
Abstract
Abstract
Purpose:
To examine our experience of laparoscopic pyeloplasty for the treatment of ureteropelvic junction obstruction (UPJO) in the pediatric population.
Methods:
From November 2001 to June 2009, 112 patients underwent transperitoneal laparoscopic pyeloplasty for the treatment of symptomatic or radiographic UPJO. Data were collected retrospectively. Patients were followed at regular intervals with imaging and symptom assessment. Failure was defined as inability to complete the intended procedure, persistent flank pain, radiographic evidence of obstruction, or the need for definitive adjunctive procedures.
Results:
Mean patient age was 9.4 years (0.2–20.5 years), and follow-up was available on all 112 patients with a mean duration of 15.3 months (0.6–84.5 months). There was one open conversion in the series. Mean operative time was 254 minutes (102–525 minutes). There was one minor intraoperative complication reported (0.8%). There were 12 (10.8%) postoperative complications; most were relatively minor with complete resolution and without long-term sequelae. Postoperative ultrasonography has been performed in 102 patients, with 99 (97%) patients demonstrating improvement of the UPJO. Three patients (3%) continued to have symptomatic and/or radiographic evidence of obstruction that necessitated the need for adjunctive procedures, which included laser endopyelotomy in 2 patients, and a re-do open pyeloplastiy in 1 patient. Of those cases that were completed laparoscopicaly, the overall success rate was 97.2%.
Conclusions:
Laparoscopic pyeloplasty for UPJO in the pediatric population is technically challenging; however, with experience, one can expect excellent success rates comparable to open pyeloplasty, with minor complications with reasonable operative times.
Introduction
Laparoscopic pyeloplasty was first described in the adult population by Schuessler et al. in 1993. 3 The technique was designed to emulate the open operation.1,3 Initial and long-term success rates have been comparable for laparoscopic and open pyeloplasty in the adult population.1,3–8 Nevertheless, acceptance of pediatric urologic laparoscopic pyeloplasty has generally lagged behind when compared to its adult counterpart. This is in large part due to the nature of the practice of pediatric urology. 9 Fortunately, there has been a shift in the paradigm. Pediatric laparoscopy has recently benefited from improvement in equipment and technology, as well as an increase in experienced laparoscopic surgeons entering the field. The techniques that were developed in adults have been refined for the pediatric population, allowing for the expansion of the technique.
Pediatric laparoscopic pyeloplasty was first described by Peters in 1995. 4 Since this initial publication, a variety of techniques and approaches have been described and utilized. Success rates and surgical outcomes for laparoscopic pyeloplasty have been found to be equivalent to the open procedure,10–13 and additional advantages include less incisional discomfort, a quicker convalescence, and excellent surgical cosmesis. Disadvantages of the procedure include a significant learning curve, and cost.1,4 In this study, we describe the evolution of our technique, and results achieved with selective application of laparoscopic pyeloplasty in the pediatric population.
Materials and Methods
From November 2001 to June 2009, 112 patients underwent transperitoneal laparoscopic pyeloplasty for the treatment of symptomatic or radiographic UPJO. Data were collected retrospectively. Patients were followed at regular intervals with imaging and symptom assessment. Failure was defined as inability to complete the intended procedure, persistent flank pain, radiographic evidence of obstruction, or the need for definitive adjunctive procedures.
