
Abstract
Abstract
Objective:
The aim of this study was to compare single versus multiple laparoscopic myomectomy with an intracapsular method.
Study Design:
A total of 335 laparoscopic intracapsular myomectomies were compared. They were subdivided into two groups. Group I included 195 patients with myoma; group II, 140 patients with multiple myomas, 4–9 cm in diameter. Laparoscopic procedures were compared with respect to intraoperative complications, postoperative compliance, and general surgical feedback. Results were analyzed using SAS software (version 8), considering a P-value of <0.05 as significant.
Results:
No differences (P > 0.05) between groups were observed with respect to the following: intraoperative blood loss (98 ± 4.7 mL of group I versus 106 ± 6.8 mL of group II), catheter inside pelvis for postsurgical drainage (40% versus 36.4% women), analgesic administration for the first 24 hours (41.5% versus 40% patients), postoperative fever after 24 hours (11.2% versus 9.2% women), postoperative therapeutic antibiotics administration (8.2% versus 6.4% patients), and hospitalization and postoperative ultrasound (US) intramyometrial hematoma detection (6.6% versus 5.7% of group II). The only surgical statistical difference (P < 0.05) was in the mean total laparoscopic time (60 ± 7.2 minutes for group I versus 97 ± 8.9 minutes for group II).
Conclusions:
Intracapsular laparoscopic myomectomies, performed in the same session on a single or on multiple fibroids, seem to preserve myometrial integrity and allow the restoration of uterine scar, with few early and late surgical complications.
Introduction
Among the therapeutic options, surgical myomectomy is the most common, performed by either laparotomy or laparoscopy. 2 In cases where reconstructing and preserving the organ is the primary goal, the choice of surgical technique appears to be pivotal, because long-term complications such as uterine rupture during pregnancy or labor occur in 2.4 of 1000 cases after myomectomy, compared with 0.5 of 1000 in controls. 3
Several studies have evaluated surgical approaches to myomectomy; some support the possibility of removing the myoma within its surrounding structure—the so-called “pseudocapsule”—by stretching and dissecting the surrounding fibromuscular skeleton to extract the myoma. This has been associated with decreased blood loss and less trauma to the healthy myometrium. 4
Many scientific investigations support “a structural architecture of the myomatic pseudocapsule,” that is, it was demonstrated how a complex network of fibers and vessels generally surrounds the myoma and separates it from normal uterine tissue. 4 Further support is given by microstructural studies demonstrating that the myoma is anchored to the pseudocapsule by connective bridges but lacks a proper vascular pedicle. 5
In myomectomy, this vascular network makes detaching the myoma inside the pseudocapsule easier, with reduced bleeding during the procedure. 6 This was also confirmed by Fox and Buckley and Vizza and Motta, who investigated a series of enucleated myomas with ultrastructural microscopy and found a separate anatomical structure. Compressed and partly vascularized fibromuscular tissues, different from the normal myometrium,7,8 were visible through ultrasonography as an echogenic line around the myoma (Fig. 1).9–11
