
Abstract
Abstract
Background and Study Aims:
The success of natural orifice surgery depends on secure closure of the transmural gut opening, so a rapid, secure, and easy-to-place closure method is desirable. Our aim was to determine whether a gastrotomy can be closed safely and effectively from within the stomach in a survival model by using a novel, endoscopically placed device: the Padlock-G system.
Patients and Methods:
This was a pilot study of 4 survival animals in an animal laboratory setting. Gastrotomies were made in the stomachs of laboratory swine, and the abdomen was explored by using a standard gastroscope. Gastrotomies were then closed by using the Padlock-G system. Survival for 2 or 6 weeks was the primary outcome measurement. Secondary outcomes included ease of use, visual assessment of closure integrity immediately and at necropsy, presence of adhesions, evidence of infection, and histologic appearance at the closure sites.
Results:
All animals thrived, ate normally, and gained weight. None developed fever, tachycardia, or signs of peritoneal irritation. Closure-site inspection at necropsy revealed excellent healing, with epithelial growth over the Padlock-G. There were no ulcers, serosal surfaces were tightly closed, and no defects could be seen. There were no signs of peritoneal inflammation, intra-abdominal adhesions, or gastric spillage. Histologic evaluation showed organizing granulation tissue with fibrosis, vascular proliferation, and mild chronic inflammatory infiltrate (i.e., scar).
Conclusions:
The Padlock-G is easy to place, provides a durable closure, and allows survival animals to thrive without adverse sequellae. This device provides a suitable closure system for transgastric NOTES.
Introduction
Materials and Methods
