
Abstract
Abstract
Background and Purpose:
Simulation-based training in medical education is increasing. Realism is an integral element of creating an engaging, effective training environment. Although physical trainers offer a low-cost alternative to expensive virtual reality (VR) simulators, many lack in realism. The aim of this research was to enhance the realism of a laparoscopic box trainer by using a simple, inexpensive method.
Materials and Methods:
Digital images of the abdominal cavity were captured from a VR simulator. The images were printed onto a laminated card that lined the bottom and sides of the box-trainer cavity. The standard black neoprene material that encloses the abdominal cavity was replaced with a skin-colored silicon model.
Results and Conclusions:
The realism of the modified box trainer was assessed by surgeons, using quantitative and qualitative methodologies. Results suggest that the modified box trainer was more realistic than a standard box trainer alone. Incorporating this technique in the training of laparoscopic skills is an inexpensive means of emulating surgical reality that may enhance the engagement of the learner in simulation.
Introduction
Simulations have the potential to address many limitations of traditional training without jeopardizing patient safety. 4 Constant technologic improvement means that simulators for educating health care professionals continue to grow with increasing fidelity. 5 Such high-fidelity simulations have been shown to be educationally effective. 6 Further, skills acquired in simulation also transfer to the real theater setting. 7 Studies have also shown that surgeons trained on simulators demonstrate a reduced learning curve, compared to those without such training. 1
With the advancement of minimally invasive surgery, many three-dimensional (3D) open surgical fields are being replaced by 2D video images. 8 Sophisticated virtual reality (VR) simulators can now provide recreations of laparoscopic procedures that are anatomically realistic. The simulators provide inbuilt metrics, which enable technical performance to be recorded, measured, and used for structured feedback. 9 Despite providing a high level of realism, VR simulators are expensive and access is thus limited. VR simulators can range from $40,000 to $100,000, depending on the number of modules purchased. Further, this cost does not take into consideration maintenance and upgrade costs. 8