The technique is as follows. All procedures were performed transperitonealy. At the beginning of the procedure, rigid cystoscopy with a retrograde pyelogram of the affected side is performed. A guidewire is placed into the renal pelvis under fluoroscopic guidance, and secured in a sterile manner. The guidewire is useful in identifying the ureter for a transmesenteric approach on the left side, and for manipulation of the ureter during reconstruction. As the series progressed, most patients had a double pigtail ureteral stent placed at this point in the procedure, often with a guidewire alongside the stent for manipulation. Alternatively, simply placing an appropriate length double pigtail stent cystoscopically before the laparoscopic portion of the procedure suffices in both intraoperative ureteral intubation and postoperative drainage. The patient is placed in a 45° flank position. We do not believe an axillary roll is necessary in the pediatric patient if the child is properly positioned and supported with neither pressure or stretch placed on the axilla. A gel pad is used in its place. Access is obtained with open placement of a 5 mm radially dilating umbilical port. Two accessory 3- or 5-mm ports are placed, depending on patient size. One is in the mid-epigastrum, and the other in the lower abdomen in the mid-clavicular line ipsilateral to the affected kidney. For left-sided procedures, the ureteropelvic junction (UPJ) is accessed via a transmesenteric approach in most cases (Fig. 1), and on the right, access is gained from mobilizing the colon to the level of the hepatic flexure. After the UPJ has been dissected clear of the surrounding tissues (Fig. 2), complete transection and excision of the abnormal segment can be performed. Dissection can be aided by early placement of an anterior pelvic stay suture through the anterior abdominal wall. If there is no crossing vessel, the pelvis can be divided just above the UPJ to leave a handle of distal pelvis on the ureter. If there are crossing vessels, the pelvis is exposed above the vessels, and the space behind the vessels is developed. The ureter may be divided just below the UPJ, and then the UPJ is lifted anterior to the vessels for anastomosis. The ureter is spatulated laterally (Fig. 3), and intracorpeal suturing using 5-0 or 6-0 absorbable suture is performed to anastomose the two segments (Fig. 4). An indwelling double pigtail ureteral stent is placed before completion of the anastomosis, if not at the beginning of the procedure. A Foley catheter has been left overnight in all of these cases, but may not be necessary. In general, the patient stays overnight in the hospital. The stent is removed 2–4 weeks postoperatively.
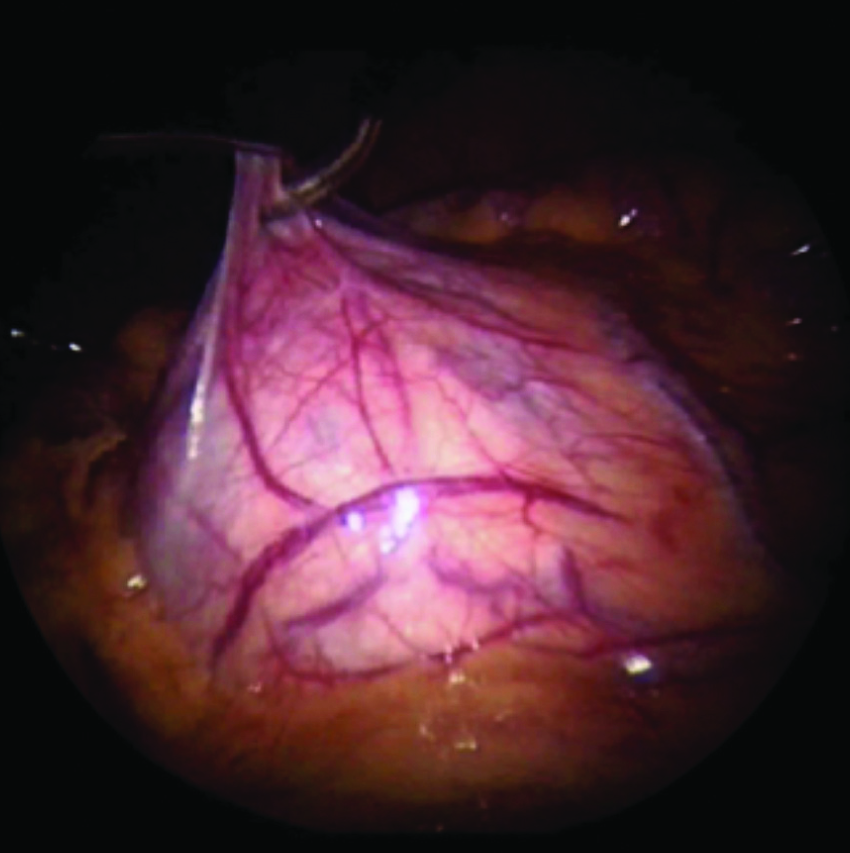
Obtaining access to left ureteropelvic junction obstruction (UPJO). The laparoscopic instrument is tenting up the mesentery with the UPJO visible underneath.
