
Abstract
Abstract
Objective:
To compare orchiopexy by laparoscopy versus traditional surgical technique in patients with an undescended palpable testicle in the inguinal canal.
Materials and Methods:
A prospective, comparative, observational, longitudinal, and double-blind research was done between August 2006 and March 2009 in the Centro de Especialidades Médicas del Estado de Veracruz, “Dr. Rafael Lucio”; 63 patients underwent surgery, age 1–10 years, all with the diagnosis of palpable undescended testicle in the inguinal canal; in 33 patients, the traditional surgical technique and in 30 patients laparoscopy were done. A visual analogue scale (VAS) was used to evaluate post-surgery pain. A testicle ultrasound was practiced before surgery and at 6 months after it.
Results:
The majority of patients were 1–4 years old with a median age of 2.3 years; 51 cases were unilateral and 12 cases were bilateral; 37 testicles were descended with the open traditional surgical technique and 38 through laparoscopy (75 testicles); 44 on the right side and 31 on the left side; there was a hernia associated with 37 undescended testicles, 23 with open surgical technique, and 14 by laparoscopy, without relapsing in any patient. The median surgery time with the open surgical technique was 38 minutes and by laparoscopy, it was 45 minutes. The gobernaculum testis was sectioned by laparoscopy in 23 descended testicles to facilitate the procedure, in the remaining 11 it was not necessary; whereas in the open technique, all the gobernaculum testis were sectioned. In 80% of cases, the laparoscopy caused less pain when compared with the other technique. All patients regardless of the technique used left hospital during the first 24 hours. All have had follow-up for more than 6 months with a median of 18 months, with satisfactory results in relation to size and location of the testicle, with a good ultrasound correlation, and not finding any statistical differences between surgical techniques. There were no accidents with any of the techniques, and 1 patient with the open technique had an important hematoma; hemophilia was later diagnosed in the patient. The esthetical aspect was better with laparoscopy, but the cost was 15% more expensive with the open technique.
Conclusions:
Both techniques had satisfactory results without any significant differences to make us choose one over the other. It is the surgeons' decision based on experience and training on laparoscopy to choose any of the techniques.
Background and Purpose
Introduction
The frequency of cryptorchidism at age 1 is of 0.7%–1%,1,2 being bilateral in 10%–25% of the cases.1,3 Since 1976, when Cortesi performed the first laparoscopy for the diagnosis of intrabdominal bilateral cryptorchidism, 4 there have been many articles reporting the advantages and benefits of this approach for no palpable testis;5–8 however, there are few publications related to the usefulness of laparoscopy in palpable undescended testes.9,10 Considering the backgrounds of the utility of laparoscopy in undescended testes independent of being palpable or not, a prospective study was done with palpable undescended testis by a surgeon with experience in both techniques making an analysis of both procedures. This was the first related comparative report.
Materials and Methods
From August 2006 to March 2009 in the Medical Specialty center “DR RAFAEL LUCIO,” 63 patients (75 testes) from 1 to 10 years old in whom palpable undescended testis was diagnosed were surgically treated: 33 patients (37 testes) with the traditional surgical technique and 30 patients (38 testes) by means of laparoscopy. Ultrasounds were performed on all of them before surgery and 6 months after surgery. A visual analogue scale (VAS) assessed pain intensity through facial expression and was used to assess postoperative pain, and the cost for both procedures was documented.
Surgical technique
The patient recumbent with mild Trendelenburg position and placed in lateral position opposite the side of the affected testicle, a 5-mm port and two-sided 5 mm or 3 mm ports were placed depending on the age of the patient. The surgeon places himself at the opposite side of the affected testicle. It starts a dissection medial and lateral of spermatic vessels leaving the peritoneum to cover the vessels (Fig. 1) temporarily with the intention of pulling it to facilitate the dissection of the vessels and vas deferens at the level of inguinal canal and to introduce the testis to the abdominal cavity if necessary, thus avoiding pinching and damaging the vessels (Fig. 2). When the dissection is manually completed, the testis of the inguinal canal is descended into the scrotum where it is attached in the traditional manner. In case the testis cannot be manually descended, it is taken to the abdominal cavity and the gubernaculum is sectioned. On the port of the affected side, a dissector clamp is inserted, taken through the inguinal canal, and then exteriorized through the scrotum (Fig. 3); it serves as a guide to pass a 5 mm port through the scrotum (Fig. 4), which avoids injuring the epigastric vessels; then, the gubernaculum is taken, and the testis is descended and fixed. In patients who had associated hernia, no maneuvers were performed to repair it.

