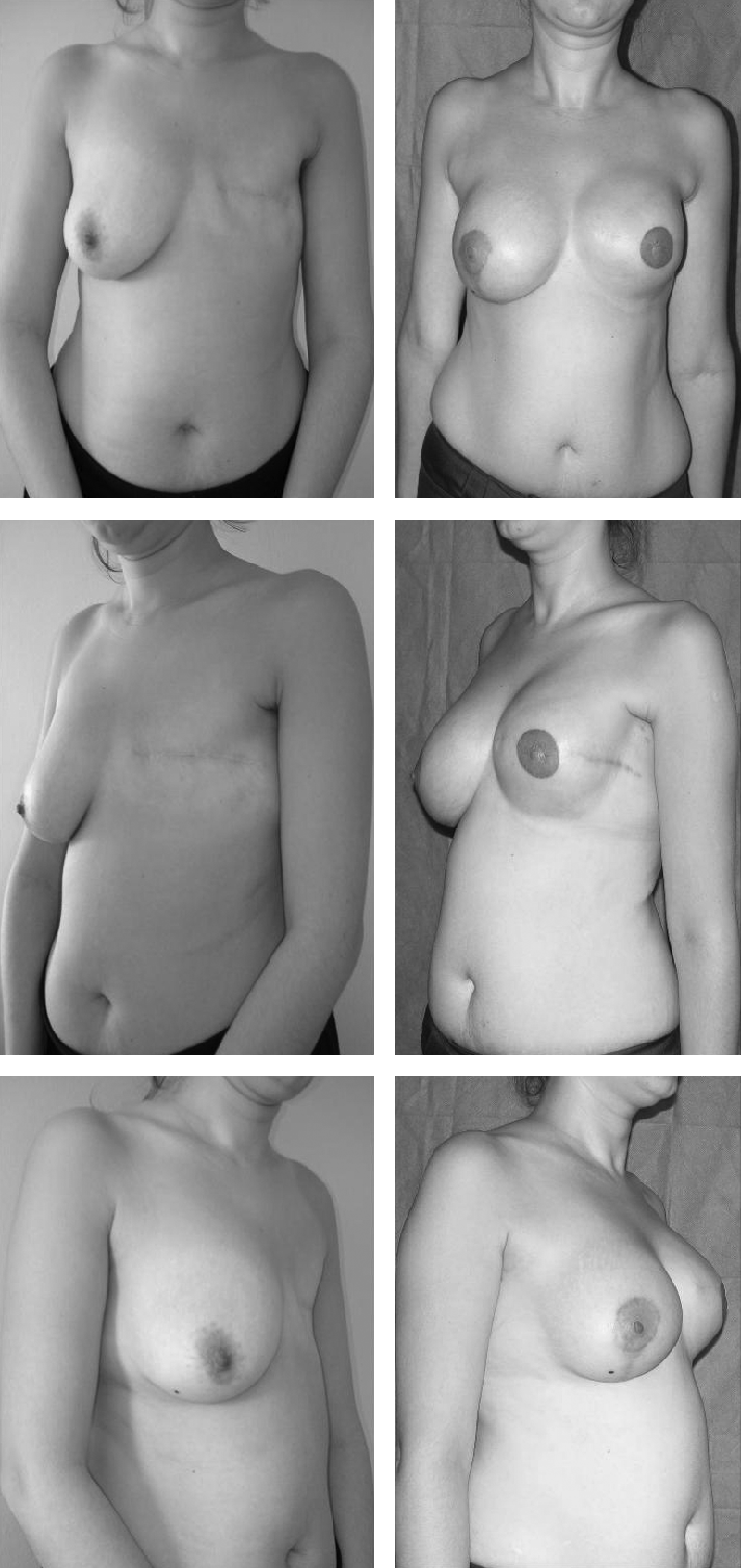
Appearance of Patient 8 on table 2 at 11 months postoperatively. Augmentation mastopexy was performed on the contralateral breast to achieve symmetry.
Note the decline in the operation time.
Patients 9 and 12 are the same patient who had a bilateral reconstruction at different times.
In terms of complications, we did not observe any flap necrosis or hematoma formation. Only 1 patient had an implant infection requiring broad-spectrum antibiotics, whereas another patient had a wound infection, which was treated conservatively. In addition, 1 patient had a seroma at the donor region, which was treated with repetitive aspirations and bandage applications. Table 3 lists the complication data.