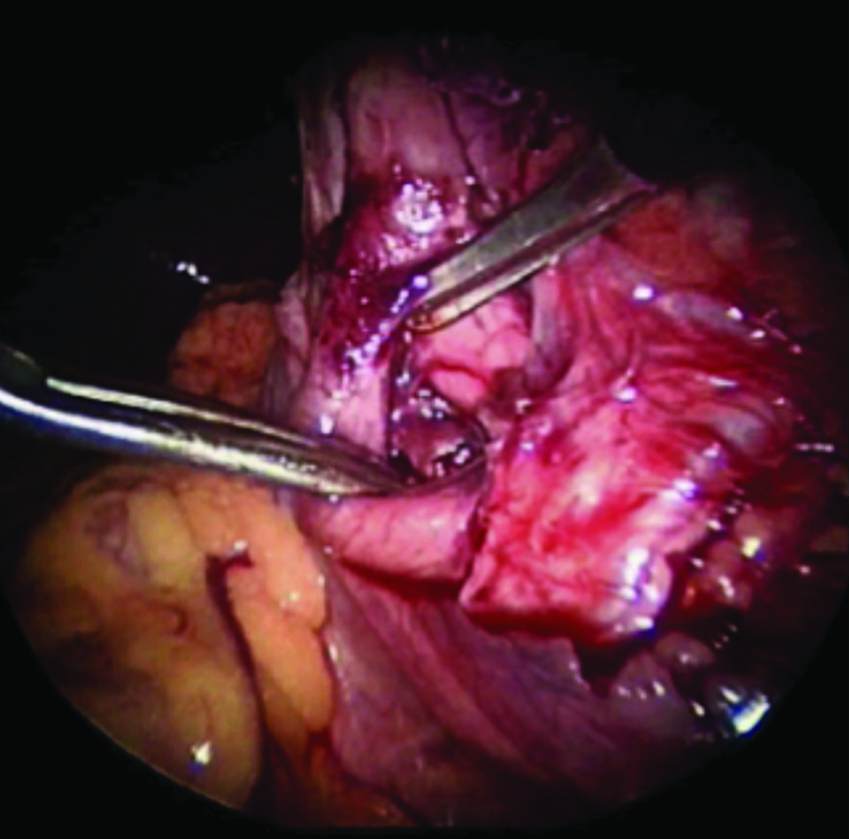
Exposure of the UPJO before dismemberment.
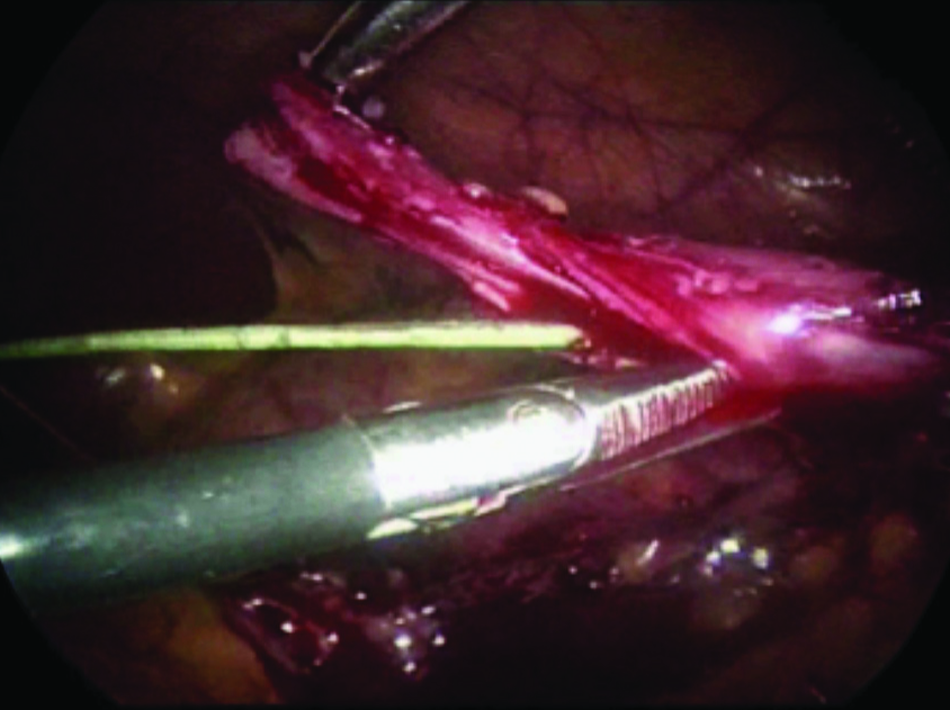
Spatulation of the ureter after dismemberment. Guidewire is visible through the proximal ureter.
