
Abstract
Abstract
Purpose:
To analyze indications and to present details of surgical technique and outcomes of thoracoscopic repair for congenital diaphragmatic hernia (CDH) in 139 patients.
Methods:
We reviewed medical records of all patients with CDH who underwent thoracoscopic repair by the same surgical team from June 2001 to October 2009. Patients were placed in the lateral decubitus position. The operations were performed using three trocars. Pleural insufflation with carbon dioxide was maintained at a pressure of 2–6 mm Hg. The hernia defect was repaired using nonabsorbable interrupted sutures with extracorporeal knots. A prosthetic patch was used when direct closure of the hernia defect was not feasible.
Results:
There were 139 patients, including 91 boys and 48 girls. Seventy-five patients were newborns, and 64 were infants or children. The hernia was located on the left side in 113 patients (81.3%) and on the right side in 26 patients (18.7%). The mean operative time for thoracoscopic approach was 66 ± 27 minutes. Conversion was required in 11 patients (7.9%) from 2001 to 2007. There were no conversions in 2008 or 2009. A prosthetic patch was used in 7 patients. There were 14 postoperative deaths (10%). Follow-up was obtained in 114 patients, ranging from 1 to 84 months (mean 26.3 ± 24.7 months). Five patients had recurrence (3.6%).
Conclusions:
Thoracoscopic repair is feasible and safe for children with CDH, including newborns. The conversion rate decreased, and indications increased with surgical team experience.
Introduction
The purpose of this study is to analyze indications and to present details of surgical techniques and outcomes of a thoracoscopic approach for CDH with 139 cases, including 75 newborns.
Materials and Methods
We reviewed medical records of all children with CDH operated by a thoracoscopic approach from June 2001 to October 2009. Indications: From 2001 to 2007, thoracoscopic repair was indicated for infants, toddlers, and selected newborns. The procedure was not indicated for newborns whose condition could not be stabilized with resuscitation and conventional mechanical ventilation or who had associated cardiac anomalies. Beginning in 2008, the surgical indication was extended to newborns whose condition was stabilized with high-frequency oscillatory ventilation (HFOV) and for children with simple associated cardiac anomalies.
Surgical technique
Patients are placed in the lateral decubitus position with the head elevated. The upper arm is left free. Anesthesia with bilateral ventilation is used for newborns, and one-lung ventilation is applied for infants and toddlers. The surgeon stands at the patient's head, with the monitor positioned at the patient's feet. A 5-mm trocar is introduced at the mid-axillary line in the third intercostal space for a thoracoscope, a second 5-mm trocar is placed in the fourth intercostal space anteriorly, and the third 5-mm trocar is inserted in the fourth intercostal space behind the scapular tip. Carbon dioxide insufflation is maintained at a pressure of 2–4 mm Hg in the thoracic cavity. Pressure is increased up to 6 mm Hg if reduction of herniated abdominal organs is difficult. A conventional ventilator with high frequency (from 80 to 100 respirations per minute), and low-peak airway pressure is used for newborns. Since January 2009, HFOV was used for patients who required HFOV preoperatively and could not switch to a conventional ventilator.
After reducing the herniated organs into the abdominal cavity, the hernia defect is repaired using nonabsorbable interrupted sutures (Ethibon 2/0 or 3/0; Ethicon France, Neuilly/Sein, France) encompassing two borders of the diaphragmatic defect with extracorporeal knots. The first stitch is placed at the middle of the hernia defect, and the insufflation is turned off. The anterior rim of the defect is sewn to the thoracic wall if the posterior rim is not present. The two rims of the defect at the posterolateral angle are sewn to the thoracic wall when the defect is large (Fig. 1). A patch (Neuro–Patch manufactured by BBraun Aesculap-Platz, Tutlingen/Germany) is introduced and secured thoracoscopically when required.
