
Abstract
Abstract
Background/Purpose:
One-trocar surgery (OTS) includes all video-surgical techniques performed using a single 10-mm port and an operative scope. These techniques can be completely endoscopic or endoscopic assisted. Since 1997, OTS has become the approach of choice in our institution for a variety of laparoscopic, retroperitoneoscopic, and thoracoscopic operations. We report our experience with this technique.
Methods:
Four hundred fifty-eight patients (age range, 3 months to 17 years) underwent OTS from October 1997 to December 2008. The procedures were transumbilical laparoscopic-assisted (TULA) appendectomy (182 patients), TULA small bowel resection (14 patients), TULA intestinal biopsies (7 patients), laparoscopic adhesiolysis (6 patients), laparoscopic-assisted liver biopsies (5 patients), laparoscopic revision of peritoneal dialysis catheter (3 patients), retroperitoneoscopic varicocelectomy (202 patients), retroperitoneoscopic-assisted renal biopsies (4 patients), retroperitoneoscopic drainage of posttraumatic urinoma (1 patient), retroperitoneoscopic-assisted pyeloplasty (15 patients), and thoracoscopic pleural debridement and decortication for empyema (19 patients).
Results:
The procedure was completed using only one trocar in 399 cases (87.1%). All conversions to multitrocar or open surgery were elective and regarded the retroperitoneoscopic approach during the learning curve (28 of 222, 12.6%; 21 varicocelectomies and 7 pyeloplasties) and the TULA appendectomy because of the appendix mobilization failure (31 of 182, 17%). There were no intraoperative or postoperative complications related to OTS. Wound infection was observed after two TULA appendectomies (1.3%).
Conclusions:
According to our experience, OTS is a feasible and versatile technique in pediatric surgery, providing a safe, effective, and the least invasive treatment for several different diseases.
Introduction

One-trocar surgery instruments.
Patients and Methods
A retrospective cohort comprising 458 children operated with OTS approach between October 1997 and December 2008 in a single pediatric surgical center were audited.
The indications for OTS laparoscopic approach were appendicitis (182 patients), gastrointestinal bleeding (12 patients), abdominal cysts (3 patients), Hirschsprung's disease (HD) (3 patients), suspected hypoganglionosis (3 patients), recurrent abdominal pain in previous laparotomy (6 patients), liver diseases (5 patients), and peritoneal dialysis catheter dislocation (3 patients). The indications for OTS retroperitoneoscopic approach were grade 3 varicocele (202 patients), suspected renal lymphoma localization (2), nephrotic syndrome (2 patients), ureteropelvic junction (UPJ) obstruction (15 patients), and posttraumatic pararenal urinoma (1 patient); OTS thoracoscopic approach was performed for multiloculated pleural empyema (19 patients).
The following parameters were analyzed: technical problems in the performance of the procedure, operative time, intraoperative complications, postoperative complications, postoperative stay, recurrence, cosmesis.
For dichotomous outcomes, Fisher's exact test was performed, with a significance assessed at a P value of less than .05 (two-tailed).
Surgical technique
One-trocar laparoscopy
The patient is placed in a supine position on the operating table. A 10-mm Hasson trocar is inserted in an “open” fashion through the umbilicus and pneumoperitoneum established up to a pressure of 12 mm Hg. The operative scope is introduced and a complete exploration of the abdominal cavity is performed.
Transumbilical laparoscopic-assisted surgery:
Appendectomy. The appendix is grasped laparoscopically with an atraumatic instrument introduced through the operative channel of the scope and externalized through the umbilicus. Appendectomy is performed outside the abdominal cavity using the conventional technique (Fig. 2). At the end of the procedure, the bowel is returned inside the abdominal cavity and the laparoscopic control always performed. If the transumbilical intestinal exteriorization is unsuccessful, laparoscopic multitrocar or laparotomic conversion is necessary.
