
Abstract
Abstract
Introduction:
Since 2001 we minimized access (2.9–4.7 cm) for universally applicable endoscopic hybrid carinatum technique with two transsternal Willital bars in 173 endoscopic hybrid (EH) patients with very satisfactory results. In 2008–2009, endoscopic Nuss bar compression with endoscopic repair of costal flaring applied a new eight-hole stabilizer, which allows the use in pectus carinatum (PC) beyond adolescence including redos and combined deformities. This prospective study of 35 “endoscopic Berlin-Buch reversed Nuss” repairs intends to establish indications for this improved technique.
Materials and Methods:
In February 2008 to February 2010, we used endoscopic Nuss bar compression by applying a bilateral new eight-hole stabilizer fixed to the bar without screws or wires, which allows unprecedented versatility and the use in pectus carinatum beyond adolescence. Thirty-five patients aged 17.05 ± 10.2 years (range: 11.3–33.1 years) were recorded prospectively and followed at 3 monthly intervals. We implanted a standard Nuss bar (11–14′) into an endoscopically dissected submuscular presternal pocket correcting PC by sternal pressure. The bars were put under tension by traction via bilateral eight-hole stabilizers and three pericostal wire sutures on each side. Bars were removed after 2 years.
Results:
All 35 “reversed Nuss” pectus carinatum repairs, including 2 redos after Ravitch, were successful, with no conversion. So far there was no local or general complication and no seroma or bar dislocation. Thirty-one patients judged their result as excellent and 4 as good.
Conclusions:
Although this is a very early experience, “reversed Nuss” is safe and effective and new technical improvements have expanded the range of applicability to older patients and suitable redos.
Introduction
So far minimal access repair of pectus carinatum was limited by the need of an extensive dissection of sternum and entire ventral thoracic cage ranging from one axillary line to the opposite one. Since 2001 we achieved this by bilateral CO2 insufflation of the submuscular space and endoscopic dissection of both serratus and pectoral muscles from the ribs and sternum from xiphoid to jugulum. 6 In the endoscopic hybrid repair for pectus carinatum, the entire dissection was performed endoscopically. Then multiple segmental rib resections and sternotomy were performed under endoscopic assistance in a semi-open way from a 3–5-cm midline (in girls submammar) incision. Two transsternal struts were introduced and fixed pericostally in the same manner. But this was still a very minimized and endoscopically assisted Ravitch-type procedure. By combining this repair with elements of sternal compression, we developed the reversed Nuss using standard Nuss bars and custom-made stabilizers.
Materials and Methods
From February 2008 to February 2010, we treated 35 children and adolescents aged 17.05 ± 10.2 years (age range: 11.3–33.1 years) suffering from severe pectus carinatum by our new Berlin-Buch “reversed Nuss” endoscopic minimal access pectus carinatum repair. Thirty-two patients were male and 3 female; two 33- and 24-year-old men had a redo after unsuccessful Ravitch 17 years ago. All patients were recorded prospectively with a postoperative follow-up of 8–32 months and received a patient-controlled analgesia via an epidural catheter, which was used for about 4 days.
First, the most prominent points of the pectus carinatum (PC) are marked and the best position of the future presternal submuscular bar or the bars is marked with skin markers. For the endoscopic reversed Nuss carinatum repair, we used two high density TV (HDTV) monitors and 30° 5-mm lens for bilateral endoscopy of the submuscular (epicostal) space (Fig. 1). After preoperative single-shot antibiotic coverage, two 5-mm trocars were advanced in a semi-open technique, into the submuscular space below the serratus anterior muscle is entered blindly and insufflated by CO2 at a pressure of 15 mm mercury. A wide pocket is dissected from the ports in a dorsolateral direction using blunt dissection and hook cautery (Fig. 2) as previously described. 6 At some point the two ports were exchanged with the lens now coming from above and the cautery hook from below to extend the dissection. The same dissection was now performed from the left side. Then, a ventral tunnel of roughly the bar's width is dissected from both sides until the two tunnels meet presternally in the midline. Then the chest is inflated by low CO2 pressure of 2–4 mm mercury bilaterally. Wires with attached needles are entered through the port holes into the lateral submuscular spaces. In a line posterior to the posterior axillary line, three different ribs are encircled by the wire suture by an endoscopic needle holder (Fig. 3) and the position of the wires is controlled by submuscular and intrathoracic endoscopy after the lowest trocars have been advanced into both chests. At that point, two 3-cm-long slightly oblique skin incisions are made dorsal to the pectoralis major muscle roughly midway between the anterior and middle axillary line. A long bent clamp is advanced from one skin incision through the subpectoral and presternal tunnel to the opposite one.

Endoscopic access view to the right lateral chest wall by CO2 insufflation below the serratus anterior muscle.