Discussion
Today, endoscopic surgery has become an indispensible part of many surgical branches such as general surgery, urology, and gynecology. Utilization of endoscopy in plastic surgery has become more popular, particularly in the last decade.10,11 In 1994, Friedlander and Sundin 12 were the first to report endoscopic LD harvesting in cadavers and pigs. After 3 years, the first use of the procedure in secondary breast reconstruction was reported by Cho et al. 13 Endoscopy certainly has many advantages in terms of flap harvesting, including improved visualization of deep body structures, shortened hospital stay, and decreased postoperative pain.4–6 Further, the limited incisions lead to decreased scar formation and a better cosmetic outcome.
Although newer surgical techniques have evolved over the years, hemostasis is still a crucial part of a successful surgery. Hundreds of articles have been published concerning various techniques of bleeding control, including clips, sutures, ultrasonic coagulation, as well as monopolar and bipolar coagulation systems. 14 One of these coagulation methods is the EBVS, which uses bipolar electrical energy to obliterate the lumen of the vessel. The generator is designed to apply a precise amount of pressure and energy to the vessel wall to unite collagen and elastin, thus forming single structure and occluding the vessel lumen. The EBVS can effectively seal and divide vessels up to 7 mm in diameter, in contrast to the regular bipolar vessel seals, which are effective only in vessels smaller than 2 mm in diameter.15,16 Vessels are easily sealed in one application and divided later. Although it produces a significant amount of energy, the EBVS has been shown to cause less harm to the surrounding tissues and produce less smoke, the latter aiding in visualization. Many animal and human studies have demonstrated the efficacy of the LIG in a wide variety of fields, including general surgery, urology, etc.8,16 Despite its widespread use in other surgical fields, there have been no published reports of EBVS use in plastic surgery, particularly for endoscopic plastic surgery.
Comparative studies with other hemostatic devices have demonstrated the superiority of the LIG system in terms of ease of dissection, shorter operative time, and decreased blood loss.8,9,17 Diamantis et al. 14 have compared the effects of monopolar coagulation, electrocoagulation, bipolar electrocoagulation, ultracision (an ultrasonic coagulating shear), and EBVS on gastric vessels, experimentally. They investigated parameters such as blood, pus, other free peritoneal fluid, or perforation together with the histological analysis of thermal damage. They found EBVS and Ultracision to be more effective and safe compared with monopolar and bipolar coagulations. Hagen et al. 17 compared the conventional suture ligature and EBVS in abdominal hysterectomy cases and found no significant difference in terms of operative time, blood loss, hospital stay, and complications. This emphasizes the effectiveness of EBVS as equal as conventional sutures.
In this study, we used an ipsilateral LD flap and an expander prosthesis to reconstruct the breasts of 11 women who had undergone mastectomy for the treatment of breast cancer. The LD flap was harvested with endoscopic assistance using the EBVS system as the main hemostatic device (in contrast to the routine methods such as clips, monopolar or bipolar coagulators, and sutures). The EBVS was used mainly for sealing the intercostal perforators reaching the LD and liberating the inferior and medial borders of the muscle from the iliac crest and vertebrae, respectively. During the dissection of the LD muscle endoscopically, we easily coagulated the perforators. Although Karp et al. 18 previously reported the difficulty of dissecting the distal and medial muscle attachments, the LIG allowed for quick separation of these distal muscle attachments with almost no bleeding during this separation. As with most surgeons, we found the LIG system practical and easy to use. The double jaws of the device allowed for precise placement on the target vessel both under direct vision and endoscopically. An audible sound informed the surgeon that vessel ligation was complete.
Operation time
In terms of operation time, various reports have been published about LD harvesting. Eaves et al. 19 reported a free LD muscle harvest time of 3 hours, whereas Robb and Miller 20 reported a harvest time of nearly 2 hours for breast and chest reconstruction. The endoscopic technique does have a learning curve because of the lack of tactile sensation and the two-dimensional nature of the procedure. New tools and setups also prolong the surgery. For example, Missana and Pomel 6 reported a mean surgical time of 238 minutes (range, 192–360 minutes) and suggest more practice to lower this time. Lin et al. 21 reported an average of 88.8 minutes for LD harvesting using the traditional technique, whereas endoscopic harvesting took an average of 90.3 minutes. In our series, we experienced the same difficulty reported by Missana and Pomel, 6 that is, LD harvest in the first operation took around 120 minutes, but as we became accustomed to the surgery, the time decreased to 50 minutes. This decrease was not solely due to our greater experience, but also due to our adaptation to the EBVS device.