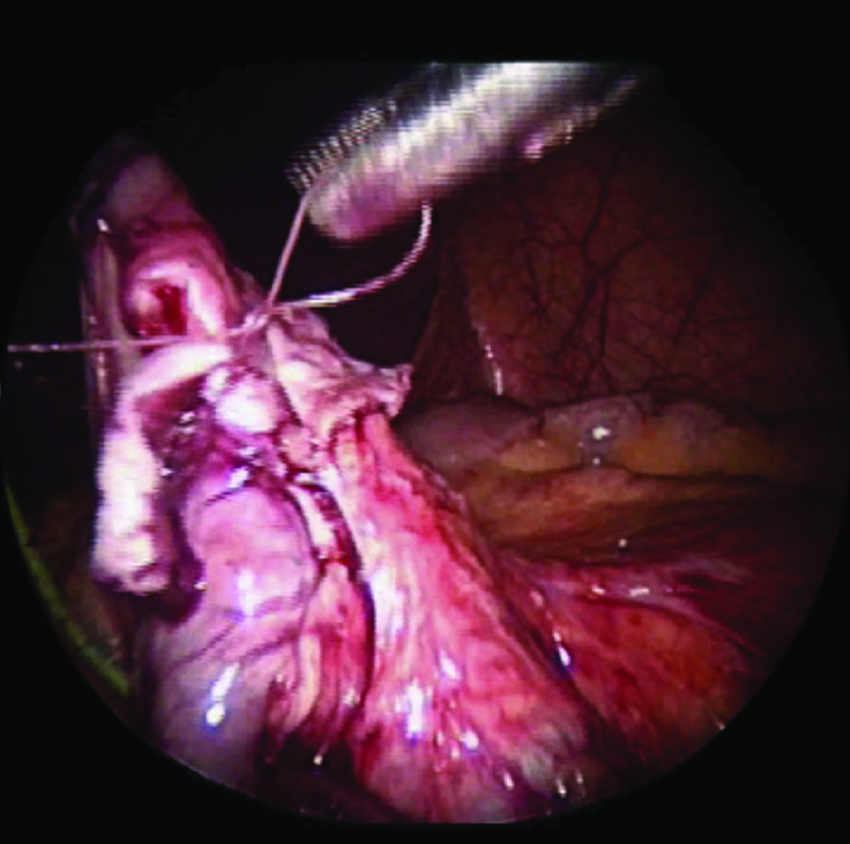
Intracorporeal suturing of the anastomosis with 6-0 absorbable suture.
Results
Transperitoneal laparoscopic pyeloplasty for UPJO was performed in 112 patients. Mean patient age was 9.4 years (0.2–20.5 years), and follow-up was available on all 112 patients with a mean duration of 15.3 months (0.6–84.5 months) (Table 1). Procedures performed included 99 laparoscopic Anderson–Hynes pyeloplasties, 4 laparoscopic Heineke–Mikulicz pyeloplasties, 3 laparoscopic Anderson–Hynes pyeloplasties with concomitant ureteroscopy, 1 laparoscopic pyeloureterostomy, 1 laparoscopic lower-pole dismembered pyeloplasty, 1 laparoscopic Heineke–Mikulicz with concomitant vesselpexy, 1 laparoscopic Anderson–Hynes pyeloplasty with concomitant appendectomy, and 1 laparoscopic Anderson–Hynes pyeloplasty with concomitant vesselpexy (Table 2). There was one open conversion in the series, for an open conversion rate of 0.8% (Table 3). Mean operative time was 254 minutes (102–525 minutes). Eighteen patients had either a preoperative stent or nephrostomy tube, and 1 patient had a previous laparoscopic pyeloplasty. A crossing vessel was present in 52 (46%) patients. Mean length of stay was 1.3 days (1–5 days). There was one intraoperative complication reported (0.8%), which resolved with out any long-term sequelae. There were 12 (10.8%) postoperative complications; most were relatively minor with complete resolution without long-term sequelae (Table 4). Postoperative ultrasonography has been performed in 102 patients, with 99 (97%) patients demonstrating improvement of the UPJO. Three patients (3%) continued to have symptomatic and/or radiographic evidence of obstruction that necessitated the need for adjunctive procedures, which included laser endopyelotomy in 2 patients, and a re-do open pyeloplastiy in 1 patient. Of those cases that were completed laparoscopicaly, the overall success rate was 97.2% (Table 5).
