
Abstract
Abstract
Whereas the majority of foreign bodies are managed endoscopically, complex objects, or those associated with significant injury, may require open removal. However, with the advent of newer, minimally invasive techniques, these objects can be successfully removed by using laparoscopic instruments. In this article, we describe our experience of using a single 5-mm laparoscopic port under pneumovesicum for removal of a knotted electric wire measuring 149 cm in length, with minimal invasiveness and avoidance of urethral injury. Using a cystoscope as the optical device through the urethra, a port can be introduced suprapubically. After insufflations of carbon dioxide at 12 mm Hg, the knotted electric cables were fragmented into several parts by laparoscopic scissor, then these parts were removed one by one. The optimal removal technique is dictated primarily by the nature of the foreign body. This case presents the feasibility of the pneumovesicum method in using a single laparoscopic port in cases of long, complex objects in the adult bladder.
Introduction
Case Report
A 20-year-old male presented to the emergency department of our institute with urethral bleeding and pain in the urethra and suprapubic region for a few hours following the insertion of a foreign body through his urethra. The patient reported that he had been inserting an electric cable through his urethra to gain sexual gratification for the past 3 months. Following masturbation, he would pull the cable out. However, in his most recent attempt, he was unable to remove the cable, and successive attempts resulted in detachment of the cable at a connecting point. Physical examination showed no abnormality on his external genitalia, other than meatal bleeding. However, a radiograph of the pelvis revealed a long foreign object (Fig. 1). As an initial attempt to remove the cable, cystoscopy was performed with the aid of local anesthetic gel. Once the presence of the electric cable was visually confirmed, it became apparent that the length and rigidity of the cable itself precluded the possibility of a urethral delivery. A cautious attempt to find the tip of the cable by cystoscopic forceps for removal through the urethra only ended with further entanglement, and a change of direction was inevitable.

A simple radiograph of the pelvis shows a long, kinking material in the pelvic cavity.
Under general anesthesia, the patient was placed in the lithotomic position, and a cystoscope was passed into the bladder. The urinary bladder was irrigated with normal saline for exudates and debris. The bladder was distended with normal saline; then, a 5-mm laparoscopic port was inserted through a small suprapubic incision (Fig. 2A). Safe entry of the trocar into the bladder was confirmed visually by cystoscope. Normal saline was then drained through the cystoscope, and the bladder was insufflated with carbon dioxide at a pressure of 12 mm Hg, which was supplied by the entry plug of the cystoscope (Fig. 3), to induce the pneumovesicum. A laparoscopic scissor was inserted through the 5-mm laparoscopic port, cutting the electric cable into several parts (Fig. 2B). The tying point of the cable was also amputated (Fig. 2C). These parts were removed one by one, using laparoscopic grasping forceps, constantly maintaining vision via the cystoscope (Fig. 2D). The removed foreign body consisted of a white electric cable measuring 102 cm and a black electric cable measuring 47 cm in length; each part was connected with yellow plastic tape (Fig. 4). Following a single stitch to the skin with 3-0 Nylon, a 5-mm port was removed, and a 16-Fr Foley catheter was inserted through the urethra. Drains were not inserted. Total operative time was 21 minutes, and the patient was discharged 1 day after surgery. A Foley catheter was removed 2 days after surgery at the outpatient department. One month after removal of the foreign body, the patient had no complaint concerning voiding.
