
Abstract
Abstract
Aim:
Laparoscopic Kasai portoenterostomy (LKPE) is generally regarded to have a poorer outcome than open Kasai portoenterostomy for the surgical treatment of uncorrectable biliary atresia. We will describe our LKPE as the only center using laparoscopy to perform Kasai portoenterostomy in Japan.
Techniques:
For our LKPE, a 5-mm trocar is placed in the epigastrium in addition to conventional trocar placement. A Ligasure device is inserted through this additional trocar to seal portal vein branches at the porta hepatis draining into the caudate lobe, instead of hook diathermy that is used universally elsewhere because there is an unacceptably high risk for lateral thermal injury to microbile ducts. We minimize porta hepatic microbile duct injury during anastomosis between the Roux-en-Y jejunum and the liver parenchyma around the transected biliary remnant by not suturing where the original right and left bile ducts were present and making sutures deliberately shallow but deep enough to prevent leakage. Our anastomosis is more central to the porta hepatis, like the original Kasai, compared with “extensive lateral dissection” commonly performed elsewhere in Japan. The length of the Roux-en-Y jejunal limb should be individualized, not predetermined to be 30, 40, or 50 cm as is common practice; the jejuno-jejunostomy should fit naturally into the splenic flexure, otherwise the redundant limb may become tortuous as the patient grows, causing bile stasis and possible cholangitis.
Conclusions:
Our LKPE can be performed safely and successfully with encouraging outcome.
Introduction
Materials and Methods
We treated 5 patients with UCBA using our LKPE: mean age at surgery was 74 days (54, 56, 70, 72, and 119 days, respectively) and mean weight at surgery was 4.7 kg (range: 4.4–5.0 kg). One of the coauthors (A.Y.) performed all surgeries.
Surgical technique
Dissection of the biliary remnants and port hepatis
The procedure is performed under general anesthesia with the patient positioned at the foot of the operating table, the surgeon at the patient's feet, an assistant with a camera at the surgeon's left, and an assistant on the right. Conventionally placed trocars are used initially. A 10-mm trocar is inserted supraumbilically using open Hasson's technique. A 30-degree 5- or 10-mm laparoscope is used. Three additional trocars are then placed under laparoscopic control—two 5-mm trocars on either side of the upper quadrant port and another 5-mm trocar on the left of the paraumbilical port. To elevate the liver to improve exposure at the porta hepatitis, a percutaneous suture introduced just below the xiphoid process is used to snare the round and falciform ligaments and retract the liver; other percutaneous transhepatic stay sutures are then introduced into the left lobe and into the right lobe. Hook diathermy and tissue forceps are used to dissect the cystic duct and the mid to distal biliary remnant, and then the fibrotic biliary remnant is transected distally at the superior border of the duodenum. The distal end of the biliary remnant is elevated to enable portal structures, that is, the right and left hepatic arteries and the bifurcation of the main portal vein to be visualized clearly. For this visualization, a Ligasure device (Valley Lab, Boulder, CO) is used. The Ligasure device is inserted through an extra 5-mm trocar placed in the epigastrium and used to dissect the biliary remnant and divide portal vein branches at the porta hepatis draining into the caudate lobe (Fig. 1), to minimize lateral thermal injury to microbile ducts, because the Ligasure device generates much less heat laterally. 7