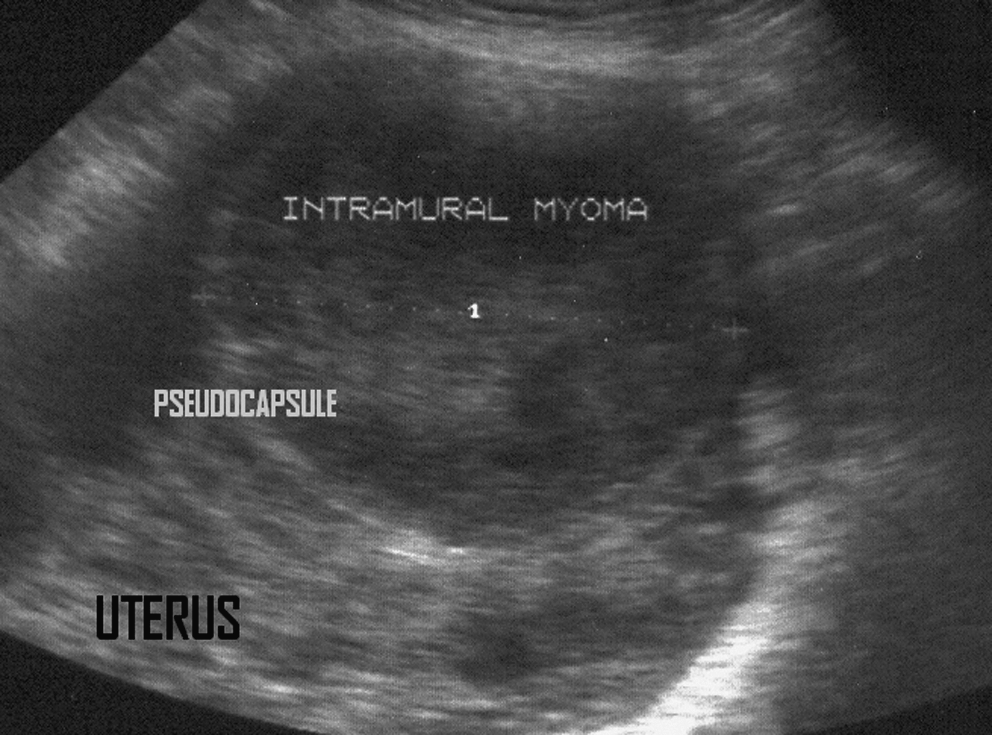
Ultrasonographic transvaginal transverse section of a uterus with intramural myoma: myoma pseudocapsule is highlighted in the myometrium by a hyperechogenic ring.
On the basis of these findings and practical experience, 4 surgically removing fibroids while respecting their surrounding structure, the pseudocapsule, has become popular amongst some gynecological surgeons and can be referred to as “intracapsular myomectomy.”4,12
It makes it possible to preserve myometrial integrity and allows restoration of the uterine scar. When performed by laparoscopy, it could be a safe, minimally invasive procedure for surgical removal of single or multiple fibroids in the same session. 4
On the basis of these findings, the articles referred to above, and their surgical experience, the authors planned this study to design a new surgical technique that minimizes postsurgical complications and optimizes the surgical outcome of single versus multiple laparoscopic intracapsular myomectomy in patients with fibroids.
The authors performed an institutional nonrandomized prospective investigation, evaluating the surgical outcome of single versus multiple laparoscopic intracapsular myomectomy, in terms of intraoperative complications, postoperative compliance, and general surgical feedback.
Patients and Methods
From January 2002 to September 2007, 335 women, with a mean age of 35.2 years, underwent single or multiple intracapsular laparoscopic myomectomy in multiple gynecological centers; 62 of these patients had undergone a previous cesarean section (18.7%).
All patients signed an informed consent prior to inclusion in this study, as approved by the local institutional research ethics committee.
The selected patients requested myomectomy for the following associated symptoms: pelvic pain, menorrhagia, and growth of myomatic nodules, verified by ultrasound, with increasing symptoms.
A few requested myomectomy in view of a future pregnancy. Exclusion criteria for the investigation were as follows: previous uterine surgery (excluding cesarean section), presurgical treatment with GnRH analogs, history of gynecological malignancy, and primary subfertility.
Exclusion criteria for preoperative GnRH analog treatment was due to reported increased risk of recurrence, a possible delay in the diagnosis of leiomyosarcoma, a risk of massive hemorrhage from degeneration, a greater difficulty in finding the cleavage plane, and a greater extent of hyalinization phenomena.13,14
All fibroids were selected through standardized transvaginal ultrasound myoma mapping; all patients had subserous and/or intramural fibroids and transvaginal ultrasound dates were recorded for postsurgical evaluation.
In the preliminary study setup, clinicians selected all women who had 3–6 myomas as patients to be submitted to multiple myomectomy.