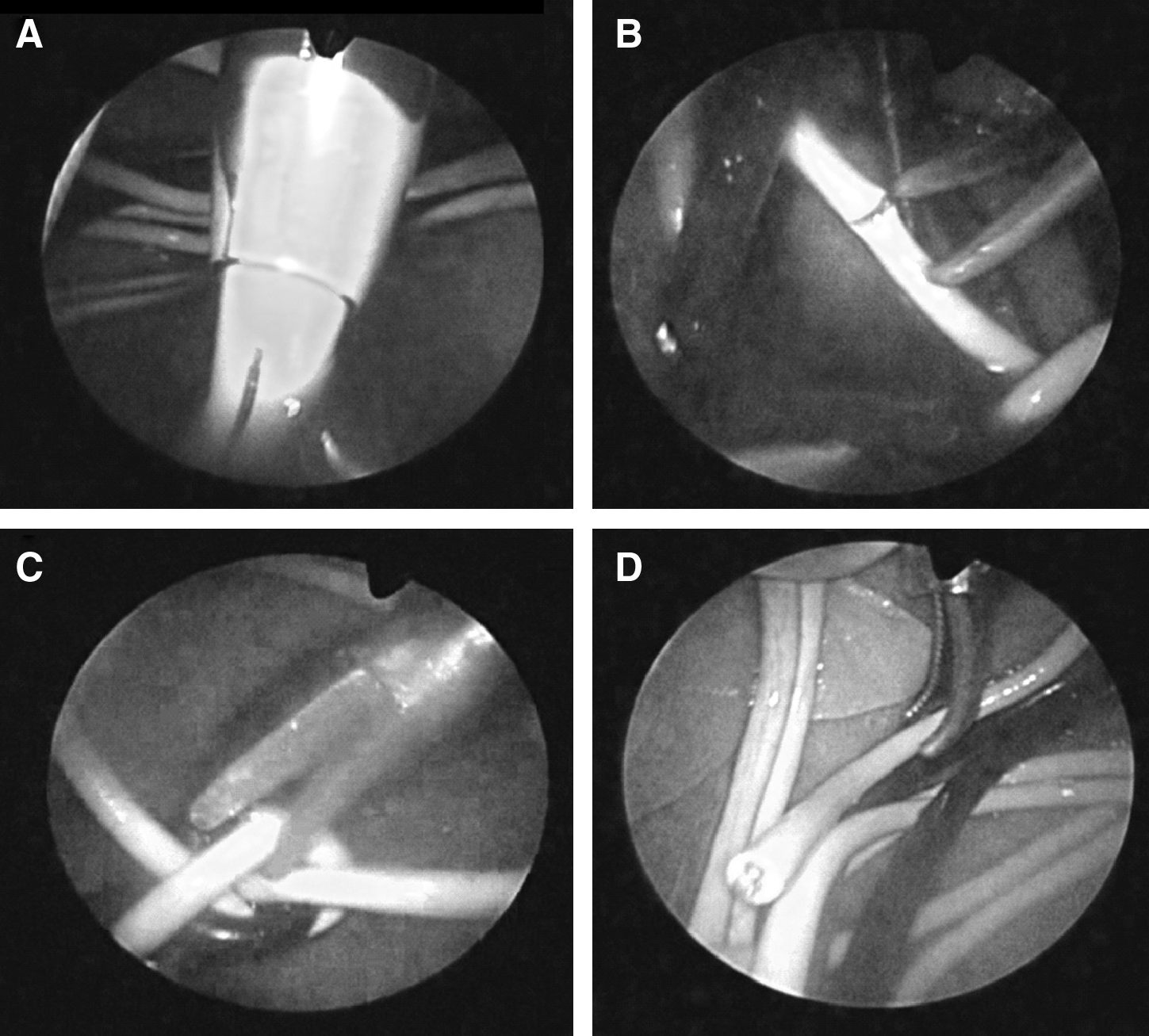
Operative process under cystoscopic vision. (

Trocar and cystoscope configuration. The line connected to the right side of the cystoscope plug supplies carbon dioxide (open), and the line connected to the left side of the cystoscope plug supplies normal saline (closed).
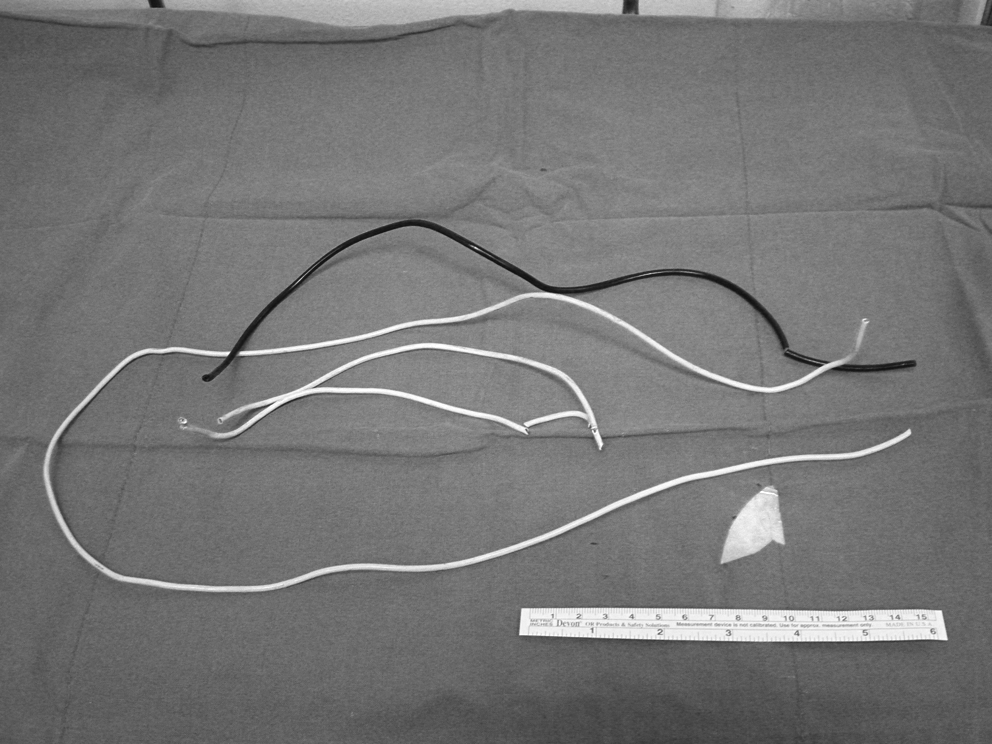
Removed electronic cable.