The Lock-It System® (Aponos Medical, Kingston, NH) comprises the Padlock-G, a Nitinol clip that is 18 mm in diameter and 0.76 mm thick (Fig. 1), as well as a scope-mounted delivery pod (Fig. 2). The Padlock-G is folded to fit into the pod but springs back into its original shape when deployed. This locking device is six-sided and has six inner prongs that embed into the gastric wall around the gastrotomy site. When the device is deployed and snaps back into its original flat or disc-like shape, these six prongs gather the edges of the gastrotomy into a secure, watertight bundle, thus sealing the gastrotomy (Fig. 3).
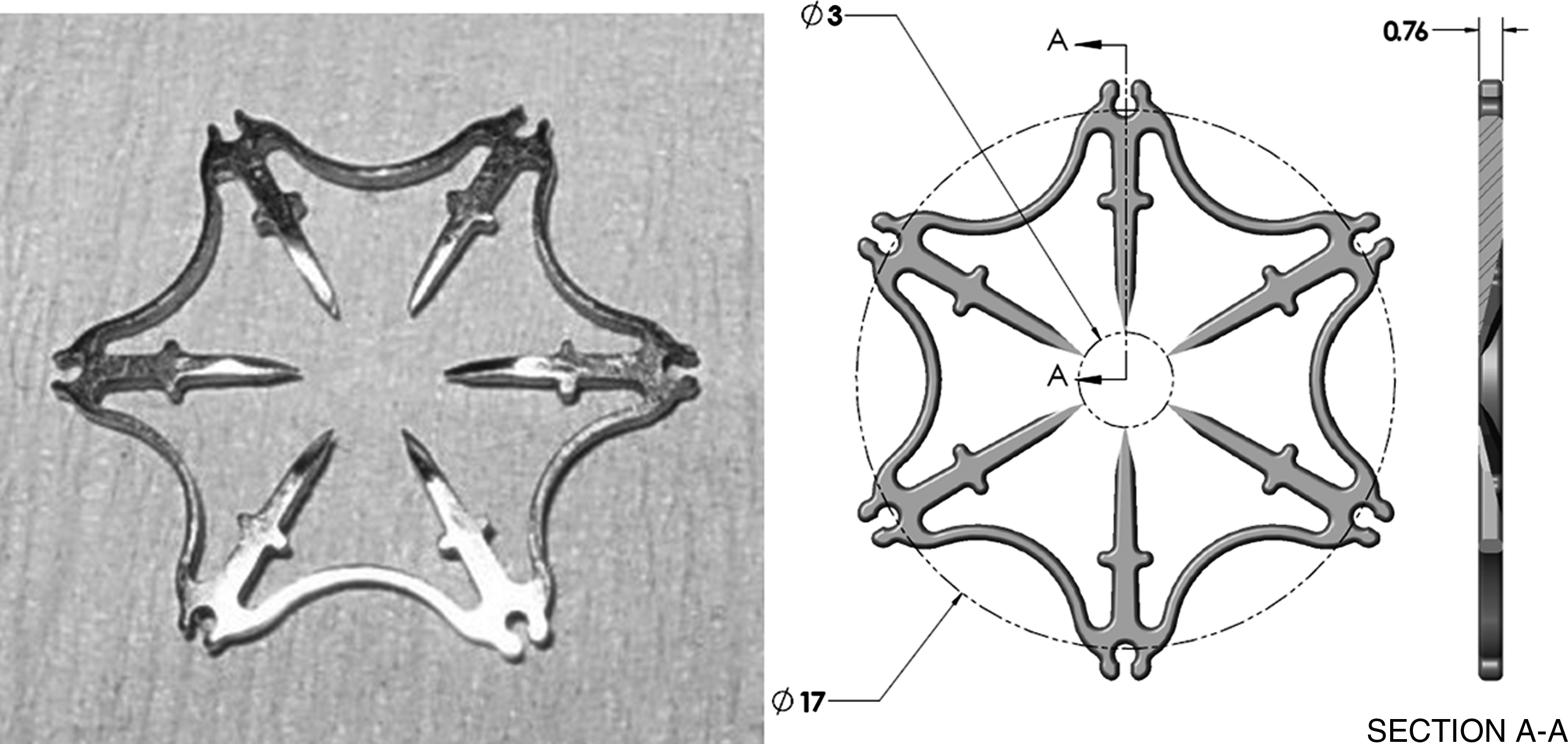
The Padlock-G. The outer circle in the computer drawing is 18 mm in diameter.

Two versions of the Lock-It system. (
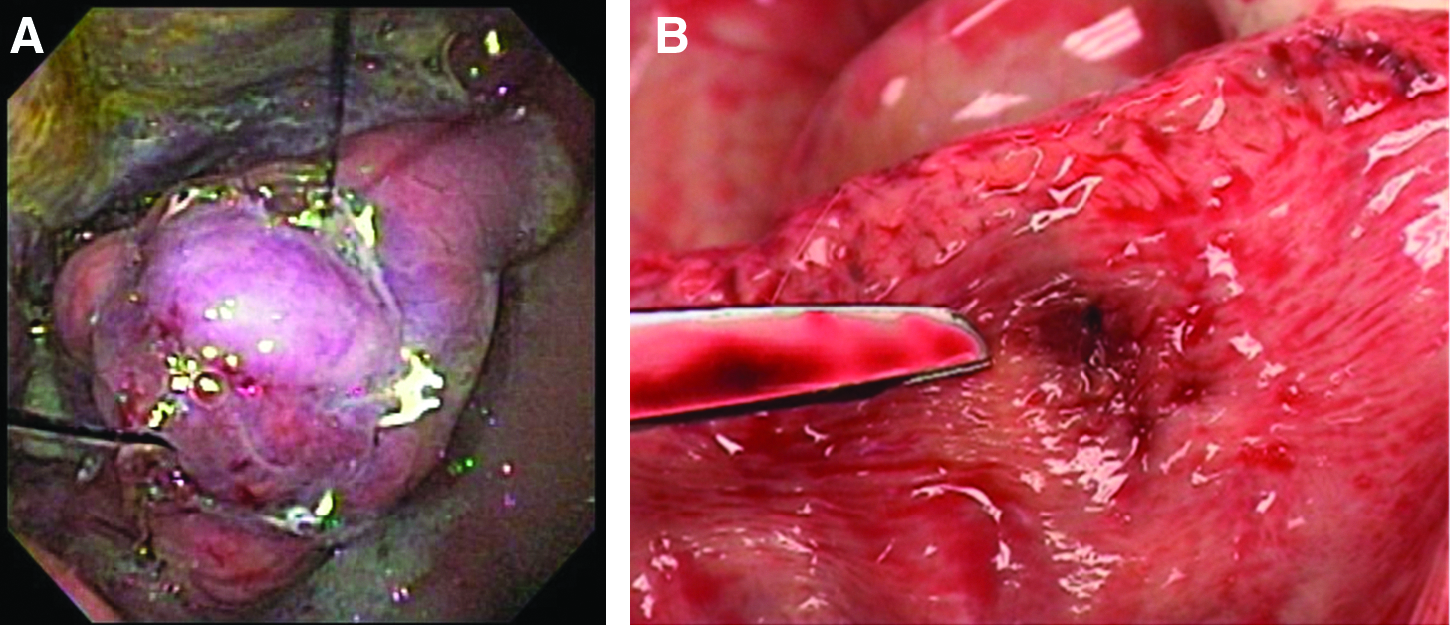
Appearance immediately after deployment of the Padlock-G. (
All animals were treated humanely according to United States Department of Agriculture (USDA) guidelines. The work was done according to a protocol approved by the Baystate Medical Center (Springfield, MA) Institutional Animal Care and Use Committee. Procedures were performed in a clean operating theater intended for sterile procedures with survival of the experimental subject, according to USDA guidelines and regulations. Four 30- to 35-kg laboratory swine were fasted overnight and then anesthetized with an intramuscular cocktail of ketamine, xylazine, and Telazol, followed by isofluorane anesthesia with endotracheal intubation. No paralytic agents were given. Gastroscopes were disinfected by using a standard reprocessing regimen with glutaraldehyde. Further disinfection was performed by soaking the endoscopes for 5–10 minutes in Betadine solution at 1:10 dilution, and this solution was injected into, and aspirated from, the working channel. Sterile water was used in the reservoir used for lens washing.