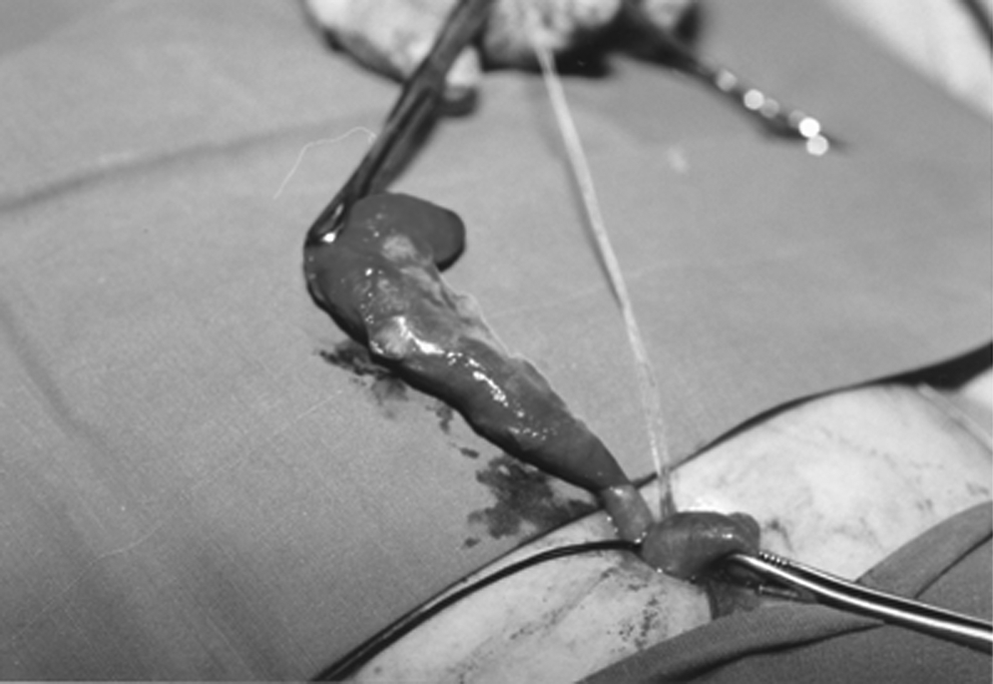
Appendix externalized through the umbilicus.
Meckel's diverticulum and small bowel pathologies. The affected loop is grasped and exteriorized through the umbilicus for the extracorporeal conventional surgery (diverticulectomy, intestinal resection, and anastomosis). When the bowel anomaly is not directly identified during the laparoscopic exploration, the terminal ileum is transumbilically extracted and the small bowel is examined outside the abdominal cavity.
Intestinal biopsies. Seromuscular or full-thickness biopsies of the colon and ileum are similarly obtained in selected cases of HD (total colonic HD and rectosigmoid HD to identify the level of ganglionated bowel during transanal endorectal pull-through), suspected hypoganglionosis after rectal suction biopsies, and extended vascular intestinal malformation.
One-trocar intracorporeal laparoscopy:
Adhesiolysis. Diagnostic laparoscopy is performed using the operative laparoscope. Intestinal adhesions to the abdominal wall are lyzed with scissors or by diathermy introduced through the operative channel. Additional trocar can be required when the adhesions are too extensive.
Revision of peritoneal dialysis catheter. The trocar is inserted using the open approach in the lateral quadrant opposite to the catheter exit site to obtain a greater operative space. The displaced catheter is freed from the possible adhesions and moved in the proper position.
Liver biopsies. Tru-cut biopsies are percutaneously obtained under laparoscopic control. Hemostasis is accomplished by compression on the sites of the biopsies.