In the study setting, the myomas' sizes before laparoscopy were between 4 and 9 cm; the 3–9 cm limit was selected by surgeons to avoid longer operation time and pointless uterine trauma for smaller fibroids.
To give homogeneity to the intracapsular laparoscopical myomectomy, the authors excluded pedunculated, cervical, and intraligamentary myomas, because they are extra myometrium.
Patients were first subdivided into two nonrandomized groups: 195 women with a single myoma in group I and 140 with two or more myomas (less than four) in group II.
Presurgical evaluation and preoperative diagnosis were performed in all cases prior to surgery and consisted of abdominal and transvaginal ultrasonographic examination and outpatient hysteroscopy to define clearly the size, location, and number of myomas and exclude additional intracavitary pathologies, that is, endometrial polyps, hyperplasia or malignancy, and adhesions.
Prior to surgery, all women received a standard prophylactic antibiotic dosage of cefazoline 2 g intravenously (i.v.), as previously agreed, to avoid complications (i.e., infections, fever, etc.); all laparoscopic procedures were performed under general anesthesia, with endotracheal intubation; all myomectomies followed a standardized procedure using a four-port approach—one for the laparoscope and three lower quadrant ancillary ports (a 10-mm supra pubic one and two 5 mm, bilaterally).
The women underwent a standardized technique, primarily described by Mais et al. in 1996, 15 performed by the same well-trained residents in referred gynecological centers, which involved hysterotomy, pseudocapsule incision, extracting the myoma by stretching, and uterine suturing.
Before incising the myometrium covering the myoma, a 10 cc solution of glypressine or diluted adrenalin (1/100,000) was injected into the tissue layers, to make tissue ischemia easier and better delineate the cleavage plane and the pseudocapsule.
The laparoscopic intracapsular myomectomy was performed using the following intracapsular technique: the myometrium was incised vertically using a monopolar scalpel after identifying the plane between the pseudocapsule and the myoma.
The purpose of hysterotomy, concerning the length and depth of the uterine incisions, was to expose the myoma pseudocapsule. Thus, the depth of the uterine incision was adapted to localize fibroids in the uterus and to show this surrounding structure, and the length of the incision made was, on average, based on the fibroid diameter. Generally, the length in each group was limited to the length of the myoma downside and the depth of the uterine incisions was only to reach the pseudocapsule.
In cases of polymyomectomy, surgeons incised the myometrium just over each fibroid and, sometimes, used a singular incision to remove more than one myoma; anyway, when it was possible for fibroid location, authors avoid to perform multiple uterine incision, trying to remove multiple fibroids, also of multiple dimensions, by a singular hysterotomy directed to show each fibroid pseudocapsule.
Hysterotomy was followed by exposure of the pseudocapsule and incision. To dissect the pseudocapsule connective bridges from the surrounding myometrium and allow the intracapsular myoma to enucleate, the authors used a monopolar crochet needle or bipolar clamp-scissors (Gyrus PlasmaKinetic AMS), and myoma drills or Collins forceps (Fig. 2). This resulted in the usual opposite traction of the myoma on the surrounding myometrium and promoted its enucleation. The pseudocapsule vascular network small vessels hemostasis was achieved either with simple bipolar electrosurgical forceps or with a bipolar device (Karl Storz) with Vapor Pulse Coagulation (Gyrus PlasmaKinetic AMS), avoiding thermal spread (due to the risk of successive uterine rupture).