All 4 animals were treated in the same way. Each animal was treated preoperatively with penicillin G (1 cc per 20 kg body weight). They were then placed in the supine position on the operating table and secured with rope ties. The mouth and oropharynx were sprayed with a solution of Betadine at 1:10 dilution. A previously disinfected, double-channel, therapeutic gastroscope (TGF-130; Olympus America, Center Valley, PA) was inserted into the oral cavity, and additional application of Betadine was done to visibly untreated areas of the oropharynx by injecting forcefully down the endoscopic channels under endoscopic vision. The esophagus and stomach were similarly treated. For the first 2 animals, a gastric overtube was used (U.S. Endoscopy, Mentor, OH). We subsequently dispensed with the overtube, having learned that the scope-mounted pod could be inserted directly into the esophagus endoscopically, analogous to placement of an endoscope-mounted band ligator. Five hundred milliliters of diluted Betadine solution were injected into the stomach and allowed to remain for 1 minute, while the animal was rocked from side to side to ensure even coating and complete treatment of the mucosa. As much residual debris and sawdust bedding as possible was then aspirated from the stomach, along with the excess Betadine solution.
Gastrotomy was performed by the so-called percutaneous endoscopic gastrostomy (PEG) technique, similar to the placement of a PEG. 2 After sterile prep of the abdomen with Betadine, an 18-G spinal needle was inserted aseptically into the abdomen under endoscopic vision. A 0.035-in Teflon-coated guidewire (Tracer Metro; Cook Medical, Winston-Salem, NC) was inserted into the stomach through the needle and brought out through the right scope channel (Fig. 4). An additional area on the abdominal wall was sterilely prepped, and a Veress needle was then inserted into the abdomen. The pneumoperitoneum was then initiated with carbon dioxide (CO2) to a pressure of 12 mm Hg.

Sequential placement of guidewire, T-bags, and then balloon dilation of gastrotomy. T-bags are placed on opposite sides of the gastrotomy site to facilitate prolapse of gastric wall into the deployment pod.
The left scope channel was then used to place two endoscopic T-tags (Cook Medical) transmurally in the stomach by standard techniques. That is, a 19-G endoscopic needle loaded with a T-tag on a 2-0 nylon suture was used to puncture the gastric wall near the guidewire, and the T-tag was deployed through the stomach wall into the abdomen. The fact that the wire was inserted on the anterior portion of the stomach during PEG-type placement, and the fact that there was now the pneumoperitoneum lifting the abdominal wall away from the stomach, ensured that there was a lower risk of puncturing other viscera, a solid organ, or the abdominal wall during T-tag placement. A second T-tag was placed in an identical fashion on the opposite side of the guidewire (Fig. 4). Excess guidewire was then coiled deeply in the abdomen by pushing it through the skin puncture site.
A wire-guided, 12-mm endoscopic dilation balloon (Cook Medical) was then passed over the guidewire, still in the right scope channel, and passed through the needle tract in the gastric wall. The balloon was positioned across the gastric wall and inflated for 1 minute to 12 mm in diameter, creating a 12-mm gastrotomy (Fig. 4). The balloon was deflated and removed. Leaving the wire in place, the therapeutic gastroscope was removed. A diagnostic gastroscope with a diameter of 9.5 mm (GIF-140; Olympus America) was then passed alongside the guidewire or, in some cases, over the guidewire, and we explored the abdomen endoscopically. The guidewire was then removed.
