
Abstract
Abstract
Background and Aim:
The traditional management of open/laparoscopic choledochotomy after common bile duct (CBD) exploration is accomplished by placement of a T-tube, a procedure historically associated with complications and discomfort. In this study, we share in humble our laparoscopic experience of the use of primary closure of CBD, primary closure over pigtail J, and endonasobiliary drainage (ENBD) tubes as easy and effective alternatives to T-tubes.
Methods:
From April 2006 to March 2009, 27 (16 women) patients with CBD stones underwent laparoscopic choledochotomy at our institute and were engaged in this study by means of T-tube-free approach after bile duct exploration: primary closure, pigtail J tube, and ENBD tube groups. On admission, routine laboratory and imaging workups were performed to confirm choledocholithiasis diagnosis.
Results:
The mean operative time for primary closure, pigtail J tube, and ENBD tube groups were 95, 100, and 97.5 minutes, respectively. There was no conversion to open surgery nor was intraoperative complication experienced in all the groups. No major biliary complications such as bile leakage or bile peritonitis were seen; however, 1 patient from the pigtail J group experienced premature tube dislodgement and 1 patient from the ENBD tube group was found with a singular CBD retained stone.
Conclusions:
Laparoscopic primary closure of the CBD and over pigtail J and ENBD tubes are easy and effective alternatives to T-tube placements; these procedures are safe and with great feasibility, they offer faster recovery time for patients and early discharge with lower hospital charge.
Introduction
Materials and Methods
Patients
From April 2006 to March 2009, a total of 27 patients with choledocholithiasis underwent laparoscopic choledochotomy performed by a senior surgeon, S. D. Wu, MD, PhD. in the department of biliary and vascular surgery at Shengjing Hospital affiliated to China Medical University, Shenyang, China. The patient selection criteria for laparoscopic choledochotomy specified large single or multiple extrahepatic ductal stones and a CBD diameter >8 mm (Fig. 1). High-risk surgical candidates and those with CBD <8 mm were managed with endoscopic retrograde cholangiopancreatography (ERCP)/endoscopic sphincterotomy, as laparoscopic procedures were considered life-threatening.
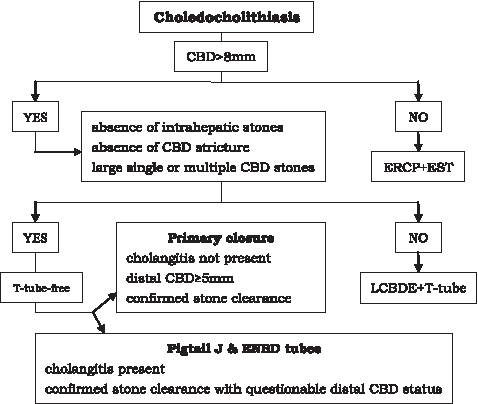
Flowchart of managements of choledocholithiasis. CBD, common bile duct; ERCP, endoscopic retrograde cholangiopancreatography; EST, endoscopic sphincterotomy; LCBDE, laparoscopic Common bile duct exploration.
All the patients presented with abdominal pain. Other complaints included jaundice, fever, and vomiting (Table 1). Choledocholithiasis was confirmed on magnetic resonance cholangiopancreatography, abdominal ultrasound (US), or computed tomography scan. All the 27 patients engaged in our study underwent the T-tube-free approach after bile duct exploration, of which 11 underwent primary closure of the CBD only, 12 had primary closure over pigtail J tubes, and 4 had closure over pre-installed ENBD tubes (Table 1). On admission, all the patients underwent routine laboratory and imaging assessment including blood counts, liver function tests (LFTs), magnetic resonance cholangiopancreatography, US, or computed tomography scan. LFTs were repeated on the third postoperative day for analytical comparison. Immediate preoperative imaging results (<24 hours to operation) suggested CBD dilatation (>8 mm) and stone existence (n ≥ 1) in all the patients with no instance of false positive imaging or error in estimation of CBD size; the mean CBD diameter was 13.30 ± 2.65 mm and the median number of CBD stones was 2.5 (range, 1–4) (Table 1). These results were later confirmed by the findings of ERCP or intraoperative choledochoscopic check.
CBD, common bile duct; ENBD, endonasobiliary drainage.