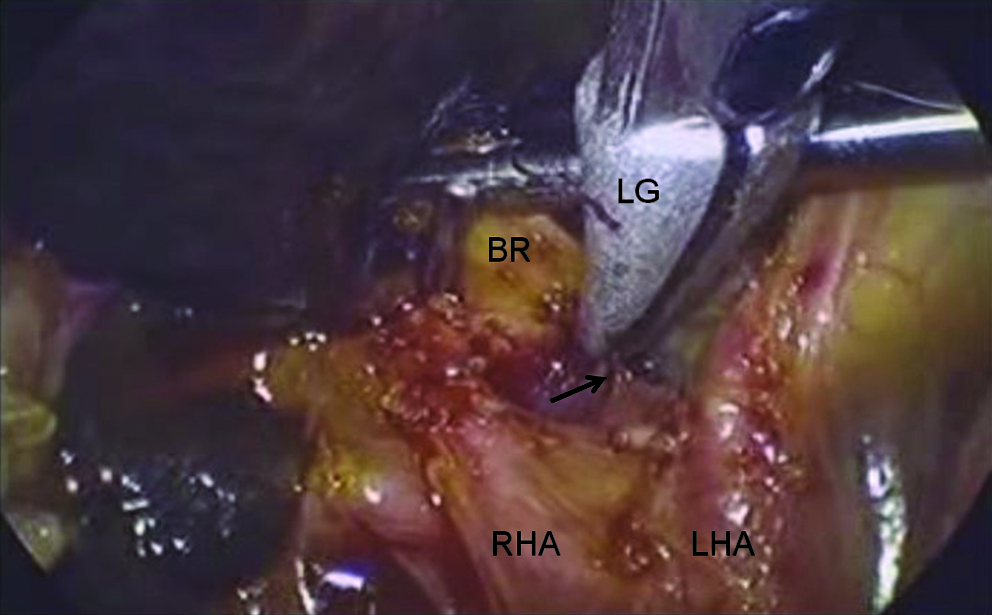
A Ligasure device inserted through an extra 5-mm trocar placed in the epigastrium being used to dissect the biliary remnant and divide portal vein branches (arrow) at the porta hepatis draining into the caudate lobe. BR, biliary remnant; LG, Ligasure device; LHA, left hepatic artery; RHA, right hepatic artery.
Extracorporeal transumbilical jejunal Roux-en-Y
The ligament of Treitz was identified and the jejunum 15 cm distal of ligament was exteriorized through the umbilical port site to create a Roux-en-Y jejunal loop extracorporeally. The length of the Roux-en-Y limb was determined by placing the jejunum loop at the umbilicus and bringing the distal end of the limb up to 3 cm above the xiphoid process, to give a jejuno-jejunostomy that fits naturally into the splenic flexure after anastomosis. The Roux-en-Y jejunal limb is approximated to the native jejunum for 8 cm cranially to prevent intestinal contents of the native jejunum into the Roux-en-Y limb (Fig. 2). An antimesentric enterotomy, 10 mm in length, for portoenterostomy was made very near the closed end of the Roux-en-Y limb and the jejunum returned to the abdominal cavity. The closed end of the jejunal limb was brought up via a retrocolic window to the portal hepatis.

The length of the Roux-en-Y limb is determined by placing the jejunal loop at the umbilicus and bringing the distal end (E) of the limb to be 3 cm above the xiphoid process. The jejuno-jejunostomy (arrowheads) will then fit naturally into the splenic flexure after anastomosis. Arrows show approximating the Roux-Y limb to the native jejunum for 8 cm cranially to streamline flow into the distal jejunum and eliminate reflux into the Roux-Y limb and prevent stasis in the Roux-en-Y limb.
Portoenterostomy
We minimize porta hepatic microbile duct injury during portoenterostomy anastomosis between the Roux-en-Y jejunum and the liver parenchyma around the transected biliary remnant by not suturing at 2 and 10 o'clock, where the original right and left bile ducts were present, or if there was risk for anastomotic leakage, connective tissue at the porta hepatis was sutured to the Roux-en-Y jejunum at 2 and 10 o'clock, not to the liver parenchyma itself. Sutures for the anastomosis were deliberately shallow but deep enough to prevent leakage (Fig. 3).

Sutures (arrows) at the anastomosis are deliberately shallow but deep enough to prevent leakage, and no sutures are placed where the original right and left bile ducts were present, at 2 and 10 o'clock. T-BR, transected biliary remnant.
Results
Outcome was successful in all cases, without any intraoperative complications and no conversions to OKPE. Mean duration of surgery was 9.1 hours. Mean intraoperative blood loss was minimal (6 mL). All were jaundice free (total bilirubin: <1.5 mg/dL) within 2 months of surgery. After a mean follow-up of 16.0 months, 3 remain jaundice free, but 1 had liver transplantation at 10 months postoperatively because of three attacks of cholangitis and some liver cirrhosis, although total bilirubin at the time of transplantation was 2.5 mg/dL. Transplantation proceeded smoothly because of minimal intra-abdominal adhesions.