The Padlock-G was then loaded into its deployment pod. The loaded pod was mounted on the tip of the diagnostic gastroscope with a friction-fit adaptor, and the sutures were brought out through the working channel with a snare. The endoscope with attached deployment pod was then reintroduced over the sutures until the pod was abutting the gastrotomy. The sutures attached to the extramural T-tags were then used to pull the edges of the gastrotomy physically into the deployment pod under endoscopic vision. Suction was applied to assist with prolapsing as much gastric wall into the pod as possible. The Padlock-G was then deployed from the pod by retracting the inner sheath of the pod, using the attached tripwire. The Padlock-G, once deployed immediately resumed its original shape, entrapping the gastric wall layers on its six prongs, and effectively sealing the gastrotomy (Fig. 3A). The T-tag sutures were then cut short with endoscopic scissors, the endoscope was withdrawn, and the procedure was terminated.
The first 2 animals were survived for 2 weeks prior to necropsy. The second 2 animals were survived for 6 weeks. At necropsy gross examination of the abdominal cavity and of the closure sites, both on the mucosal and serosal sides, was performed. The closure sites were then excised for microscopic evaluation.
Results
All animals thrived, ate normally, and gained weight. The 2-week survivors gained 2.8 kg each, while the 6-week survivors more than doubled in weight (>35 kg). None of the animals developed fever, tachycardia, or signs of peritoneal irritation. The stomachs were harvested, and inspection of the closure sites revealed excellent healing with epithelial growth over the Padlock-G (Fig. 5). There were no ulcers, serosal surfaces were tightly closed, and no defects could be seen. There were no signs of peritoneal inflammation, intra-abdominal adhesions, or gastric spillage. There were localized serosal adhesions and adherent omentum at the closure sites involving the T-tags, but not the Padlock-Gs, which were on the mucosal side. Histologic evaluation showed organizing granulation tissue with fibrosis, vascular proliferation, and mild chronic inflammatory infiltrate (i.e., scar). Acute inflammatory infiltrate was not seen (Fig. 6).
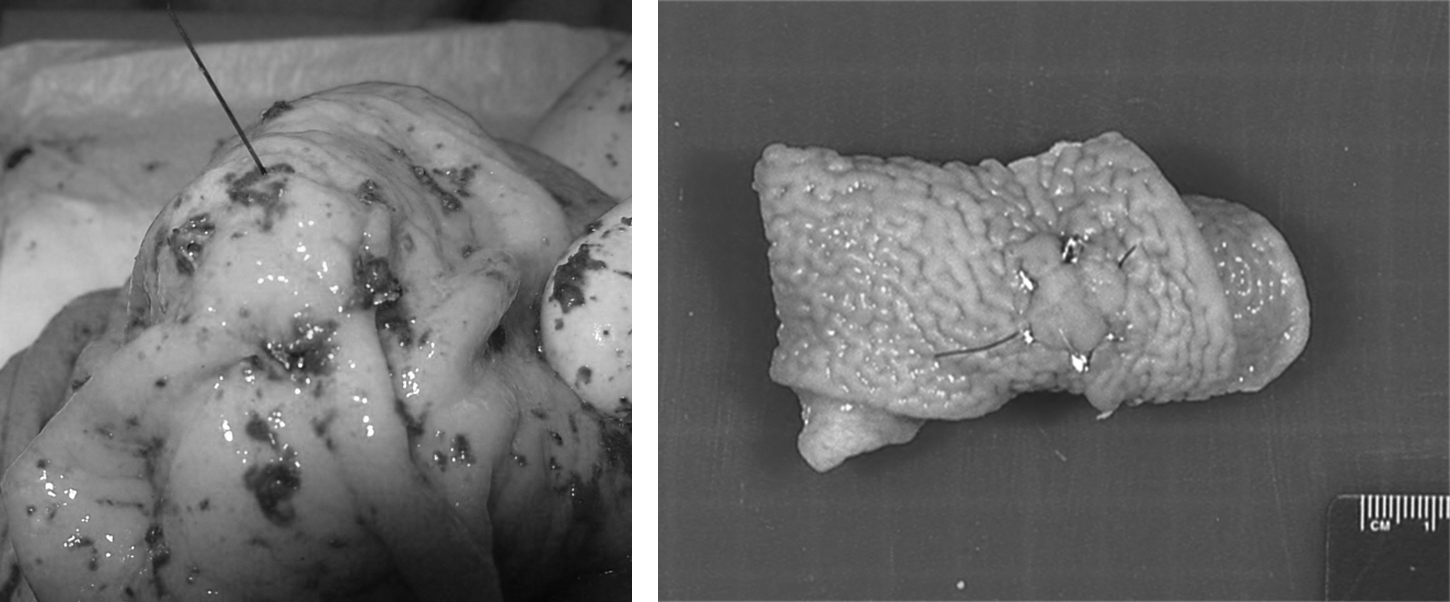
Appearance of the Padlock-G at necropsy and after tissue fixation. This is from one of the 2-week survival animals.