Discussion
UPJO is the most common cause of hydronephrosis in newborns and young children, and open pyeloplasty has been the gold-standard treatment of this entity for decades. In contemporary series, success rates for the open technique are >90%.1,4–6 Laparoscopic pyeloplasty is an accepted surgical standard for the treatment of UPJO in the adult population. Success rates in the literature for adult laparoscopic pyeloplasty range from 88% to 98%.8,10–13 Recently, Jarrett et al. demonstrated that the long-term success rates for laparoscopic pyeloplasty in adults are equivalent to the open approach. 1
Acceptance of laparoscopic pyeloplasty in children has lagged behind when compared to its adult counterpart. As Peters et al. described, this phenomenon is partly due to the nature of the practice of pediatric urology, with an emphasis on reconstructive procedures and relatively little exposure to laparoscopy. 9 Suture-assist devices, often used in adult pyeloplasty, are not suitable for reconstruction in children, and hand sewing with fine suture is technically demanding. In addition, infants and young children experience less postoperative morbidity, and thus there is less incentive and demand for minimally invasive procedures. Finally, traditional open operations performed through a small flank incision, have such high success rates, that there has been a reluctance to subject pediatric patients to procedures that might be less successful.
Tan et al. reported the first pediatric series of transperitoneal laparoscopic dismembered pyeloplasty in 1999, and since that time a variety of techniques and approaches have been described. 13 The transperitoneal, retroperitoneal, and robotic approaches have all been reported, with advocates for each procedure. Although there is a theoretical risk of intra-abdominal injury while performing a transabdominal technique, in fact this is rare. 14 Advocates of the retroperitoneal approach have suggested an easier dissection 14 ; however, there is less working space in the retroperitoneum, often making the procedure difficult in smaller children and infants, and there is some question as to whether crossing vessels are more easily missed. Robot-assisted laparoscopic pyeloplasty has also been described and allows 3D observation and 6° of wrist movement, making suturing more intuitive and lowering the learning curve. 15 However, the overall cost of equipment and training is much higher with use of the robot, and the technology is not universally available. In the end, the approach used should be based on the experience and comfort of the operating surgeon.
The overall success rate in our series using a transperitoneal approach was 97.2%. This is comparable to what has been reported in the literature for the adult population, and compares favorably to the results of traditional open pyeloplasty.1,8 As stated previously, no significant intraoperative or postoperative complications occurred, and all patients were discharged on postoperative day 1 or 2, tolerating a regular diet. Although not studied here, there appears to be a subjective benefit in convalescence, excellent cosmetic outcome (Fig. 5) for older children and adolescents.

Postoperative appearance of laparoscopic incisions 6 months after surgery.
Disadvantages to the procedure are related to the technical difficulty of the laparoscopic technique. There is a fairly steep learning curve that is associated early on with long operative times, and there is the need for advanced laparoscopic skills. This series has demonstrated that operative times eventually compare favorably to open surgery.
Our series of transperitoneal laparoscopic pyeloplasty in children is unique because it is one of the largest series to date in the literature. In addition to our excellent overall success rate, this series also highlights the evolution of our technique, which helped us overcome the difficult and steep learning curve associated with the procedure. Laparoscopic pyeloplasty has become our preferred method of correcting UPJO in children at our institution.
Conclusion
The spectrum of laparoscopic urological surgery in children continues to expand, although it still lags behind its adult counterparts. Procedures such as laparoscopic pyeloplasty have only recently been introduced and have been primarily available at centers with advanced laparoscopic experience.
Laparoscopic pyeloplasty for UPJO in the pediatric population is technically challenging; however, with experience, excellent success rates with few complications and reasonable operative times can be expected. Results are consistent with those for open pyeloplasty, with potentially less postoperative incisional discomfort, a quicker convalescence and an excellent cosmetic outcome. In experienced hands, laparoscopic pyeloplasty should be considered an accepted technique for repair of UPJO. As the field continues to evolve with improvement in technology, and surgeons entering the profession with basic laparoscopic backgrounds, pediatric urologic laparoscopy will also continue to progress. It is our hope that minimally invasive approaches to urologic conditions, such as UPJO, will become more available to children in the near future.
Footnotes
Disclosure Statement
No competing financial interests exist.