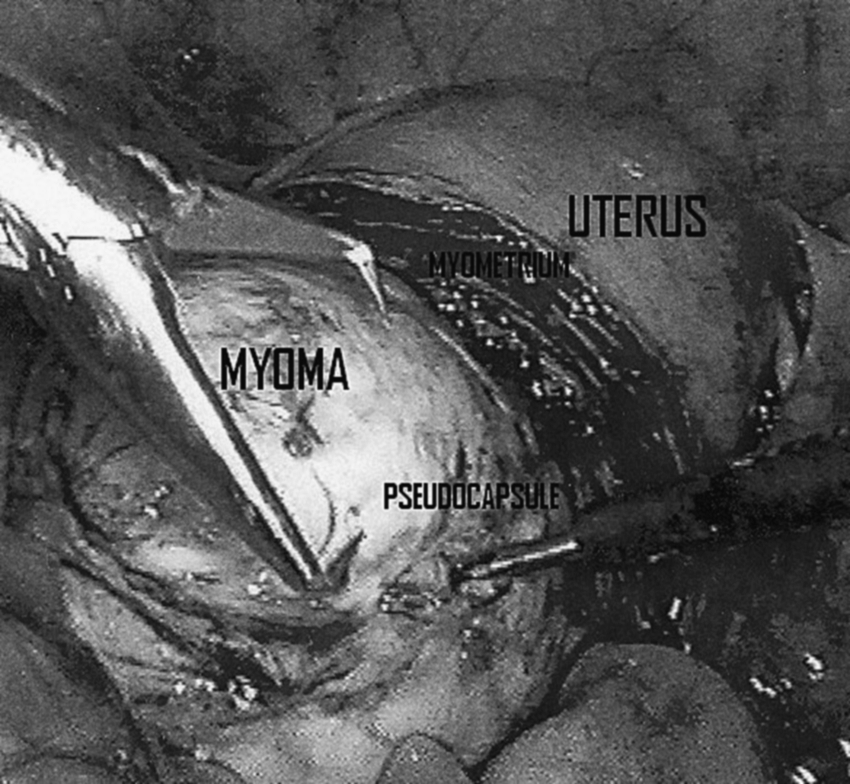
Laparoscopic image of myoma enucleating by intracapsular myomectomy: on the left, myoma is hooked by Collins forceps, and on the right, the pseudocapsule is cut using monopolar Crochet needle, exposing myometrium.
In all procedures, myomas were removed using electrical morcellators (Karl Storz Endoscopy and Gynecare; Johnson & Johnson) and the myometrium was sutured using intra- and extracorporeal single or double stitches, with 0 absorbable poliglecaprone monofilament.
Surgeons approximated the clear edges of the uterine defect (linked to intracapsular method), with intro-flexing single U-stitches, at 1 cm increments; when the myometrial defect was deep or large, it was repaired by suturing with multiple intro-flexing single stitches, followed by serosal repair with multiple intro-flexing single-stitches suturing. Albeit difficult, at times the myometrium required two-layer suturing; sutures were applied at 1 cm increments, using extra- or intracorporeal adequate knot tying, depending on bleeding: extracorporeal for larger bleeding and intracorporeal for smaller. The surgeons decided, a priori, to leave a catheter inside pelvis for postsurgical drainage, to record postsurgical blood loss.
All procedures were based on the following surgical parameters: infiltration into myometrium (number of patients per group), total operating time (in minutes), intrasurgical blood loss (in mL), postsurgical bleeding (mL in drainage), need for painkiller drugs (number of patients per group), postoperative fever (number of patients with fever >38°C after 24 hours and for the first 2 days of hospitalization), postoperative antibiotic administration (number of patients who requested therapy), duration of hospitalization (for 24 or 48 hours), and postoperative clinically significant intramyometrial hematoma >3 cm, 16 as detected by a standard transvaginal ultrasonography before demission. All parameters collected during surgery and hospitalization were recorded and reported in tables by the surgeons involved in the study.
Moreover, patients were annually followed up by the clinicians involved in research, using gynecologic and ultrasonographic exams, for recurrence rate of myomas, pregnancy rate, or delivery outcomes after laparoscopic myomectomies. Dates of follow-up were obtained from patient files and analyzed to report the consecutive number of spontaneous pregnancies, mean time of delivery, type of delivery, Apgar score at I and V minutes, and neonatal weight.
The clinical and instrumental follow-up of patients who requested myomectomy was directed to check and verify the symptoms which they referred before laparoscopic myomectomy; pelvic pain and menorrhagia were investigated in an interview during a gynecologic visit at admission and questioned at postsurgical follow-up, and the patients' answers were reported to clinicians in terms of postmyomectomy pelvic pain and persistence of bleeding disorders.