One-trocar retroperitoneoscopy
The patient is placed in flank position. A 10-mm Hasson trocar is inserted in an “open” fashion below the apex of the 12th rib (Fig. 3), and CO2 is insufflated up to a pressure of 12–15 mm Hg. The retroperitoneal dissection to develop the working space is performed under visual control using a blunt-tipped dissector inserted through the operative scope. The psoas muscle is the main retroperitoneoscopic landmark.

Incision for one-trocar retroperitoneoscopy.
Varicocelectomy: Following the psoas muscle, the ureter and spermatic vessels are identified. The vessels (both artery and vein) are cauterized with bipolar forceps and cut.
Pyeloplasty: The kidney is mobilized posteriorly and the ureter identified. The ureteropelvic junction and the pelvis are endoscopically isolated and externalized through the trocar incision to perform a conventional pyeloplasty outside the abdominal cavity (Fig. 4).
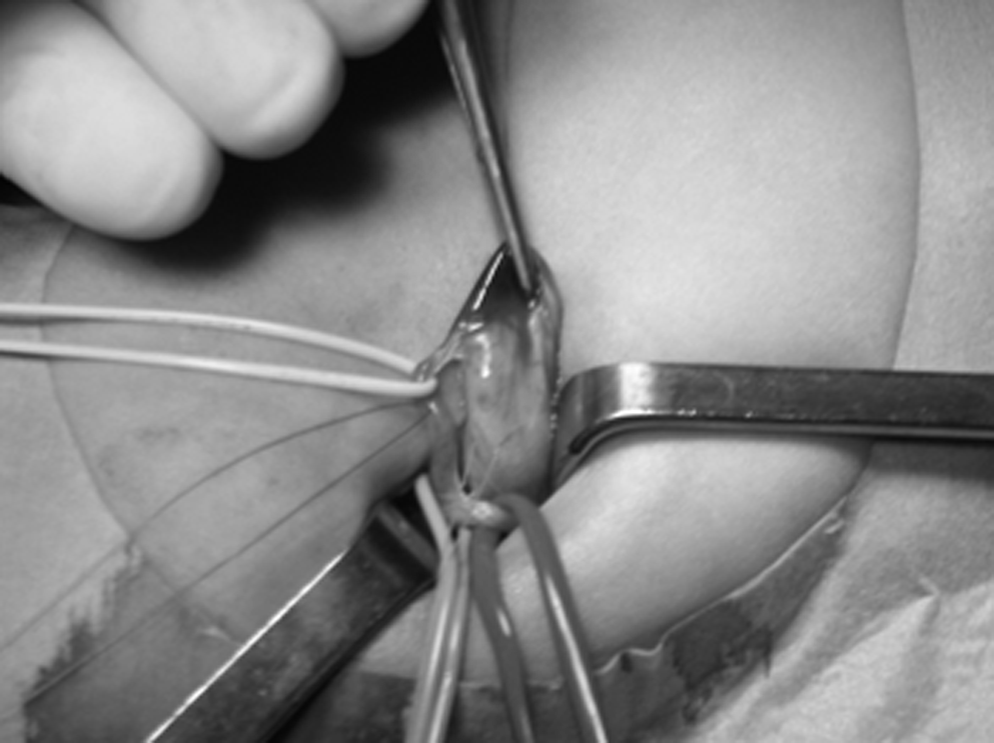
Ureteropelvic junction externalized in one-trocar–assisted pieloplasty.
Renal biopsies: Biopsies are performed both percutaneously, under retroperitoneoscopic control, or endoscopically, using a spoon biopsy forceps.
Drainage of posttraumatic urinoma: A large drainage tube is inserted into the retroperitoneal space through the operative channel of the scope, after minimal retroperitoneoscopic dissection.