Endoscopic view of the right lateral chest wall by CO2 insufflation below the serratus anterior muscle; note the exact dissection of the ribs and intercostal muscles.
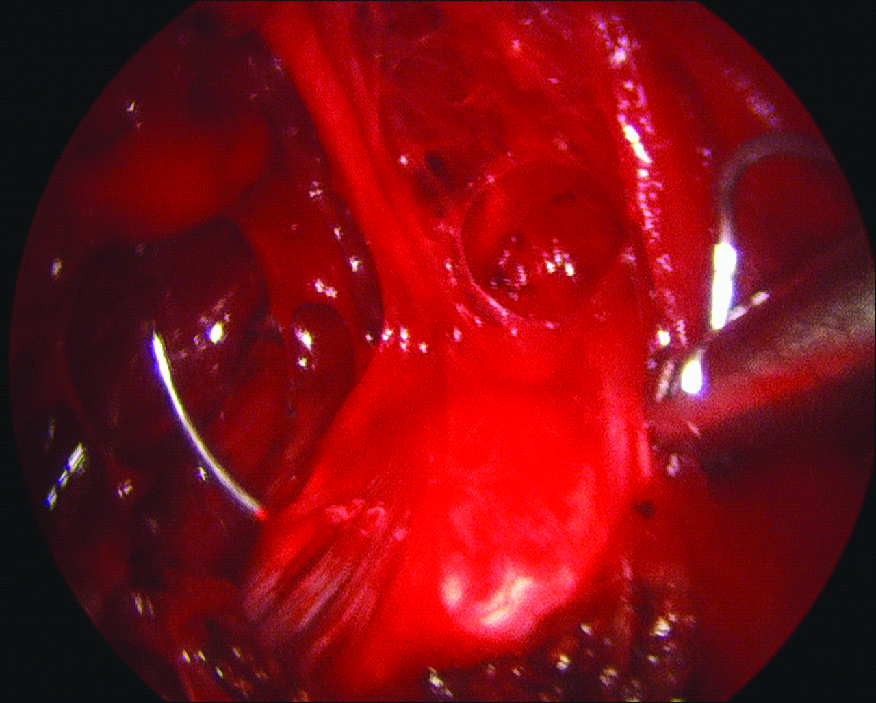
Endoscopic submuscular view of the right dorsolateral chest wall; the needle is passed around the rib by an endoscopic needle driver.
Now the testing bars are laid on the chest and the shortest possible bar is formed by a bar bender to suit the chest with a slight indentation toward the most prominent points of the PC. Now the eight-hole stabilizers are entered through both skin incisions threaded on the bar ends and fixed by over-bending the bar ends toward the chest wall. This technique has been previously published by us for pectus excavatum 1 and proved to be much easier and more versatile than the screws used by Abrahamson. 9 Now the ends of the three pericostal wires are threaded through the end hole of the Nuss bar and through two of the eight holes of the stabilizer (Fig. 4). While the bar is pushed dorsally, the wires are tightened sequentially changing right and left side every time until the prominence of the chest is evened out. Now, under endoscopic sight the medial parasternal part of the bar is fixed to all adjacent ribs by four to six pericostal polydioxanone (PDS) sutures. Finally, prominent costal arches are adjusted to the level of the sternum by partial rib wedge excisions and both chests are controlled by final thoracoscopy for hemorrhage, fixed lung lobes, or pneumothorax. Pneumothorax is evacuated under thoracoscopic sight by suction tubes removed at the end of the procedure. Submuscular suction tubes are introduced, but in case of doubt one or two intrapleural Bülau drains can be left during the postoperative surveillance, although this was exceptionally used in only 2 of the older patients and is not necessary in standard reversed Nuss repairs. Strut removal is planned after 2 years on average (range: 18–30 months), leaving the bar a bit longer in older or redo patients.
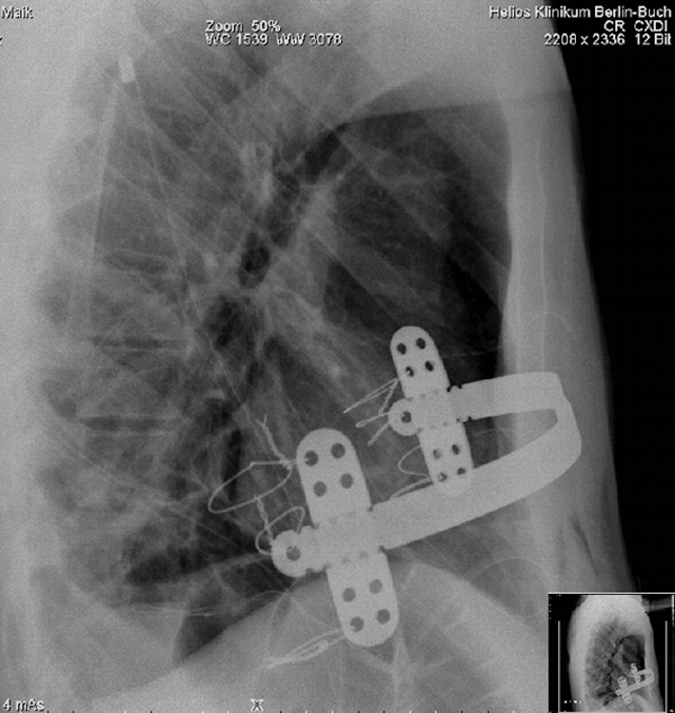
Postoperative lateral X-ray of bar, stabilizers, and the three wire sutures on each side.