Dissection medial and lateral of spermatic vessels.
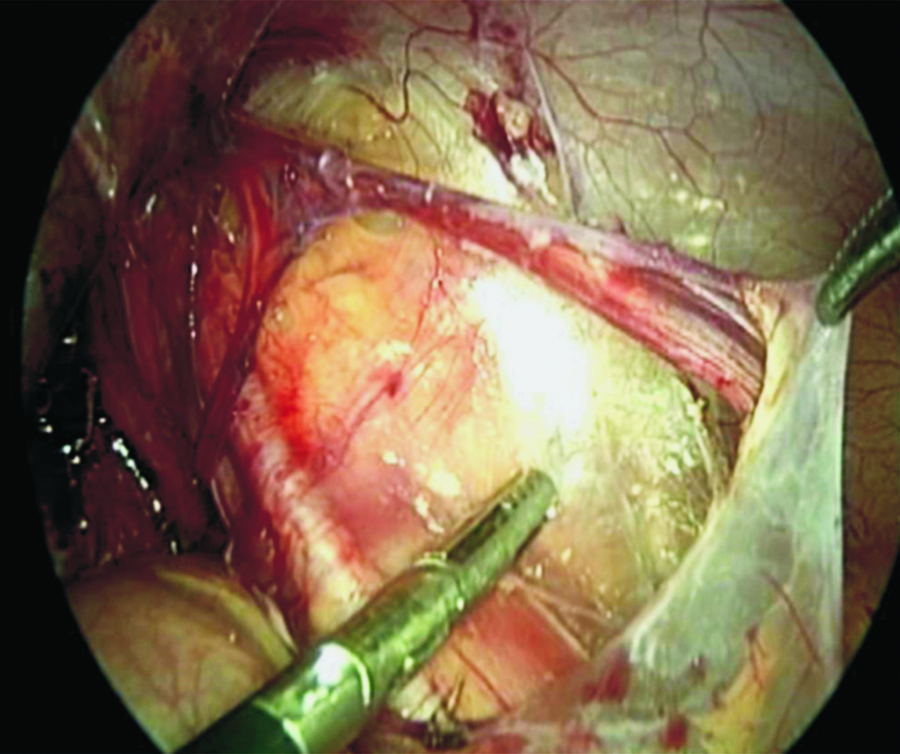
Leaving the peritoneum to facilitate the dissection of the vessels and vas deferens.

Dissector clamp is taken through the inguinal canal and then exteriorized through the scrotum.

Five-millimeter port is passed through the scrotum, the gubernaculum is taken, and the testis is descended and fixed.
Results
The majority of patients were 1–4 years old with a median age of 2.3 years; 51 cases were unilateral, and 12 cases were bilateral; 37 testicles were descended with the open traditional surgical technique and 38 through laparoscopy (75 testicles); 44 on the right side and 31 on the left side; there was a hernia associated with 37 undescended testicles, 23 with open surgical technique, and 14 by laparoscopy, without relapsing in any patient. The median surgery time with the open surgical technique was 38 minutes and by laparoscopy, it was 45 minutes. The gubernaculum testis was sectioned by laparoscopy in 23 descended testicles to facilitate the procedure, in the remaining 11 it was not necessary because it was manually descended; whereas in the open technique, all the gubernaculum testis were sectioned. In 80% of cases, the laparoscopy caused less pain when compared with the other technique. All patients regardless of the technique used left hospital during the first 24 hours. All have had follow-up for more than 6 months with a median of 18 months, with satisfactory results in relation to size and location of the testicle, with a good ultrasound correlation, and not finding any statistical differences between surgical techniques. There were no accidents with any of the techniques, and 1 patient with the open technique had an important hematoma; hemophilia was later diagnosed in the patient. The esthetical aspect was better with laparoscopy, but the cost was 15% more expensive with the laparoscopy technique.
Since it was manually descended. Generally speaking, they were patients with a testis distally placed.
Discussion
There are advantages and disadvantages of both surgical techniques: the open technique requires further dissection of the inguinal region and when the testis is located in a high position, maneuvers are performed rather blindly and with some difficulty when the dissection is close to the pole of the kidney, a situation that does not occur in the laparoscopic approach where we also have a magnified image.9,10 The relative disadvantage of the laparoscopic approach is that the surgeon should have training and experience in this type of approach. The surgeons who participated in this study, in addition to working as a team, had extensive experience in these procedures, which explains the negligible rate of complications.
We reported the usefulness of the laparoscopic approach in palpable testes in high position,9,10 as is in any level of the inguinal canal. 10 We included all patients no matter what level were the testis located, finding that those distally located were feasible to manually descend (Fig. 2), avoiding to bring the testis into the abdominal cavity with the consequent excision of the gobernaculum testis; this implies a proper dissection element in the path of the inguinal canal. We consider it advisable to temporarily leave the peritoneum covering the spermatic vessels (Fig. 1), which pulling it facilitates the dissection just mentioned and avoids pinching and damaging the vessels.
It describes the passage of the port of the scrotum to the abdominal cavity below the epigastric vessels, which carries the risk of injury to the vessels with consequent bleeding; 10 we prefer to pass a clamp from the port on the affected side (Fig. 3) and move it above the epigastric vessel through the inguinal canal and externalized through the scrotum to guide the port from the scrotum. It is a quick and safe move to avoid passing through the inguinal canal floor without having to be an impediment to properly descend the testis; this is understandable, because they are palpable as compared with intra-abdominal testes where a Prentiss maneuver may be required (step medial to the epigastric vessels).
Similar to other authors,9,10 in the cases of hernia associated with the vaginal process, it was adequately dissected and no repair of the hernia was necessary regardless of the size of the defect; and in no case, we had recurrences.
Conclusion
With both techniques, we had satisfactory results without any significant difference to favor one, so it is up to the surgeon training and experience to use the proper surgical technique.
Footnotes
Disclosure Statement
No competing financial interests exist.