Physical bench-top models, such as the box trainer, provide an inexpensive alternative to VR simulators. Traditionally, a black neoprene skin is placed over the open plastic abdomen, in which laparoscopic ports and instruments can be inserted. The trainee can then learn how to manipulate instruments, for instance, by stacking sugar cubes placed in the box. A standard box trainer costs approximately £975 ($1,463) (e.g., VAT). 8 Although significantly less expensive than a VR simulator, box trainers lack in visual and tactile realism. For instance, the inside and outside of box trainers are made of either white or grey plastic, thus being far from the actual human color of the abdominal cavity.
This is important, because realism plays an crucial part in simulation and “cannot be overstressed”. 10 Ideally, surgeons and residents should train with tools that closely emulate surgical reality. Realism could be enhanced by covering a box trainer with surgical drapes and bringing it into context by placing it into a simulated or real operating room. However, due to a lack of resources of simulated facilities, this might not always be possible. An alternative approach would be not to replicate every detail of a clinical environment or procedure, but rather to replicate clinical cues that tap into actual memory. These cues seem to be sufficient to build a realistic representation. 11 In this article, a simple, inexpensive method is described to enhance the visual realism of a box trainer by recreating the visual cues of the human abdomen.
Materials and Methods
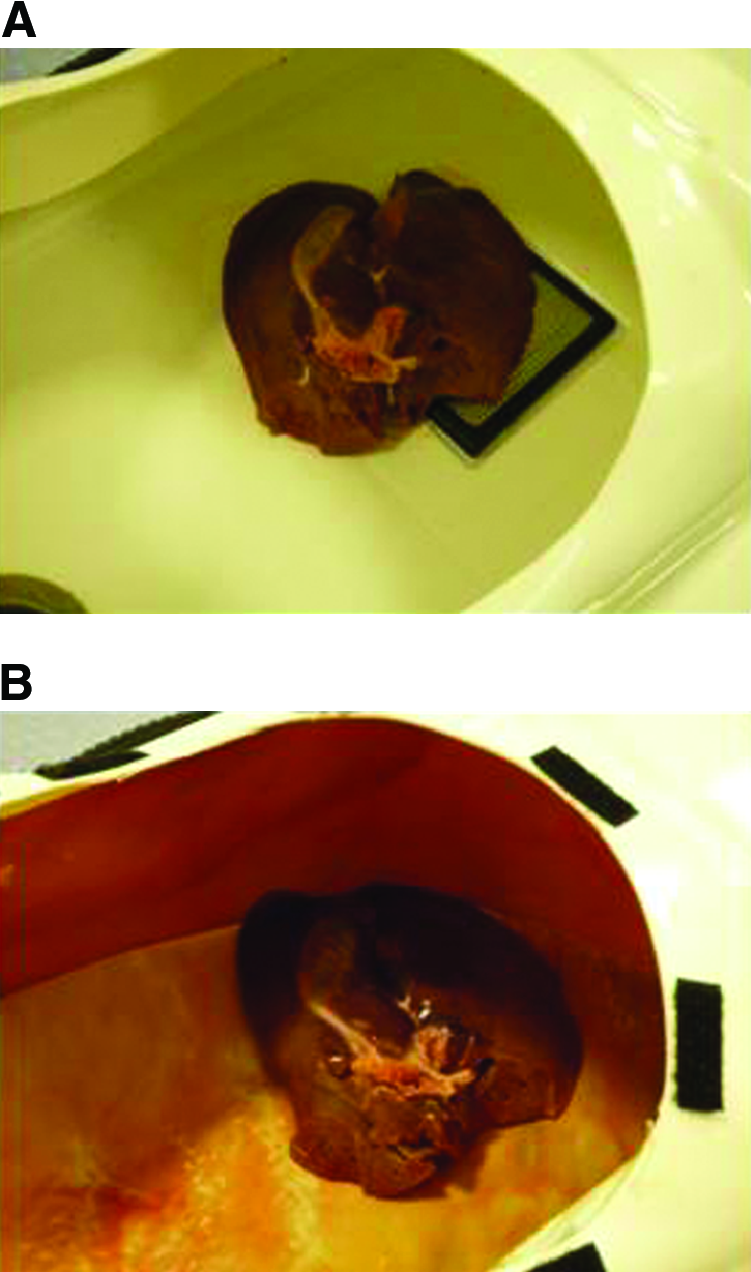
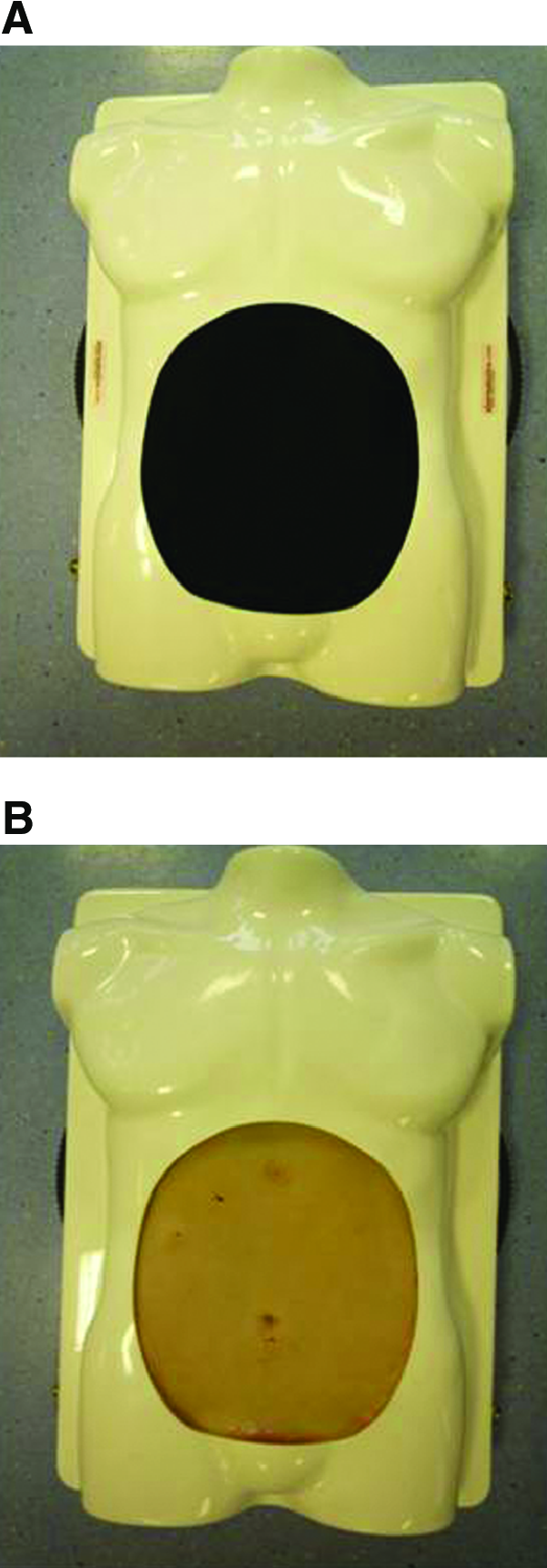
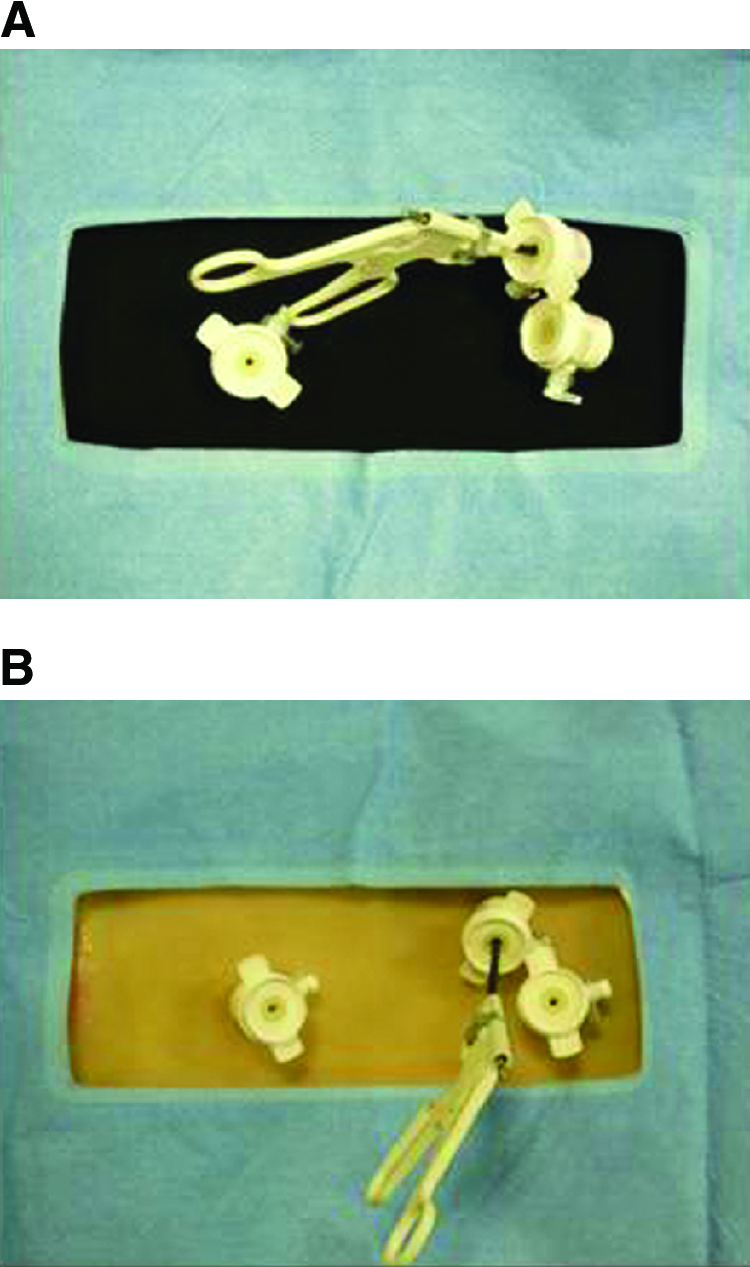