The results were estimated by an independent reviewer and analyzed using SAS software (version 8); differences in parameters between the two groups were analyzed using the Student's t-test for continuous variables and chi-square tests for nominal variables, considering a P-value of <0.05 as significant, with data presented as mean ± standard deviation or median range.
Results
Over 335 enrolled patients, 1 isolated myomatous nodule and consequent single intracapsular myomectomy was performed out of a total 195 (59.09%) cases; the presence of multiple myomas was detected and, therefore, multiple myomectomies were performed in 140 (42.4%) cases, with a range of 3 ± 1.1.
Symptoms of patients submitted to laparoscopic myomectomy in group I were pelvic pain in 134 patients (68.7%), menorrhagia in 91 patients (46.6%), and ultrasound (US) growth of myomatic nodules in 119 (61.02%); in group II, the same symptoms were reported by 59 (42.1%), 77 (55%), and 73 patients (52.1%), respectively.
Comparison of participants' baseline characteristics did not show statistically significant differences (P < 0.05) (Table 1).
The mean total laparoscopic operating time was 60 ± 7.2 minutes in group I and was significantly longer in group II with 97 ± 8.9 minutes, with P < 0.05 in the Student's t-test analysis.
No statistical differences (P > 0.05) were found in the amount of mean intraoperative blood loss (140 ± 4.7 mL in group I versus 175 ± 6.8 in group II), the catheter inside pelvis for postsurgical drainage (78 women in group I versus 51 in group II), need for painkiller drugs (81 women in group I versus 56 in group II), postoperative fever on 1st hospitalization day (22 patients in group I versus 13 in group II), postoperative antibiotic administration (16 women in group I versus 9 in group II); also in the Student's t-test analysis, no statistical differences (P > 0.05) were found for duration of hospitalization with respect to the number of women discharged in 24 hours (140 women in group I versus 99 in group II) and in 48 hours (55 patients in group I versus 41 in group II), or the detection of postoperative intramyometrial hematoma (>3 cm) with ultrasound, during patient's hospitalization (13 women in group I versus 8 in group II).
No laparoconversion was performed in this study. Normally, all patients leave the operating theater with an analgesic mixture of ketorolac or tramadol in pump; yet, if patients request more analgesic, nurses are accustomed to administer, “on demand,” ketorolac 30 mg i.v., or tramadol 100 mg i.v. in allergic patients (Table 2).
Data are presented as mean ± standard deviation or median range.
There were no significant differences in short-term complications, such as acute anemia (with Hb < 9 g/dL, hematocrit (Hct) < 30 or red cells (RC) < 3,500,000 millions/mm3), postoperative excessive abdominal bleeding (more than 50 mL of blood in the catheter inside pelvis for postsurgical drainage), and urinary tract infections (detected by positive urine culture after Foley removal) between the two groups (Table 3).
The clinical and instrumental follow-up of 3 years was performed in 298 myomectomized patients (90.3%). The transvaginal ultrasound revealed that 29 of 195 women wishing to become pregnant after surgery achieved pregnancies (14.8%) as a secondary outcome. All pregnant women delivered by cesarean section (as a personal choice); 15 pregnancies were observed in group I (7.6%) and 9 in group II (6.4%), with no statistical differences (P > 0.05); the same for mean time of delivery (39 ± 1.8 and 38 ± 6.2), for Apgar score at minute I (9.14 ±0.9 and 9.20 ± 0.5) and minute V (9.78 ± 0.4 and 9.67 ± 0.4), and for neonatal weight (3155 ± 235 and 3240 ± 190 g).
All women became pregnant spontaneously, without assisted fertility techniques or pharmacological preconception treatments for subfertility, and none of the remaining patients decided to receive additional assisted reproductive technology (ART). The rest of the patients preferred to avoid pregnancy, so they had protective sexual rapports during postsurgical follow-up.