Hospital stay
Various reports on the hospital stay of patients have been published. Missana and Pomel 6 reported that the average length of hospital stay was 5.6 days (range, 2–12 days). Patients were discharged with the dorsal drain in place, which was removed on postoperative day 15. Vasconez, 22 on the other hand, believed that a 5-day hospital stay was excessive, as his patients stayed for an average of 3 days. We know that the endoscopic method results in less operative donor site pain and better upper extremity motion postoperatively. 21 We initially kept patients in the hospital for 5–6 days, but were able to progressively shorten this time without an increase in complications or complaints (range, 3–7 days). We do not know whether this shortened stay is due to decreased incision length, less donor site pain, or increased postoperative mobility. We also cannot rule out regional differences, type of reconstructions, and the surgeon preferences as affecting the length of hospital stay. Nevertheless, we believe that EBVS usage, leading to less bleeding, seroma formation, and damage to surrounding tissues, might shorten the hospital stay.
Postoperative drainage
The literature discussing postoperative drainage and seroma formation following LD harvesting is inconsistent. Missana and Pomel 6 reported 2500 mL of lymphatic drainage (range, 950–6380 mL) when the drain was removed on postoperative day 15. In contrast, Vasconez 22 reported that having the patient lie on her back decreased seroma formation, and he removed the drains 3–5 days postoperatively regardless of the harvesting method. Lin et al. reported an average postoperative drainage of 557.7 mL, which is less than those previously reported. No differences in postoperative seroma formation have been observed between the traditional and endoscopic methods. 21 In our series, we observed much less drainage formation than that reported by Missana and Pomel. 6 Our average date of drain removal was postoperative day 11.6 (range, 10–15 days), with an average drainage of 950 cc (range, 785–1075 mL; Fig. 8). Although Lin et al. reported an average postoperative drainage of 557.7 mL, their values ranged from 167 to 1400 mL, and no consistency was attained. In the present study, intraoperative bleeding amount was 81.6 mL (range, 45–145 mL), which is a little less than the ones reported by Lin et al. (105 mL). The reduced drainage when using the EBVS system may be related to its effective sealing of vascular structures, including the lymphatic vessels. 21 A study by Novitsky et al. 23 demonstrated the efficacy of EBVS on sealing lymphatic vessels in pigs. Unfortunately, the etiology of seromas remains unknown, although numerous causes have been proposed, including disruption of lymphatic and vascular channels, shearing effects between subcutaneous tissues and muscles, surgically created dead spaces, and increased inflammatory mediators. 24 We believe that the decreased rate of seroma formation in our patients results from the efficacy of the EBVS system on sealing lymphovascular structures. Only 1 patient had visible seroma, which was treated conservatively. Hematoma was not observed at all. Only 2 patients received autologous blood transfusions postoperatively.

Mean drainage amounts. Drains were removed on the 12th day postoperatively. The shaded blue area represents the average amount of drainage of all patients (950 cc).
Previous reports have shown that the EBVS causes minimal sticking, charring, or peripheral thermal spread, while also creating a seal that is quite resistant to dislodgement. 15 This system leads to less accidental injuries and saves time by grasping, coagulating, and transecting vessels in a minimal number of steps, avoiding frequent instrument usage. 15 In terms of wound healing, EBVS was found to be less harmful to surrounding tissues, which is particularly important for plastic surgeons. 25 Less damage to the harvested flap, as well as a more secure pedicle, will increase the success rate of reconstruction, which is especially useful in more sophisticated flap operations such as perforator flap harvesting or free flap procedures.
Conclusions
For the first time, we report the use of EBVS in endoscopic plastic surgery, specifically for LD flap harvesting for breast reconstruction. We found this device easy to use, as it was safe, bloodless, and quick to perform. Perforators and muscle attachments were easily sealed with EBVS, decreasing the operative time markedly. The total amounts of drainage, transfusion needs, and hospital stay were less than those previously reported.
In conclusion, the bipolar vessel sealer EBVS brings many advantages to LD flap harvesting, and its utilization will improve this procedure and help the field of plastic surgery as a whole. However, more randomized controlled studies in larger groups of patients, whether reconstructive or aesthetic, are required to show the EBVS's effectiveness in terms of decreased hospital stay, drainage amount, and operative time. These larger studies should also address the overall cost-effectiveness of the EBVS system given the relatively high cost of the device.
Disclosure Statement
No competing financial interests exist.