Operative techniques
Primary choledochorrhaphy approach
The procedure begins with laparoscopic cholecystectomy (LC) by the four-trocar technique and patients in a head-up, left-tilt supine position. With the 30-degree, 10-mm laparoscope at umbilical port, a further 10 mm subxiphoidal port is placed for introducing the choledochoscope and extraction devices. Two 5 mm ports are placed on the right upper quadrant 2 cm below the costal margin along the anterior axillary and mid-clavicular lines respectively.
Access into the CBD was through a supraduodenal longitudinal incision on the anterior wall of the CBD made with cutting electrocautery; suction irrigation was applied to maintain a clear view. Once the duct is opened, reachable stones are grasped and removed directly with Semm's spoon forceps. The flexible choledochoscope is then passed through the 10-mm subxiphoidal port to perform visual-guided extraction of further residual stones. When a stone had been located, a Dormia retrieval basket was used in conjunction with the flexible choledochoscope to extract the stone. Probing, especially around the terminal end of the bile duct, must be carried out gently to minimize unnecessary ductal spasm and edema. The stones were extracted from the peritoneal cavity in a specimen sac.
After all the stones had been removed, the biliary tract was irrigated with saline and a completion check choledochoscopy was performed for inspecting the distal and proximal portions of extrahepatic ducts to ensure clearance of residual stone fragments from the biliary tract. The CBD incision was closed in a single layer, using interrupted or continuous 3/0 absorbable atraumatic Vicryl suture(s) (Ethicon, Somerville, NJ), 2 mm apart. A peritoneal drain was inserted via the right subcostal 5 mm trocar along the anterior axillary line and placed in the hepatic space near the choledochotomy.
Pigtail J tube approach
The procedure begins with LC and CBD exploration by the four-trocar technique in the same fashion as described above. After all the stones are removed, choledochoscopic examination and stone extraction are performed to ensure stone clearance from the CBD. A guide wire is passed through the instrument channel and advanced through the ampulla of Vater into the duodenum, after which the scope is removed, leaving the guidewire in situ A pigtail J tube (HuaMei, Zhangjiagang City, Jiangsu, China) is then threaded along the guidewire into the CBD, through the ampulla of Vater and into the duodenum. With one end of the J tube in the duodenum, the guidewire is removed and the opposite end of the J tube is adequately fixed into the CBD (Fig. 2). A completion check choledochoscopy is performed to ensure exact positioning of the J tube before primary choledochorrhaphy with interrupted or continuous 3/0 absorbable Vicryl suture(s). A peritoneal drain is placed in the hepatic space near the choledochotomy in case of bile leak.
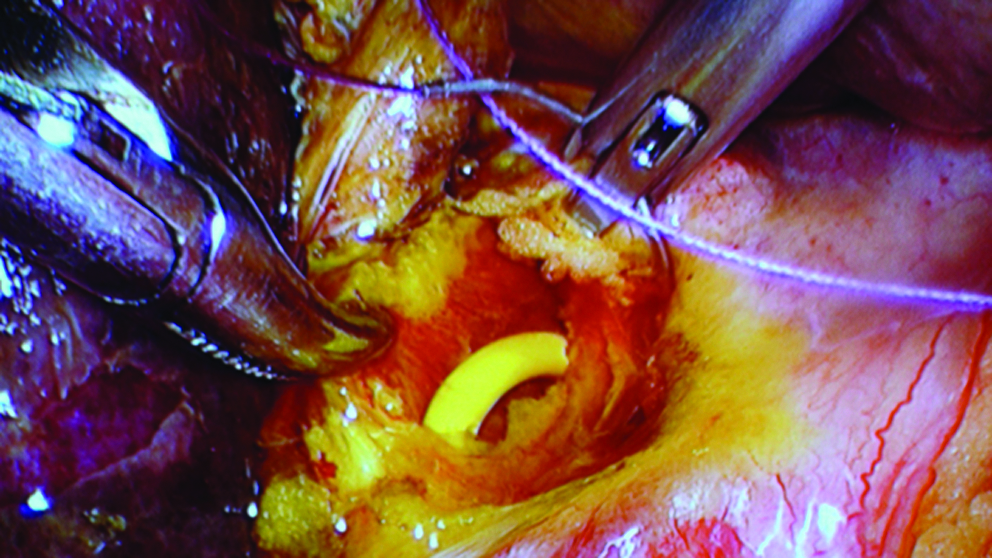
Intraoperative view of opened CBD containing pigtail J tube before choledochorrhaphy.