Symptoms associated with myomas, which patients presented before laparoscopic myomectomy, such as pelvic pain and bleeding disorders, had improved at follow-up, with a persistence in less than 11% of women. Data collected show the absence of difference in symptoms in both groups (Table 4).
Discussion
These results move from literature dates 4 and they support the author's hypothesis that if a patient is to be submitted to laparoscopical myomectomy, be it singular or multiple, in the same session, the surgical outcome is the same, whether she has one or more subserous and/or intramural fibroids—in terms of intraoperative complications, postoperative compliance, and general surgical feedback.
This happens because of intracapsular myoma enucleation—after dissecting the connective bridges of the pseudocapsule from the surrounding myometrium—which avoids surgical damage to muscular fibers, enables restoration of myometrium integrity, and respects the uterine musculature. 4 Supporting the a priori hypothesis of this study, the myoma pseudocapsule existence was first recognized in 1944, through a description of the vascular system around a fibroid as “a mass of proliferating arteries.” 17 Subsequently, Farrer-Brown in 1970 18 and Awataguchi in 1982 11 found a venous and a vascular plexus, surrounding the periphery of the myoma (Fig. 3). In a recent study, published in 2000, Casey et al. 19 reported significantly higher microvasculature density in the adjacent myometrium compared with small and large myomas, described as a “fire ring” if identified by eco-color Doppler. 10

Histological examination of myoma pseudocapsule, colored by hematoxylin and eosin: detection of vessels and compressed myometrial muscular smooth tissue.
Walocha et al. evaluated the microstructure of the myoma vascular capsule and stated that blood vessel density increases in the immediate surroundings of the myoma, and as it grows in size, new blood vessels penetrate the tumor from its periphery where “the vascular capsule” is being formed, creating a vascular network. 20
Starting from this preliminary anatomical and pathological analysis of the fibroid pseudocapsule existence,4,13,15 the authors of this investigation tested, in the same session, the surgical performance of a single versus a multiple intracapsular laparoscopy, in a group of fertile women affected by subserous and/or intramural myomas and submitted to myomectomy.
The clinical and surgical outcome in the women treated showed that this minimally invasive treatment did not report intraoperative and subsequent long-term complications, with a restitutio ad integrum of uterine anatomy, demonstrated by transvaginal ultrasonography and proved by the excellent follow-up of patients at 3 years.
In fact, the aim of conservative surgery on the uterus, especially in fertile women, must aim at recovering integrity of the skeleton of the extracellular matrix, as the latter ensures the 3D organization of the uterine muscle, which explains why this technique is not accompanied by more bleeding in cases of multiple fibroids extraction compared with single fibroid extraction.
The surgical respect of the proper anatomical entity surrounding myoma, the pseudocapsule, should prevent excessive bleeding when removing single or multiple fibroids.
On the basis of this dogma, in recent years, laparoscopic myomectomy has been considered as the true alternative to laparotomy, with numerous advantages: short hospitalization, decreased need for analgesia, little intraoperative blood loss, and good performance in subsequent pregnancy.21,22
The main important innovation of the endoscopy, in fibroids removal (if necessary with surgery), could be summarized by the magnification of the pseudocapsule and of fibers and blood vessels surrounding the myoma, enabling the surgeon to delicately dissect it, selectively coagulating and cutting this extra-myoma network, thereby enucleating the myoma without damage and respecting the surrounding myometrium.
Discussing the results of laparoscopic myomectomy by intracapsular method, the authors of this article hypothesized the secondary importance of the suture technique on short and late complications, postoperative compliance, and general surgical feedback of treated women. After removing the fibroid from its pseudocapsule, the correct intro-flexing suturing of the hysterotomy, respecting the anatomy of muscle fibers by simply approaching the hysterotomic clear edges (applied at 1 cm increments), in a single or double layer, generally restores the original anatomy of the uterine wall, without leaving hemorrhagic sites or avascular areas.