One-trocar thoracoscopy
Pleural empyema: The patient is placed in full lateral position. Single lung ventilation is not mandatory, but in some instances it facilitates the procedure. A 10-mm Hasson trocar is inserted in an “open” fashion on the middle axillary line at the 4th–5th intercostal space, and CO2 is insufflated up to a pressure of 4 mm Hg. The operative scope is introduced and pleural adhesions are initially disrupted with the camera movements inside the pleural space. Pleural debridement is performed: fibrinous septa are completely disrupted using endoscopic blunt tip dissectors; fluid is aspirated and debris removed from the pleura. In the more advanced empyemas, decortication is performed by removing the organized material from the visceral and the parietal pleural surfaces. At the end of procedure, a large chest tube is positioned under vision through the trocar site.
Results
OTS was performed on 458 children. The mean age was 6 years (range, 3 months to 17 years). The operations were 217 OTS laparoscopies: 182 transumbilical laparoscopic-assisted (TULA) appendectomies, 14 TULA small intestine resection (10 bleeding Meckel's diverticulum, 2 cystic Meckel's diverticulum, 1 cystic duplication, 1 jejunal hemangioma), 7 TULA intestinal biopsies (1 extended intestinal vascular malformation presented with bleeding, 1 total colonic HD, 2 rectosigmoid HD during transanal endorectal pull-through, 3 normal histology in suspected hypoganglionosis), 6 adhesiolysis, 5 laparoscopic-assisted percutaneous needle liver biopsies (1 metastatic Wilms' tumor, 1 focal nodular hyperplasia, 1 histiocytosis, 2 cirrhosis), and 3 revisions of peritoneal dialysis catheters; 222 OTS retroperitoneoscopies: 202 varicocelectomies, 4 renal biopsies (2 lymphomas, 2 nephrotic syndromes), 15 pyeloplasties, and 1 drainage of a posttraumatic perirenal urinoma; 19 OTS thoracoscopic pleural debridements and decortications for empyema.
The operation was completed using only one-trocar in 399 cases (87.1%). There were no intraoperative or postoperative complications related to OTS. The operating times and hospital stay for the different procedures are shown in Tables 1 and 2, respectively. All conversions to multitrocar or open surgery were elective. During the learning curve, 21 of 202 (10.3%) varicoceles needed conversion to laparoscopic transperitoneal varicocelectomy because of the lack of orientation during the retroperitoneoscopic dissection and impossibility to identify the spermatic vessels. There were technical difficulties in 7 of 15 (46.6%) pyeloplasties, because of a fixed ureteropelvic junction or polar vessels, which did not allow the ureteropelvic junction extraction outside the abdominal cavity; all these 7 patients needed elective conversion to open surgery.
1 patient: 32 minutes.
1 patient: 20 days.
Thirty-one of 182 (17%) appendectomies needed open conversion because of the appendix mobilization failure caused by a fixed cecum or peritonitis. Umbilical wound infection was observed after two TULA appendectomies (1.3%).
At follow-up (range, 6–140 months), varicocele persistence/recurrence occurred in 21 of 181 (11.6%) retroperitoneoscopic varicocelectomies and recurrent ureteropelvic junction obstruction was observed in 1 patient (6.7%).
Discussion
Minimally invasive techniques have the advantages over open surgery in terms of trauma, postoperative pain, and cosmetic results. Most of the laparoscopic, retroperitoneoscopic, and thoracoscopic procedures described in literature are performed using two to five trocars for the scope and the instruments. The operative scope allows operating using only one-trocar and few instruments.
The first description of OTS was appendectomy and was published in 1992 by Pelosi and Pelosi. 1 In 1998, Esposito 2 reported his initial experience in performing OT appendectomy in 25 children. He concluded that the one-trocar appendectomy is easy to perform, but the use of the operative scope can be difficult because of the co-axial movement of the camera and the instrument, which sometimes makes difficult organ exploration and manipulation. In our experience, OTS has been a safe and effective approach, with minimal complications and better cosmetic results (Fig. 5) than open or multitrocar surgery. 3 As our experience with OTS has increased, we have been able to expand its application in many pediatric surgical fields. In this study, 458 operations were performed. The predominant procedures were TULA appendectomies (182 cases) and retroperitoneoscopic varicocelectomies (202 cases), but OTS was also applied in many selected surgical procedures without extensive laparoscopic organ manipulation.