Discussion
Presence of a foreign body in the genitourinary tract often requires prompt intervention. 4 Definitive management of intravesical foreign bodies is aimed at providing complete removal of the foreign body with minimal complication. Various methods of removal have been described, including meatotomy, cystoscopy, internal or external urethrotomy, suprapubic cystostomy, Fogarty catheterization, and injection of solvents. 2 On rare occasions, the object may be spontaneously expelled from the bladder during urination. 5 But conventionally, with the aid of grasping forceps and retrieval baskets, most foreign bodies may be removed, either completely or after fragmentation, by using a cystoscopic approach. However, in some cases, grasping an object with alligator or calculus forceps increases the effective diameter of that object and may make removal difficult and hazardous.
Removal of electronic cable or flexible metal wire is challenging, due to its semirigid pliability and smooth surface disallowing a firm grasp by forceps. Further, due to its length and the contractions of the bladder, the wire tends to twine and entangle upon itself at the time of presentation or endoscopic manipulation. Thus, various approaches have been suggested. In a summary describing 16 cases involving removal of various foreign bodies, Rafique reported on 2 cases of metal wire removal in a 14-year-old female and a 25-year-old male, which were both conducted by open cystostomy to minimize urethral trauma. 3 Trehan et al. reported on the successful removal of a knotted telephone cable through the urethra, using plenty of local anesthetic gel and gentle traction from the urethra in a 55-year-old male. 6 Ejstrud and Poulsen used three laparoscopic ports—one 10 mm and two 5 mm—to visualize and untie a knotted intravesical cable in a 66-year-old male. Using directed vision, the knot was untied, and the electric cable was removed. 7 Modifying this technique, Eradi and Shenoy reported the laparoscopic extraction of a knotted electronic cable in a 14-year-old male. Under cytoscopic visualization, a 10-mm laparoscopic port was introduced via a suprapubic incision into a saline-distended bladder. Instead of manipulation under the cystoscope, the knotted electric cable was then grasped by using a laparoscopic grasper and delivered with the suprapubic incision en masse with the port. 8
The pneumovesicum method was initially described by Gill et al., during laparoscopic ureteroneocystostomy. 9 As reported by Reddy and Daniel, this technique was also applied for removal of bladder foreign bodies. Though a single 10-mm port insufflated with 12 mm Hg of carbon dioxide, they crashed Blu-Tack, a puttylike substance, then removed it from the bladder of a 14-year-old boy. 10 We adapted this method for removal of the long object. Because the electric cable was extremely long and tied up during the initial trial with cystoscopic removal, we fragmented the whole cable into several removable pieces in order to facilitate removal though a single port. To minimize the incision, a single 5-mm port was chosen in this case. Under the pneumovesicum, the entire removal process can be achieved with clear vision and distance from the urothelium, avoiding injury or bleeding of bladder mucosa within a short operative time. The optimal technique is dictated by the patient's condition, associated urinary tract injury, and size, and, primarily, the shape and nature of the foreign body. 3 Thus, an individualized method with consideration for each circumstance will provide the most suitable approach. In this regard, our case presents the feasibility and efficacy of the pneumovesicum method in using a single laparoscopic port inserted suprapubically in cases of long, complex objects in the adult bladder.
Footnotes
Disclosure Statement
No competing financial interests exist.