The risk of uterine rupture after laparoscopic myomectomy is low but still exists and relates to the quality of the uterine scar and the utilization of electrosurgery on the myoma, that is, uterine rupture occurs when the surgical technique is not well performed (for excessive thermal spread) and the preservation of uterine wall vascularization is not maintained. 23
Generally, the risk factors for uterine rupture with subsequent pregnancy, which would be important to analyze, are location of the myomectomy, length of incision, and depth of the incision, and not merely the number of myomata resected.
The authors, in perfecting this method already described in 1996, 15 evaluated and discussed the results, trying to answer the criticisms produced by these operative concepts in understanding and metabolizing.
Primarily, in the study setting, the authors decided to include only patients with subserous and/or intramural fibroids, all located in the uterine body (excluding cervix); to give homogeneity to the intracapsular laparoscopical myomectomy, the authors excluded pedunculated, cervical, and intraligamentary myomas.
Then, on the basis of the anatomical–pathological criteria, 4 the length of the incision made was, on average, based on the fibroid diameter and the depth of the incision was only to reach the pseudocapsule, just to identify the plane between the pseudocapsule and the myoma. In fact, the concept of intramural myomectomy is based on the anatomical entity existence and the myoma-pseudocapsule and in its respecting. 4 So that, the long-term effects of intracapsular myomectomy on the risk of uterine rupture with subsequent pregnancy could be reevaluated in terms of more tailored surgical removal of fibroids. This affirmation should be highlighted by the absence of postmyomectomy clinically symptomatic hematomas 16 —usually detected by ultrasonographic evaluation of myoma sites—in the clinical follow-up of patients. 24
These preliminary data should allow the conclusion that patient appreciation and the feasibility of the techniques used are linked to the preservation of myometrial integrity.
As to pregnancy rates observed in this investigation, the mean age of operated women was between 34.9 ± 2.9 years in group I and 35.6 ± 3.8 years in group II, and this was probably relevant to the nonattainment of pregnancy, even if the women had no medical or surgical complications that might have impaired their fertility rates.
About the bias in the study setup, authors appreciate the nonrandomization, the restricted number and size of fibroids, and the short follow-up for fibroid recurrence rate detection.
Moreover, the laparoscopic procedure was performed at a mean age of 36.5 years, not based on patients' pregnancy wish and not to correct secondary infertility, but to solve clinical symptoms and for a future pregnancy, and so the precise impact of this procedure on fertility after surgery could not be stated.
Even if there are too few pregnancies to draw any conclusion, the authors performed an investigation to evaluate, as first outcome, the surgical outcome of single versus multiple laparoscopic intracapsular myomectomy, in terms of intraoperative complications, postoperative compliance, and general surgical feedback. The effects on pregnancy outcome of this surgical method were reported but only as further dates in the long-term follow-up.
In fact, some patients became incidentally pregnant and this might explain the reason for pregnancy rates below average, related to the fear of a uterine rupture during subsequent pregnancy after myomectomies, in group II. Moreover, it was not possible to test the uterine scars after myomectomy for the personal choice of women to receive a cesarean section, avoiding labor.
Conclusions
Intracapsular laparoscopic myomectomy, performed on single or multiple myomas in the same session, did not show significant differences in terms of intraoperative complications, postoperative compliance, and general surgical feedback, thus enabling recognition of the myoma pseudocapsule during enucleation of fibroids and preservation of uterine scarring. These surgical outcomes may be related to the surgical technique, which respects the anatomy of the benign uterine pathology, focuses on the myoma pseudocapsule, and preserves myometrial integrity, enabling restoration of the uterine musculature. With further consolidation in gynecological surgery by a randomized larger number of women, this laparoscopic method's benefits could be more precisely assessed in terms of myoma recurrence, pregnancy rate, and delivery outcome.
Footnotes
Acknowledgment
The authors thank Prof. Maria Rosaria Buri, Professional Translator/Association Internationale Interprètes de Conférence (AIIC) Conference Interpreter, University Researcher in Translation Studies, for her professional paper revision and editing.
Disclosure Statement
No competing financial interests exist.