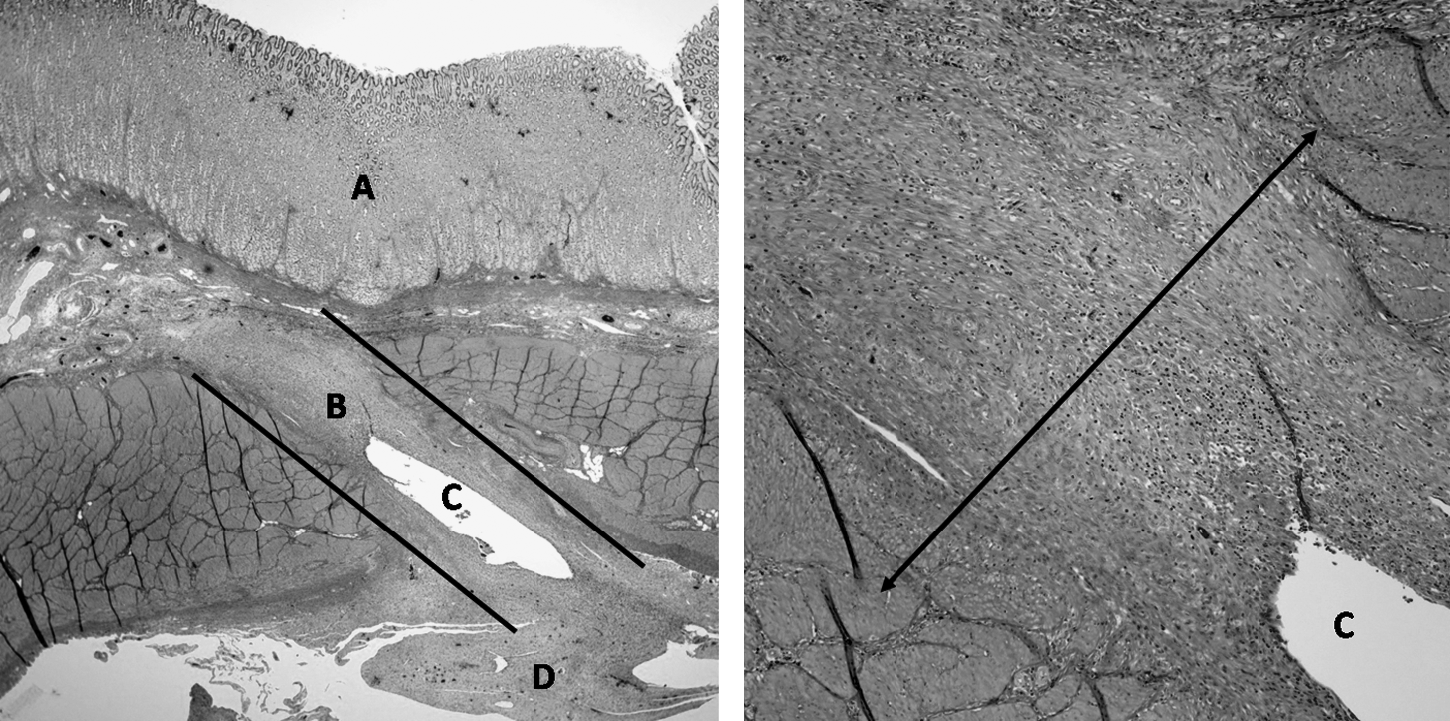
On left: low-power image of closure at 6 weeks. (
Discussion
Although one group has reported a successful porcine survival study where the gastrotomy was left open, 3 few would be willing to perform this experiment in humans. It is common practice in experimental animals to close the enterotomy by using endoscopic clips,4–8 but this is technically difficult, expensive, and does not guarantee a secure closure. Other closure methods include tissue anchors and looped T-anchors,9–11 suturing techniques, 12 self-approximating tissue flaps,13,14 and even deployment of a cardiac septal occluder, 15 among others. However, these can be time-consuming or difficult to place (mucosal flaps, endoscopic sutures), can potentially lead to unintended damage to other organs on the opposite side of the gastric wall (T-tags), or are expensive (cardiac septal occluder). A cheaper, faster, more reliable, and secure closure method is needed before transgastric NOTES procedures will be ready for widespread adoption.