Cosmetic results after transumbilical laparoscopic-assisted small bowel resection for Meckel's diverticulum.
In our experience, appendectomy was easily performed in uncomplicated appendicitis, when preoperative ultrasound did not reveal sign of perforation; however, elective conversion to open surgery was necessary in 17% of cases because of the cecum and appendix mobilization failure. After the learning curve, the operative time for appendectomy became shorter, but the conversion rate did not change. It is still controversial whether the retrieval of the appendix through the umbilicus results in a higher infection rate compared with other laparoscopic or open techniques. In 2008, Visnjic 4 compared TULA appendectomy with laparoscopic appendectomy in children. The author reported a wound infection rate of 13.7% and 4.6%, respectively, concluding that this infection rate was not significant (P value = .17). Recently, Sesia et al. 5 conducted a retrospective chart review of 262 children with acute uncomplicated appendicitis who underwent OT appendectomy, reporting a 2.7% infection rate. In our series, the wound infection rate after TULA appendectomy was 1.3%. We suppose that our lower infection rate was related to the preoperative selection of the patients in whom TULA approach was performed only in case of uncomplicated appendicitis, without preoperative clinical and ultrasonographic signs of perforation. Moreover, laparotomic conversion was our preferred choice in patients with higher risk of infections, when a localized peritonitis constricting the mobility of the caecum and appendix was found during the OT laparoscopic exploration.
Intestinal biopsies, small bowel exploration, and resection are also safely performed through the TULA approach. In our series, 14 patients underwent transumbilical small bowel exploration and resection without complications. We found 12 Meckel's diverticulum, 1 ileal duplication, and 1 jejunal hemangioma. The laparoscopic intracorporeal search for Meckel's diverticulum is considered time consuming and not completely reliable. 6
In the jejunal hemangioma case, the child presented with gastrointestinal bleeding and the Meckel's scan was positive. TULA small bowel exploration outside the abdominal cavity was performed and diverticulum was not found; the hemangioma was identified as a small soft palpable lesion of the bowel at about 40 cm from the Treitz, and in our opinion, intracorporeal laparoscopic small bowel exploration could not be effective in this case.
Sauer et al. 7 proposed the umbilical incision to perform colonic biopsies for identify the level of ganglionated bowel before to start the mucosectomy during the transanal endorectal pull-through for HD. In our experience, the TULA approach was an advantageous minimally invasive alternative to perform seromuscular biopsies of the colon and the ileum for total colonic HD diagnosis and rectosigmoid HD to identify the level of ganglionated bowel during transanal endorectal pull-through; full-thickness biopsies were also obtained in patients with suspected hypoganglionosis, after rectal suction biopsies and in a case of extended intestinal vascular malformation.
Malfunction of peritoneal dialysis catheters result from migration of the catheters into the upper abdomen or adhesions. 8 Adhesiolysis and revision of peritoneal catheters can be successfully performed using only one trocar. We performed three peritoneal dialysis catheter revisions. Catheter was freed from adhesions and moved in the proper position; dialysis was started few hours after the procedure and there was no recurrence.