Postoperative abdominal X-ray is done to confirm the position of the pigtail J tube before the patient is discharged and the tube removed.
ENBD tube approach
All the patients in this group were subjected to preoperative ERCP and endoscopic sphincterotomy to confirm the diagnosis of choledocholithiasis (<6 hours to operation) and ensure the absence of strictures and stones of intrahepatic ducts. After failed attempts at stone retrieval by endoscopic measures, a 7 French ENBD tube (Cook, Winston-Salem, NC) was placed in the CBD of each patient followed by an ENBD cholangiography to confirm its position.
LC and bile duct exploration were accomplished by the four-trocar technique in the same fashion as described above. After all the stones have been removed, a completion check choledochoscopy was performed to ensure clearance of the biliary tract of any residual stones and accurate positioning of the ENBD tube in CBD. The choledochotomy closure was performed using interrupted or continuous 3/0 absorbable Vicryl suture(s). Saline was injected into the ENBD tube to observe any possible bile leak through closed sutures, and a peritoneal drain was placed in the hepatic space near the choledochotomy.
Before the ENBD tubes were removed, cholangiography was scheduled to verify the biliary tract was free of residual stones.
Results
About 27 (16 women and 11 men) patients with a mean age of 62.48 years, ranging between 27 and 84 years, underwent laparoscopic choledochotomy and exploration: primary closure (n = 11), pigtail J tube (n = 12), and ENBD tube (n = 4) groups (Table 1).
There were no conversions to open surgery nor did intraoperative complication occur in any of the groups; pigtail J and ENBD tubes were closed without any difficulties. The mean operative time for primary closure, J tube, and ENBD groups were 95 (range, 45–130), 100 (range, 55–160), and 97.5 (range, 55–150) minutes, respectively (Table 2). The peritoneal drains were placed in all the patients and commonly removed on postoperative day 3 if permitted, and pigtail J and ENBD tubes on postoperative day 14 after cholangiography or US have confirmed clearance of the biliary tract of any residual stones.
No major biliary complications such as bile leakage, bile peritonitis, and pancreatitis were seen in each group. However, abdominal X-ray of one patient from the pigtail J group revealed a premature displacement of the J tube into the ascending colon before its endoscopic removal, which was later safely excreted. Another complication experienced was the postoperative cholangiography discovery of a singular distal CBD residual stone in a patient from the ENBD group. From our past experience, retained stones are highly uncommon, especially after a completion check choledochoscopy. This complication was later resolved with routine endoscopic (ERCP) retrieval procedure (Table 2).
The postoperative day 3 leukocyte counts were slightly higher for patients in each group, which is not uncommon for patients after their surgery. Antibiotics were routinely administered to all the patients preoperatively and postoperatively for a total of 4–6 days. Almost all the postoperative LFTs values demonstrated trends of improvement when compared with the preoperative values. Postoperative bilirubin values for the ENBD group did not show improving trends possibly because of its small sample size.
The postoperative hospital stay for the three groups ranged from 3 to 7 days (Table 2). Patients experienced faster recovery time and there was no postoperative mortality/morbidity. Until now, no patients have returned with any biliary complications.
Discussion
CBD exploration is a standard procedure performed when stones are known to be present in the CBD or are found on intraoperative cholangiography. There is no single best approach for the management of CBD stones, and factors including surgical skills, experience of surgeons, and clinical status of patients should be taken into consideration.13,14 With the explosion of the use of minimally invasive surgery, laparoscopic choledochotomy and CBD exploration (LCBDE) in the laparoscopic era have profoundly diffused among surgeons.
At present, two laparoscopic methods are currently used for the removal of CBD stones: the transcystic duct exploration and exploration via a choledochotomy. The former is more appealing to some surgeons, because it is feasible in most patients and because it is a more minimal access solution to the CBD and does not require placement of a T-tube, which is consistent with the aims of a minimally invasive procedure. In conditions where intrahepatic stones, large stones, or acute angulated cystic duct preclude the use of the transcystic approach, 15 exploration via a choledochotomy permits direct CBD and intrahepatic routes and disregards the cystic anatomy and stone characteristics.