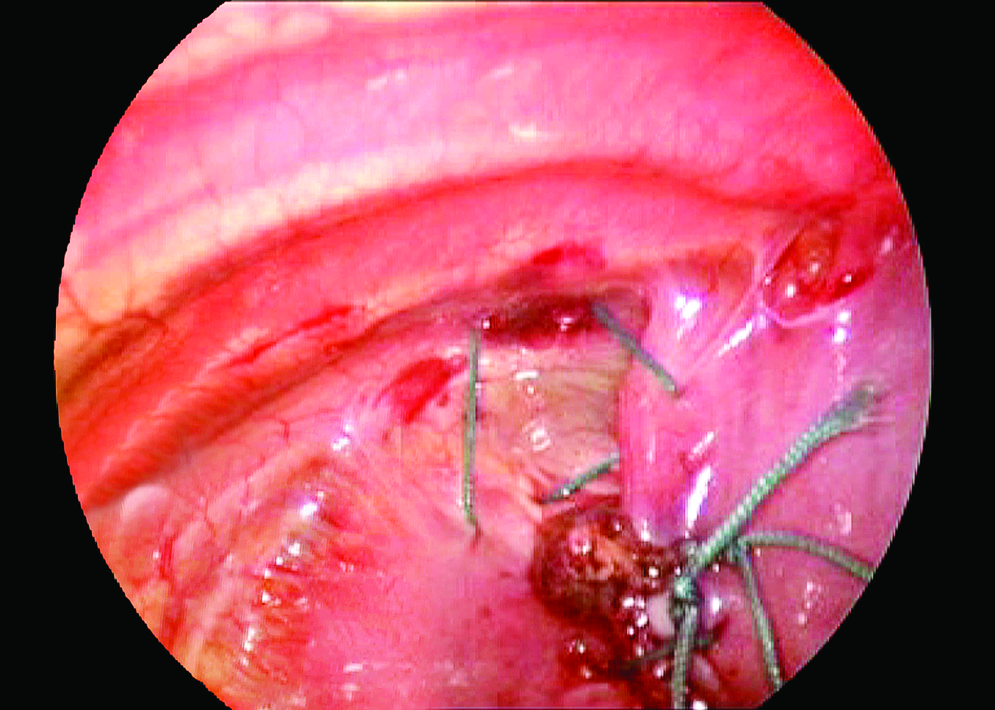
Two rims of the defect at the posterolateral angle are sewn to the thoracic wall.
Results
There were 91 boys and 48 girls. Seventy-five patients were newborns, and 64 patients were infants or toddlers. Preoperative ventilator support was required in 53 patients (38.1%) including 50 newborns and 3 infants. Forty patients required a conventional ventilator, and 13 patients required HFOV. Associated cardiac anomalies included patent ductus arteriosus in 21 patients and atrial septal defect in 1 patient.
Anesthesia with conventional ventilator support was used in 135 patients and with HFOV in 4 patients. Operations were carried out in the operating theater in 135 patients and in intensive care unit (ICU) in 4 patients.
The hernia was located on the left side in 113 patients (81.3%) and on the right side in 26 patients (18.7%). There was a hernia sac in 77 patients (55.4%) and no hernia sac in 62 patients (44.6%). The hernia contents included small intestine in 124 patients, colon in 100 patients, spleen in 41 patients, liver in 26 patients, and stomach in 20 patients. A diaphragmatic incision to widen the hernial orifice was performed in 2 patients.
Conversion to laparotomy was required in 11 patients (7.9%), including 7 newborns and 4 infants. All conversions were performed during the period from 2002 to 2007. No conversion was required in 2008 or 2009. Indications for conversion included a large hernia defect in 3 patients, inability to reduce herniated organs in 3 patients, oxygen desaturation in 2 patients, intestinal adhesions in 2 patients, and pulmonary sequestration in 1 patient.
The diaphragmatic defect was repaired by directly closing 2 hernia borders in 50 patients and by suturing the diaphragmatic border to the thoracic wall in 82 patients. A prosthetic patch was required in 7 patients. The patch was secured thoracospically in 5 patients. In 2 patients, the patch was secured with the diaphragmatic rims and thoracic wall during laparotomy. The hernia sac was plicated in 29 patients and removed partially in 48 cases.
Mean operative time for single thoracoscopic operation was 66 ± 27 minutes (range from 15 to 180 minutes). Thoracoscopic operation plus laparotomy required 97 ± 33 minutes (range from 55 to 180 minutes).
A chest drain was inserted in the first 9 patients and connected to underwater seal. In 128 patients, the drain was connected to a syringe and aspirated manually every 6 hours. There was no chest drain in 2 cases.
There were no intraoperative deaths or complications. Intraoperative blood loss was insignificant. There were 14 postoperative deaths (10%), all of them in newborns. Cause of death included pulmonary arterial hypertention in 8 patients and septicemia in 6. For survivors whose operation was carried out completely by a thoracoscopic approach, mean postoperative stay was 17.3 ± 12.9 days (range 3–91 days). Follow-up was obtained in 114 patients, ranging from 1 to 84 months (mean 26.3 ± 24.7 months). Five patients had recurrence (3.6%).
Discussion
Most surgeons have reported performing the thoracoscopic repair using three trocars. However there are differences in positioning of patients and trocars. Ferreira and Kim et al. placed the first trocar for the thoracoscope below the tip of the scapula. Two other trocars were introduced through the fourth or fifth intercostal space.7,10 Yang placed the first trocar in the anterior axillary line in the fourth intercostal space, and two additional trocars were inserted in the fifth or sixth intercostal space posteriorly and in the sixth or seventh intercostal space below the nipple. 21
We try to place trocars as high as possible. The first trocar is placed in the second or third intercostal space for the thoracoscope, two other trocars are introduced in the fourth intercostal space. With this placement, we always have enough working space to perform operative maneuvers. The working space for surgery would be narrower if trocars were placed at lower levels. This might explain a high conversion rate in some reports.4,7
The hernia defect can be closed with extracorporeal or intracorporeal knots.9,14 We prefer extracorporeal knots, because they can be easily done. After reduction of the hernia contents, we perform the first stitch at the middle of the hernia defect. This stitch can prevent abdominal organs returning to the thoracic cavity, allowing us to turn off the insufflation to avoid further hemodynamic or blood gas disorders due to CO2 pressure.