The specific aim of this study was to determine whether a gastrotomy can be closed effectively from within the stomach by using a novel, endoscopically placed device: the Padlock-G system. This device relies on the shape-memory alloy properties of Nitinol to gather up the tissue around the gastrotomy and pinch it firmly together into a watertight bundle. Explant data reveal that after gastrotomy closure with the Padlock-G, burst pressures in explanted stomachs average 68 mm Hg. 1 At these pressures the inflated stomachs are tightly stretched and are twice their normal capacity or larger. Internal gastric pressures of this magnitude are unlikely to be generated in vivo, and the Padlock-G should maintain integrity of the gastric wall. We have confirmed this by means of this survival study.
It would have been very informative to burst test the stomachs from this experiment after a 2- or 6-week survival. However, we wanted to be certain to obtain histologic data in each case, so burst testing could not be done. Also, in order to obtain meaningful data, several such burst tests would need to have been done. This is perhaps an experiment that can be performed in the future if sufficient funding is available. One criticism of the experiment is the technique utilized to create the gastrotomy. We chose balloon dilatation, rather than needle knife cautery, to open the stomach wall, as we have observed a higher risk of bleeding with the needle knife. Also, we have found that needle knife cautery makes the gastrotomy irregularly shaped and thus harder to close.
In this study, we used the PEG technique to prevent inadvertent T-tag insertion into nearby solid organs or viscera. Exiting the stomach on its anterior surface and then generating the pneumoperitoneum ensures a dome of CO2 over the anterior stomach, such that needle puncture and placement of T-tags has a lower likelihood of misplacement of T-tags. Despite this, in 1 animal, a T-tag was still found to be embedded in the anterior abdominal wall upon endoscopic exploration of the abdomen. This tag was removed with endoscopic forceps, and a new tag was placed in the proper position alongside the gastrotomy. We had no inadvertent organ punctures in this study, as determined during abdominal exploration and also at necropsy.
Examination of the stomachs at necropsy showed that the T-tags could be a nidus for adhesion formation, although there were no abscesses or other evidence of infection. There is still a theoretic risk of inadvertent organ puncture, and, indeed, this occurred on some of our nonsurvival studies. We have subsequently determined that a satisfactory closure can be achieved by pulling the edge of the gastrotomy into the pod by using rat-toothed forceps with either a single-channel gastroscope or by using two such forceps and a double-channel scope. Closure in this fashion would be expected to eliminate the risk of errant T-tag puncture, adhesion formation, and so on.
Finally, it appeared, on the 6-week survivors, that the Padlock-G tends to migrate along the surface of the mucosa toward the antrum/pylorus as it slowly sloughs or rises to the surface. Indeed, in these animals, the Padlock-G was found 3–4 cm away from the closure site, which was covered with normal-appearing mucosa and which would be unrecognizable were it not for the two nylon sutures marking the spot. It is unclear if it will slough before reaching the pylorus, and, of course, this will depend on where it is placed. Considering that the Padlock-G is about the same size and thickness as a U.S. dime (i.e., 10-cent coin), and since these pass readily through the gastrointestinal tract in children and adults, we theorize that the Padlock-G should pass spontaneously once it sloughs from the inner surface of the stomach. This is also to be a subject of future research.
Conclusions
In summary, transgastric NOTES will depend on being able to enter and leave the abdominal cavity through the stomach, and therefore closure of the gastric opening is of paramount importance. Much of the published data involve gastric closure from using endoscopic clips or T-tags. Disadvantages of these approaches include the cost of numerous endoscopic clips, the technical difficulties of trying to close a hole from inside the stomach, and the potentially poor mechanical strength of these closures. By using the the Lock-It System and the Padlock-G, we have demonstrated that effective, durable gastrotomy closure can be achieved. The method is relatively fast, simple, and reproducible.
Footnotes
Acknowledgments
Aponos Medical funded the animal labs for this study and provided the Padlock-G System for our use. Cook Medical provided engineer support and some laboratory supplies in support of this project. Olympus America donated the endoscopes and endoscopic towers used in this study. The authors received no salary support from Cook, Olympus, or Aponos Medical, have no stock or other interests in these companies, and have no other disclosures related to this article.
Disclosure Statement
No competing financial interests exist.