In an attempt to avoid the complications commonly seen with T-tube placement, several ductal drainage techniques have been performed in the management of CBD stones. Transcystic duct tube drainage (C-tube), for instance, 16 poses a similar mentality as that of the T-tube by allowing effective postoperative biliary drainage and cholangiography for possible residual stones. Nevertheless, complications including bile leakage and premature tube dislodgement are likely to occur as with the T-tube; C-tube withdrawal is permitted only with matured tract.
In this study, we share in humble our laparoscopic experience of the use of primary closure of CBD, primary closure over pigtail J, and ENBD tubes as easy and effective alternatives to T-tubes for the treatment of CBD stones. Primary closure after laparoscopic bile duct exploration has gained much attention and with favorable results. 17 Studies by Collins 18 and Krauss and Kern 19 on primary choledochorraphy have shown a significant reduction in complications or mortality and morbidity when compared with that of T-tube drainage. The primary closure approach does not necessarily lead to bile leakage; in our study, there was no bile leakage in the choledochorraphy group (Table 2) as with other investigators' reports.20,21 Gentle probing, especially around distal CBD, should be emphasized to prevent unnecessary ductal spasm and edema that may lead to elevated bile duct pressure. Primary choledochorraphy after laparoscopic bile duct exploration is safe and with shorter hospital stay, it is recommended by some, especially for hospitals with access to endoscopic measures (ERCP) that allow postoperative cholangiogram and stone extraction. 3
The criteria for laparoscopic primary choledochorraphy (distal CBD ≥5 mm or choledochoscope is able to pass along the distal CBD smoothly) are stricter than for other choledochotomies (Fig. 1); in Table 3, we provided recommended indications and contraindications for the procedure based on our experience. Circumstances with questionable distal CBD status should provide intraductal decompression means to prevent bile leakage from elevated ductal pressure through a choledochotomy. In so doing, without using T-tube drainage as an external drainage, we adopted primary choledochorraphy over a pigtail J tube drainage as an internal drainage that permits extrahepatic biliary decompression while avoiding excessive bile loss and many known complications. This drainage procedure is easy to perform and patients go “tube-free” for ∼2 weeks before its endoscopic removal. No major complications were seen in this group; however, abdominal X-ray before endoscopic J-tube removal for one patient revealed a tube displacement into the ascending colon (see Table 2) and later excreted safely; J-tube removal is independent of tract maturation. Perhaps, single-pigtail J tubes are a more appropriate option for assuring proper fixation within the CBD.
Absolute criteria for simple primary closure of the CBD.
For patients with difficult endoscopic stone retrievals, an ENBD tube was placed in the CBD of each patient before operative intervention. Laparoscopic primary choledochorraphy over ENBD tubes, similar to any intraductal drainage, allows decompression of the biliary tree and performs cholangiography at ease (pre- or postoperative) after placement. Bile flow alongside or entering the tubes reduces the possibility of excessive bile loss or increased intraductal pressure, respectively. The ENBD tubes were easily and safely placed in the CBD; patients found them tolerable and were instructed to prevent premature tube withdrawal and damage with maximum care. Removal of the ENBD tubes is also independent of tract maturation; tubes are generally removed after cholangiography confirmation of CBD stone clearance, approximately on postoperative day 14. In 1 patient, postoperative cholangiography revealed a singular distal CBD retained stone (Table 2), which was uncommon from our past experience, and later retrieved by endoscopic procedures. No major biliary complications were experienced by other patients.
To conclude, laparoscopic primary closure of the CBD and over pigtail J and ENBD tubes are easy and effective alternatives to T-tube placements; these procedures are safe and with great feasibility. Laparoscopic primary choledochorraphy is consistent with the aims of minimally invasive surgery, and its strict patient selection criteria sometimes hinder its diffusion. The introduction of pigtail J and ENBD tubes not only allowed primary choledochorraphy but also preserved the major uses of T-tubes, without the risk of bile leakage. Tract maturation is no longer a prerequisite for the removal of pigtail J and ENBD tubes; in rare cases of retained stone (1 in our study), endoscopic (ERCP) retrieval is routinely performed. These new approaches offered faster recovery time for patients and early discharge with lower hospital charge. However, larger sample size studies are recommended to confirm these findings before broad clinical application is anticipated.
Footnotes
Disclosure Statement
No competing financial interests exist.