A body torso laparoscopic trainer (model BTS300D; Pharmabotics Ltd., Hampshire, UK), commonly known as a “box trainer,” is the shape of a human torso (Fig. 1A). The standard box trainer is white, but is also available in grey and transparent. The box trainer allows both animal and synthetic models to be placed inside the cavity (Fig. 2A). A piece of black-colored neoprene material covers the cavity and allows laparoscopic instruments to be placed through ports inserted into the neoprene material (Fig. 3A).

(
(
(
In an effort to enhance the realism of the abdominal cavity, the standard box trainer was modified from using inexpensive materials. Digital images of the abdominal cavity were captured from the Simbionix™ LAP Mentor™ (Simbionix, Cleveland, OH) during a laparoscopic cholecystectomy procedure. The “management” mode of the LAP Mentor was used so that the images were free from text captions, which assist the trainee by detailing the objectives of the task during training modules. The digital images were transferred and saved onto a memory stick. The images were then taken to a nonspecialized printing company, which modified the images to remove the simulated shadows that give the impression of the curvilinear shape of the abdominal cavity. The images were copied and pasted next to one another in order to obtain the required size. The images were then printed onto a laminated card (approximately 0.5 mm thick). In order to omit any reflections created by the light source of the laparoscopic camera, the laminated card was printed with a matte finish. Two laminated sheets of card, of sizes A0 (841 × 1189 mm) and A3 (297 × 420 mm), lined the bottom and sides of the box-trainer cavity. The total cost of printing was £90 (approximately $135). The flexible nature of the laminated card allows the card to be carefully placed in a curvilinear manner akin to the abdominal wall (see Fig. 1B. The card was attached to the box trainer by using nonspecialized double-sided tape. Like the standard box trainer, the laminated surface of the card allows animal and synthetic models to be placed inside the cavity without damaging the card, thus making the card reusable (Fig. 2B). Further, the laminated surface of the card allows the images to be wiped clean with a damp cloth, if soiled when using animal or synthetic models.