In our series, two borders of the hernia defect were closed directly together in 36%. We had to close the diaphragm with the thoracic wall in 59%, and used the patch in 5%. The diaphragm is very fragile in newborns. With a large hernia defect, any attempt to close two borders directly together could tear the diaphragm and increase risk of recurrence. The posterolateral angle between the two hernia rims and the thoracic wall is always a weak point, and the defect could not be closed completely in many cases. The remaining defect at this angle might lead to recurrence. To avoid this risk, we always close two rims of the hernia defect with the thoracic wall when direct closure of the two rims is not feasible.
When a patch was required, it was introduced easily through the trocar's incision. The patch was secured to the thoracic wall using a running suture. Interrupted sutures were used on other sides. We performed this suturing without difficulty.
We performed thoracoscopic repair safely in the ICU for 4 patients. We believe that operation in the ICU should be indicated for severe patients at increased risk during transportation to operating theater.
Our results show that thoracoscopic repair is feasible for CDH, not only in children but also in newborns. The conversion rate was not significantly different between newborns and infants or children. Published reports show conversion rates varying from 11% to 42%.4,7,10 Need for conversion may drop with surgical team experience. All conversions in our series were performed before 2008. There were no conversions in 2008 or 2009, whereas indications for thoracoscopic repair were extended to more severe patients. A patch was introduced and secured thoracoscopically in 5 patients in our series, as has been reported by other authors.9,14,19 The need for a patch is no longer an indication for conversion in thoracoscopic repair for CDH.
Oxygen desaturation is a great concern during thoracoscopic repair for CDH, especially in newborns. This leads to conversion or a requirement of high intraoperative peak inspiratory pressure levels.7,10,11,14 HFOV was first successfully used in 1 patient in 2009. 13 This was used for 4 patients in our study. Oxygen saturation and cardiovascular parameters were stable during operation. This new approach could avoid oxygen desaturation and, thus, reduce the rate of conversion. We operated on the patient under HFOV without difficulty.
Inability in reducing herniated abdominal organs has been reported.7,11 We recently overcame this obstacle by increasing PCO2 pressure to 6 mm Hg for a short time combined with maximizing the dose of muscle relaxant. For a small hernia defect, we inspect the orifice and then incise the diaphragm to widen the orifice as needed. To gain adequate space for operative maneuvers, we place trocars at higher levels than some authors.4,10,21 With these modifications, there has been no conversion in our series during 2008 and 2009 due to difficulty in reducing herniated organs.
Before 2008, associated cardiac anomalies were a contraindication for thoracoscopic repair in our series. However since 2008, thoracoscopic repair was safely performed for CDH associated with patent ductus arteriosus or atrial septal defect. Thoracoscopic repair has also been safely carried out by other surgeons for CDH combined with cardiac anomalies.10,14
Presence of the stomach in the thoracic cavity was considered a contraindication for thoracoscopic repair in some reports. 21 In our series, the stomach was present in the thoracic cavity in 20 cases. In 15 of those cases, thoracoscopic repair was successfully carried out. Kim et al. also successfully performed thoracoscopic repair for CDH with the stomach present in the thoracic cavity. 10 The presence of the stomach in the thoracic cavity is no longer a contraindication for thoracoscopic repair for CDH.
There were no intraoperative deaths or complications in our series. This shows that thoracoscopic repair is a safe procedure for CDH both in children and in newborns. There were 14 patients who died postoperatively in our study. The mortality rate was 10%. All patients were newborns. The cause of deaths was pulmonary arterial hypertension in 8 patients and septicemia in 6 patients. Characteristics of those patients are presented in Table 1. This rate is higher than in other series. However, those series included more selected patients.7,9,21
PAH, pulmonary arterial hypertension.
The recurrence rate in our series was 3.6%, lower than in other series.7,9,14 We believe that the closure of two diaphragmatic rims to the thoracic wall at the posterolateral angle is an important factor to prevent recurrence.
In our series, all newborns were operated by the same surgeon. Infants and children were operated by one of 2 senior surgeons. Surgeon experience is associated with recurrence rate, as mentioned by Guner et al. 9
In conclusion, thoracoscopic repair is feasible and safe for CDH. The conversion rate decreased, and indications increased with surgical team experience.
Footnotes
Acknowledgment
The authors thank John Taylor, MD, PhD, from the Department of Pediatrics, School of Medicines at the University of Washington, Seatle, WA, for his careful reading and valuable comments on the manuscript.
Disclosure Statement
No competing financial interests exist.