In the last years, OTS have been also successfully applied to perform procedures as revision of the peritoneal shunt catheters for hydrocephalus and gastrostomy in neurologically impaired children.9,10
Regarding OT retroperitoneoscopy varicocelectomy employing the Valla technique, the largest subgroup of patients was undergoing OTS. 11 In this group of patients, the conversion rate of 10.3% was directly related to the learning curve. In fact, in a previous study, we report a 17.6% (17 out of 97 patients) conversion rate to a laparoscopic transperitoneal multitrocar technique because of the difficulty in orientation inside the retroperitoneal space, 12 but in the last 105 cases the conversion rate decreased to 3.8% (P = .002). The recurrence/persistence rates of retroperitoneoscopic varicocelectomy in our previous (11.2%) and present (11.6%) series are similar to other techniques. 12
Retroperitoneoscopic pyeloplasty requires a special laparoscopic skill, mainly in infants, 13 owing to the small operative space. In 2004, Farhat et al. 14 reported the initial experience in performing retroperitoneal-assisted laparoscopic pyeloplasty in 9 children. After retroperitoneoscopic dissection using three trocars, the ureteropelvic junction was brought up through a 10-mm trocar site to the skin level and pyeloplasty was performed over a Double-J stent. In two patients, mobilization of ureteropelvic junction was inadequate and open conversion was performed. One-trocar–assisted pyeloplasty (OTAP) was first described by Lima et al. in 2007. 15 OTAP was performed on 16 patients using the operative scope and there were no conversions. The authors concluded that OTAP allows to perform the Anderson-Hynes pyeloplasty through a 10-mm lumbar incision, especially in very small children and also in presence of crossing vessels. Also, in our initial experience, this approach was more advantageous in infants than in older children; in fact, in infants, the thin abdominal wall allows the externalization of the ureteropelvic junction more easily. The conversion rate was high in our series (46.6%), but in these patients only a small enlargement of the lumbar incision allowed to perform the conventional pyeloplasty. There was one recurrent ureteropelvic obstruction due to an unrecognized proximal ureteral hypoplasia, and therefore, it was not related to one-trocar technique. Caione et al. 13 performed a study comparing the outcomes in young children consecutively enrolled for open dismembered pyeloplasty (25 patients) and OTAP (28 patients). The median operative time was significantly longer with OTAP (95 versus 72 minutes; P < .05). OTAP was superior to open pyeloplasty in terms of postoperative hospital stay (median: 2.4 days with OTAP and 6.1 days with the open procedure; P < .05), postoperative pain, and cosmetic results.
OTS can also be an alternative to the percutaneous ultrasound-guided procedures such as drainage positioning and tru-cut biopsies in selected cases after interventionist radiologist consulting, particularly when the risk of bleeding is high.
Renal trauma is considered a contraindication to laparoscopic surgery. We performed successfully OT retroperitoneoscopy in a patient with a major renal trauma to drain a perirenal urinoma. A large drainage tube was inserted through the operative laparoscope inside the retroperitoneal space and urinoma resolved without complications. OT renal and liver biopsies were also successfully achieved under endoscopic control. Operative scope allowed to perform successful bleeding control after biopsies.
One of the latest innovations in the armory of laparoscopic surgery is the laparoendoscopic single-site surgery. This technique uses a single multichannel (three or four channels) trocar inserted through a single incision; articulating, prebent, and flexible instruments provide a degree of triangulation in the operative field to perform surgical procedures. 16 This new laparoscopic surgery is spreading in adult, but it remains more sporadic in pediatric age. 17 We underline that the laparoendoscopic single-site surgery and OTS are both minimally invasive surgical methods, but they are different laparoscopic techniques with own specific devices. In 2004, Martinez-Ferro et al. reported the single-port thoracoscopic debridement for pleural empyema in 10 children. 18 Thoracoscopy was performed using a single rigid nonvalved thoracoport for the contemporary introduction of a 5-mm scope and 3-mm instruments. We performed OT thoracoscopy for pleural empyema using the operative scope in 19 children without complications, with good cosmetic results and less postoperative pain.
In conclusion, our experience shows that OTS is a versatile, safe, and effective approach in the surgical management of many pathologies in children. The indications for these OT procedures have expanded and can be applied to the minimally invasive operations that do not require great endoscopic viscera manipulation. The operating time is comparable with that of conventional technique and complication rate is low. The main advantage of OTS is the better cosmetic result than multitrocar techniques.
Footnotes
Disclosure Statement
No competing financial interests exist.