To further enhance the visual realism of the box trainer, the black-colored neoprene, which simulates the skin of the torso, was replaced with a low-cost silicone model (Fig. 3B). Like the black-colored neoprene, the silicone skin covers the abdominal cavity and allows surgical instruments to be placed through ports inserted into the skin (Fig. 4B). The silicone skin is visually realistic and is attached to the body torso laparoscopic trainer by using Velcro tape. The silicone skin costs approximately £300 ($450) and was designed and produced by a prosthetic designer. Again, however, it can be reused on multiple occasions. The total cost for increasing the realism of the body torso, using the methods described above, was approximately £390 ($585).
(
Results
Evaluation of model
Twenty surgeons (10 residents, 10 attending) carried out a simulated laparoscopic cholecystectomy by using a standard laparoscopic box trainer and also by using the “modified” box trainer. Following each simulated procedure, surgeons responded to the following question: The model used is a realistic representation of a real procedure. Surgeons responded on a 6-point Likert scale with clearly defined anchors (1 = strongly disagree, 6 = strongly agree). The standard box trainer received a mean rating of 3.6 (SD = 1.2), in comparison with the modified laparoscopic box trainer, which received a mean rating of 4.0 (SD = 0.9). The results suggest that the modified box trainer decreased the visual realism gap, as intended, between the model and a real procedure.
After completing the two simulated laparoscopic cholecystectomies, using the standard and modified box trainers, surgeons also participated in a brief interview to explore their thoughts and perceptions of the modified box trainer, specifically in comparison to the standard, unmodified box trainer. This methodology was employed to obtain a richer understanding of surgeons' opinions that went beyond simple quantitative scoring. Interviews were transcribed; a standardized, qualitative methodology was used to identify emergent themes. The following four quotes were extracted from the interview transcripts: 1) “[standard box trainers] are just black and white … it was mocked up quite nicely. … because you could see other stuff, so I think that's a definite improvement from before, it's more realistic, definitely” (surgeon 11); 2) “[the modified box trainer] was more realistic [in comparison to the standard box trainer] without just having the white walls, definitely” (surgeon 10); 3) “I think it's ([modified box trainer] a lot more realistic” (surgeon 9); and 4) “it looked good [modified box trainer], it was a lot more realistic because normally you can see the edges of it and the outsides or the insides. … so that was, it was well prepared definitely. So, I think that was good” (surgeon 2). Overall, surgeons reported that the modified box trainer was more realistic than the standard box trainer alone.
Discussion
The use of simulation in surgical education, training, and assessment is rapidly increasing. The chief medical officer in the UK has envisaged that simulation-based training will form a fundamental role in bridging the skills gap in the future. 1 Realism is an important element in creating an optimal training environment. A simple, inexpensive, yet effective, method to enhance the visual realism of a box trainer was described above.
The method discussed in this article is not intended to replace the use of VR simulators in surgical training. However, due to the considerable cost gap between VR simulators and physical trainers, the use of VR simulators in surgical training is limited to a relatively small number of centers. Widely available, physical trainers offer a low-cost alternative to VR simulators, yet they often lack visual realism. Realism is an important element in creating an effective training setting. 11 Thus, the goal should be to enhance the level of realism in simulation (i.e., minimize the gaps between the simulated and clinical environment) to a level that ensures that there are not too many gaps that are wide from reality. 11 Although there have been other examples in the literature of novel box trainers or home trainers,12,13 these rely upon developing a box trainer from the very beginning. This may require significant time and may not be the most economic approach. Conversely, the method described in this article can be used as an adjunct to increase the realism of box trainers that already exist—making this technique highly adaptable and less resource intensive. Further, not only did this method minimize the visual gap between a standard box trainer and real laparoscopic surgery, it was also found to be extremely effective by end-users.
The method described above is not without limitations. To replicate the method described, access to a VR simulator is required. However, we suggest that this limitation can be overcome by capturing digital images during a real surgical procedure. Also, although we only described the technique for a laparoscopic cholecystectomy, it can potentially be used to increase the realism of any intra-abdominal procedure. This technique could be incorporated into any surgical skills training course, such as the Basic Surgical Skills course in the UK or the Fundamentals of Laparoscopic Surgery (FLS) training program in the United States. Doing so would help create a more realistic environment that closely emulates surgical reality. This may facilitate the suspension of disbelief in a manner that maximizes simulation engagement and provides optimal learning outcomes.
Conclusions
A simple, inexpensive, yet effective, method of enhancing the visual realism of the widely accessible box trainer was developed. The model was evaluated from using both quantitative and qualitative methodologies. Results suggest that the method described above enhances the visual realism of the box trainer. It would thus be beneficial to incorporate this method in the training of laparoscopic skills.
Footnotes
Acknowledgments
This research was funded by the BUPA Foundation and the London Deanery STELi.
Disclosure Statement
No competing financial interests exist.