Results
From February 2008 to February 2010, the method was successfully employed in 35 children and adolescents.
Thirty-two patients were male and 3 female; two 33- and 24-year-old men had a redo after unsuccessful Ravitch 7–17 years ago. Thirty-five operations could be completed endoscopically in all patients by the described minimal access repair. There was one postoperative seroma managed conservatively.
There was no hemorrhage and no conversion to a large standard access. Operating times came down from initial 180 minutes to 70–130 minutes in the later cases and averaged about 100 minutes except for the older patients and the redos. For safety, all patients had donated a unit of own blood preoperatively, which most received back after the operation. The postoperative course was uncomplicated in all patients, and there was no bar dislocation or need for a reoperation. Thirty-one patients judged their postoperative result as excellent and 4 as good (Figs. 5 and 6); in 3 patients the struts have been removed with no recurrence so far. In our opinion, the results are at least good or better than that with the standard open Hegemann Willital repair and equally good as the minimal access endoscopic hybrid repair used in 173 patients since February 2001.

Patient SM, 14.1 years, suffering from a symptomatic pectus carinatum endoscopic Berlin-Buch “reversed Nuss.”

Patient SM, 14.1 years, at 1 week after endoscopic Berlin-Buch “reversed Nuss” by an 11-inch Nuss bar and two custom-made eight-hole stabilizers, each fixed by three thoracoscopically placed wire sutures to the ribs in the posterior axillary line.
Discussion
During the 3-year period from February 2001 to February 2004, we minimized conventional Hegemann Willital repair to suit accesses below 3 cm and established endoscopic hybrid minimal access repair of pectus carinatum by subpectoral CO2 insufflation, standardized the technique in 37 patients, which is described extensively elsewhere, 6 and continued to use it successfully in more than 170 patients up to now. This technique proved to be universally applicable in every pectus carinatum regardless of age, severity, or the number of failed previous attempts in difficult redos. The only drawback was the necessity of an access on the ventral chest, that is, a short median scar in males or bilateral submammary scars in females.
To avoid this, in 2008 and 2009, we combined our technique with another similar to the ones proposed by Koyobashi in 19977 and Hock or Abramson in 20028,9 but modified dissection by CO2 insufflation of the lateral chest wall below the serratus anterior muscle and below the pectoralis major muscle.
Hock and Abramson had used fairly simple self-made bars made of low-quality material, which never received approval by the European community. Therefore, we modified the use of the well-established and time-honored Nuss bars and got the company to produce special custom-made eight-hole stabilizers for this new application of endoscopic reversed Nuss technique. The sturdy bars allowed more precise modeling and the repair of more severe, older, or redo patients, and the sturdy new stabilizers could be used as levers to exert deliberate torque on the bar if required.
Moreover, the techniques described by Koyobashi 7 and Hock and Abramson8,9 worked only in fairly young patients in puberty (10–16 years) and fairly insignificant deformities, which often were not fully corrected; it was not suited for redo of recurrences and also did not correct deformities of the costal arches such as flaring ribs.
Therefore, we improved our technique and modified the implants to suit older patients up to 33 years, redos, and severe deformities, with the aim to use one implant for all chest deformities regardless of pectus excavatum or carinatum; some costal wedge resection was done in all except the youngest patients. Helios Center for Pediatric and Adolescent Surgery, Berlin-Buch, is a major, supranational reference center for thoracic deformities. During the same 2-year period, 264 Nuss pectus excavatum (PE) repairs (total 1041 Nuss) were performed. In combined PE/PC deformations, both a retrosternal Nuss bar and a presternal reversed Nuss bar are used (“sandwich Nuss” technique).
Berlin-Buch “reversed Nuss,” endoscopic pectus carinatum repair is feasible, safe, effective, and truly a minimal access procedure. Endoscopically assisted minimal access repair of pectus carinatum could be established and standardized.
The results are at least as good as the conventional repair and the hybrid method in young patients; however, this is an early experience and the follow-up is too short.
Footnotes
Acknowledgments
This work was supported by the Sonnenfeld Stiftung (Berlin), Mickey Foundation (Berlin), and McDonald's Kinderhilfe (Munich).
Disclosure Statement
No competing financial interests exist.