Discussion
Kasai portoenterostomy revolutionized surgical management of UCBA when it was introduced by Professor Kasai in 1959, and Kasai portoenterostomy has been widely accepted as the standard surgical treatment for UCBA. In the original OKPE performed by Professor Kasai himself, transection of the biliary remnant was not deep, and the right and left biliary remnants remain connected by fibrotic connective tissue, which could contain microbile ducts. His sutures for the anastomosis between the raw surface of the biliary remnant and the jejunum also appear to be deliberately “shallow” to avoid damage to patent microbile ducts, especially at 2 and 10 o'clock, where the original right and left bile ducts were present. Many Japanese pediatric surgeons tried modifying the original OKPE to improve results, 8 and the anastomosis at the porta hepatis was extended laterally to become wider than the original OKPE. Although LKPE is technically challenging for even experienced pediatric surgeons, the authors believe that if the original concepts of OKPE as derived from an operative video of Professor Kasai himself performing OKPE are adopted, then the anastomosis at the porta hepatitis is possible laparoscopically. In fact, we strongly feel that the extended wide portoenterostomy anastomosis commonly performed in Japan cannot be performed laparoscopically, and if transection is too deep, the liver parenchyma comes between the right and left biliary remnants and they are separated, which could further disrupt microbile duct distribution.
During our LKPE, we did not transect the biliary remnant deeply as Professor Kasai did, resulting in that the portoenterostomy anastomosis is not wide, allowing us to perform portoenterostomy laparoscopically. Also, we tried not to place sutures for the portoenterostomy anastomosis at 2 and 10 o'clock.
When dissecting the fibrotic biliary remnant, special attention must be given to the small vertical branches of the portal vein that drain into the caudate lobe. Most surgeons use high-power hook diathermy to divide the portal vein with unacceptable lateral thermal injury. For our LKPE, we use a Ligasure device to minimize lateral thermal injury to microbile ducts, but an additional 5-mm trocar is needed in the epigastrium. This trocar allows a Ligasure device to be used safely without damaging surrounding tissues and contribute to decreasing the incidence of portal vein complications such as thrombosis, which can be caused by lateral thermal energy.
Many surgeons predetermine the length of the Roux-en-Y limb to be 30, 40, or 50 cm, irrespective of the size of the child. This causes redundancy of the Roux-en-Y limb, because as the child grows, the Roux-en-Y limb also grows and can become tortuous, causing bile stasis and possible cholangitis. It is important to make the Roux-en-Y limb fit the size of the child, as we have described previously, 9 so the jejuno-jejunostomy fits naturally into the splenic flexure after the anastomosis is completed. Also, a conventional T-shaped jejuno-jejunostomy may cause bile stasis due to reflux. This can be prevented by approximating the Roux-en-Y limb to the native jejunum for 8 cm cranially to streamline flow into the distal jejunum and eliminate reflux into the Roux-Y limb and prevent stasis in the Roux-en-Y limb.
We were able to perform our LKPE safely and successfully in all cases, although the time required for LKPE was longer compared with conventional OKPE. However, we expect that operative time will improve as there is a learning curve associated with any new procedure. Although the number of cases in this series is small and follow-up is limited, our initial results would indicate that our LKPE is as effective or may even be better than conventional OKPE based on reports in literature.10,11 More cases and longer follow-up will allow us to modify our LKPE, so that it can be considered as a valid alternative to OKPE for the surgical treatment of UCBA.
Footnotes
Acknowledgment
This work was supported by a Japanese Foundation for Research and Promotion of Endoscopy grant.
Disclosure Statement
No competing financial interests exist.
This paper was presented at the 19th Annual Congress of the International Pediatric Endosurgery Group, June 8–12, 2010, in Waikoloa, Hawaii.